
Abstract
Purpose:
Gastropexy during laparoscopic gastrostomy tube (GT) insertion can be technically challenging. T-fasteners are an effective method of gastropexy. However, the use of external bolsters requires an additional procedure for removal and may cause skin complications due to pressure necrosis. We describe our experience utilizing T-fasteners in a novel way that eliminates external bolsters during laparoscopic GT placement.
Methods:
Pediatric patients requiring enteral access who underwent gastrostomy at a single institution using the paired T-fastener technique were reviewed. Gastropexy was achieved by passing pairs of T-fasteners, under laparoscopic and/or endoscopic guidance, through single stab incisions into the stomach in a square configuration, allowing the suture from one T-fastener to be tied subcutaneously to its paired suture. This eliminates the need for external bolsters. Operative time and 30-day postoperative complications, including local wound infection, granulation tissue formation, bleeding, and tube replacement, are reported.
Results:
Thirty patients underwent gastrostomy placement using the paired T-fastener technique. Mean age was 9.2 years (standard deviation [SD] 6.9) and mean weight 29.9 kg (SD 21.0). Mean tube length was 2.2 cm (SD 0.71). Eight patients underwent an additional procedure at the time of gastrostomy. Mean operative time was 74.4 minutes (SD 39.7). Five patients developed a local wound infection requiring antibiotics. Five developed granulation tissue. Seven patients underwent tube replacement within 30 days for dislodgment or stem upsize.
Conclusion:
The paired T-fastener technique is a safe and efficient method for primary button gastrostomy placement. This method eliminates the need for additional trocars or external bolsters and may be helpful in patients with thick abdominal walls.
Introduction
Gastrostomy tube (GT) placement is a common procedure to allow delivery of enteral nutrition. Children may require long-term enteral access for a variety of conditions, including neurological disorders, failure to thrive, and malnutrition. 1 GTs can be placed using several different surgical techniques. Percutaneous endoscopic gastrostomy (PEG) and laparoscopic gastrostomy have become the favored approaches in children, with unique advantages and limitations to each approach. PEG placement avoids additional abdominal incisions and is readily performed regardless of patient abdominal wall thickness, although it does require adjunct maneuvers to allow primary low-profile—or button—gastrostomy placement. The laparoscopic approach has been shown to have fewer major complications, including gastrocolic fistula formation, than PEG in pediatric patients.2,3 In addition, PEG tube exchange can be distressing to children and often requires sedation, whereas balloon-containing button tubes can be easily replaced. 4 For these reasons, laparoscopic primary button GT placement has become an increasingly popular approach for long-term enteral access in pediatric patients.
A key step in the placement of a primary button gastrostomy is the creation of a gastropexy, which allows the surgeon to dilate and advance the tube through the abdominal wall with gastric counter-tension. 5 In addition, a secure gastropexy affords a degree of safety in the event of early tube dislodgment, reducing the risk of gastrocutaneous fistula disruption. There are various suture techniques available to perform laparoscopic gastropexy to secure the stomach to the anterior abdominal wall to allow for GT placement, including T-fasteners, purse string sutures, and U-stitches. 6 Although each technique has potential advantages and disadvantages, the local skin complications associated with T-fastener bolsters has limited their use in pediatric patients. We hypothesized that a modified T-fastener technique in which the external bolsters are not required could eliminate the risk of bolster-related skin complications, whereas providing equivalent gastropexy outcomes when compared with other techniques.
Methods
Pediatric patients requiring enteral access who underwent laparoscopic GT placement using the paired T-fastener technique for gastropexy at a single institution from 06/01/2019 to 01/31/2021 were reviewed after Boston Children's Hospital Institutional Review Board approval. All GT placements were performed by pediatric surgeons. Patient demographics as well as operative details, including operative time, GT size, use of endoscopy, and additional concurrent procedures at the time of GT placement such as central line placement or urological procedures, were recorded. Prior abdominal surgery is defined as any prior procedure that involved laparoscopy or laparotomy. Outcomes included 30-day postoperative complications, including local wound infection, granulation tissue formation, bleeding, and need for tube replacement, were recorded.
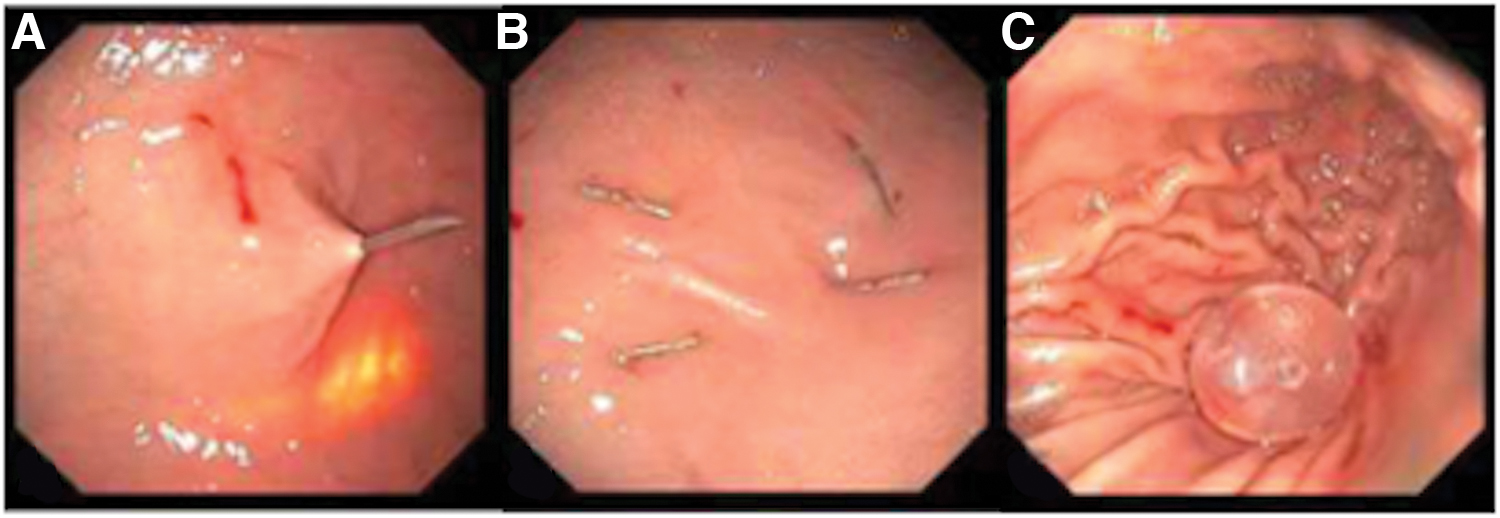
A standardized technique was used by all surgeons for the study period. Initial peritoneal access was obtained through a transumbilical trocar (Fig. 1). The stomach was inspected to determine the optimal site for GT placement. Gastropexy was achieved by passing pairs of T-fasteners (Avanos Medical, Inc., Alpharetta, GA) under laparoscopic visualization, with or without endoscopic guidance, through the fascia and stomach wall in a square configuration around the planned site of the GT (Fig. 2). The T-fastener consists of a metal anchor attached to an absorbable monofilament polydioxanone suture. Each pair was passed through a single skin stab incision to allow each pair of absorbable sutures to be tied and buried subcutaneously. An additional incision was made centered between the four T-fasteners to accommodate the GT. The stomach was then accessed through this incision with an introducer needle and the GT was placed through Seldinger technique, using the T-fasteners to provide gastric counter-tension to allow dilation of the tract and advancement of the button GT (Applied Medical Technologies, Inc., Brecksville, OH). Intraluminal placement of the GT was confirmed through laparoscopy in all but one case where endoscopy was used (Fig. 3). The paired absorbable sutures were then tied after removing the external bolsters, burying the knots within the subcutaneous tissue.
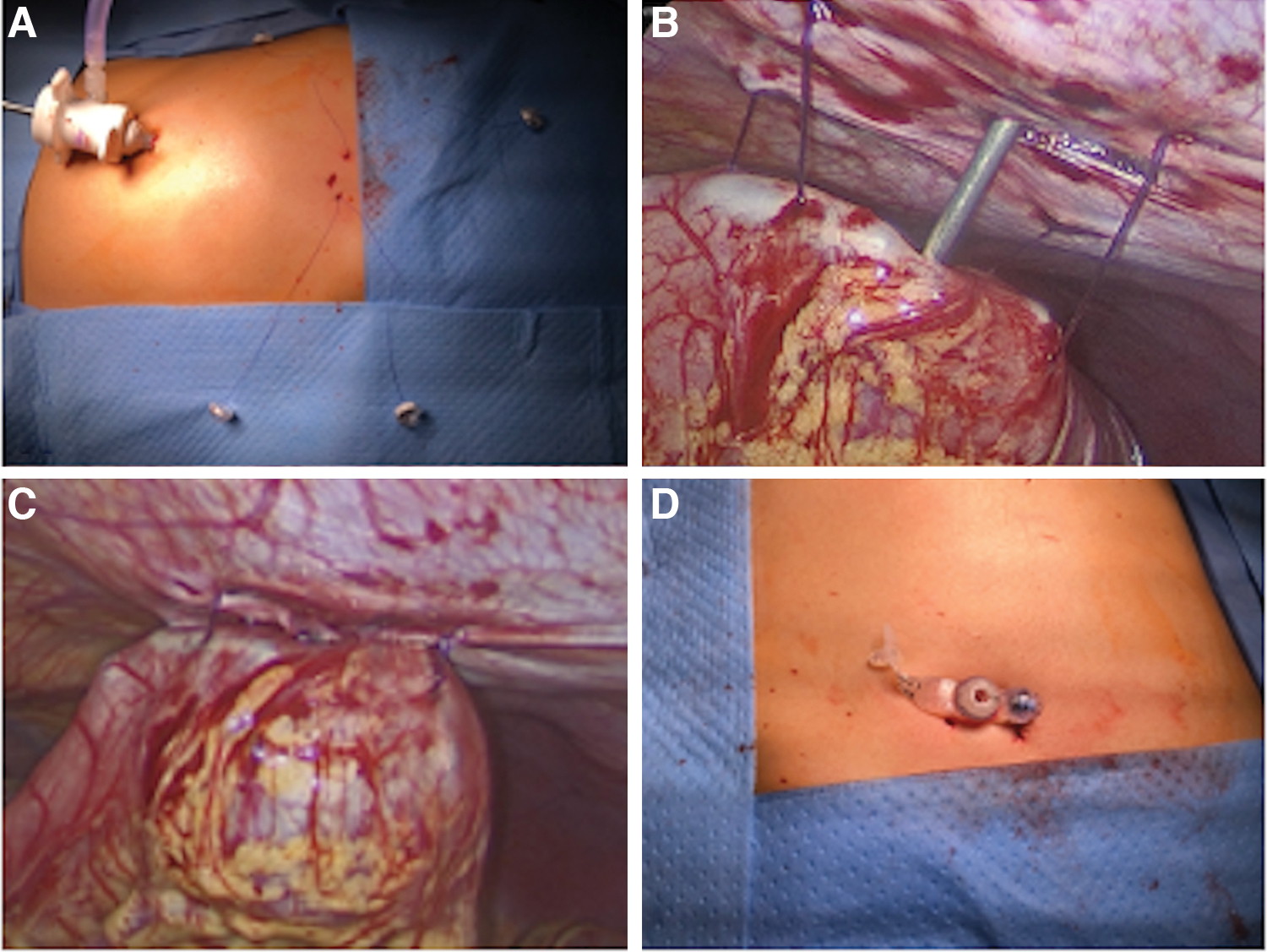
Operative images:
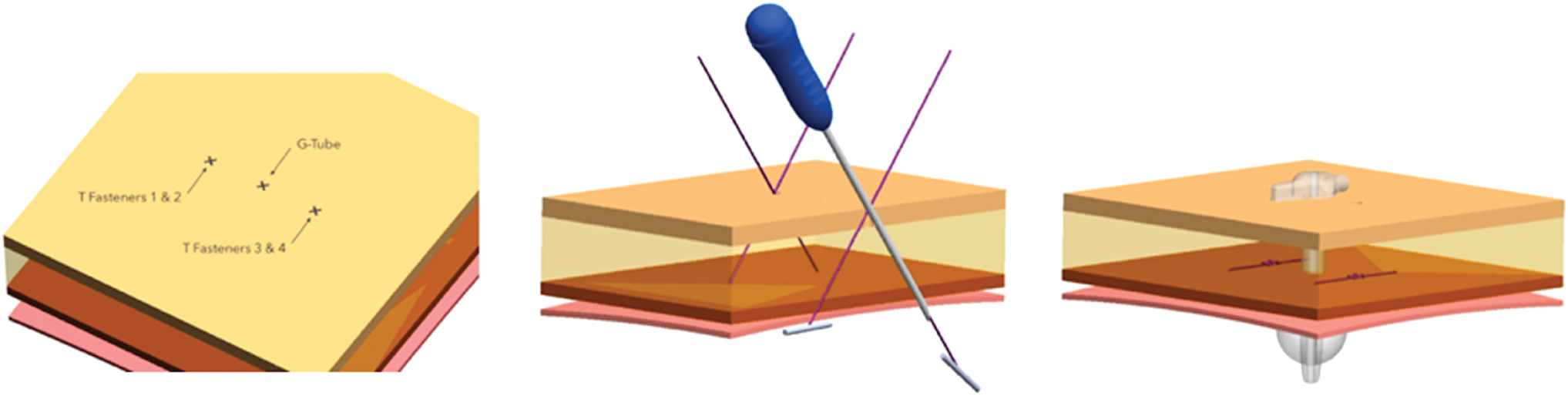
Schematic of T-fastener and GT configuration. GT, gastrostomy tube. Color images are available online.
Results
Patients
A total of 30 patients underwent minimally invasive gastropexy during enteral tube placement using the paired T-fastener technique. Two patients (6.7%) had a gastrojejunostomy (GJ) feeding tube placed, and the remainder underwent GT placement. Six patients had prior abdominal surgery. The mean age was 9.2 years (standard deviation [SD] 6.86) and mean weight 29.9 kg (SD 21.0). The mean body mass index was 18.8 kg/m2 (SD 5.7). The most common indication for long-term enteral access was neurological condition 14 (46.7%) (Table 1).
Patient Demographics and Indication for Enteral Access
Operative
Mean operative time was 74.4 minutes (SD 39.7, range 35–197 minutes). Eight patients (26.7%) had an additional procedure performed at the time of operation. Additional procedures included three endoscopies, one port placement, one urological procedure, one lung resection, one take down of gastrocutaneous fistula, and one bronchoscopy. For patients undergoing an additional procedure, mean operative time was 95.9 minutes (SD 56.7). Patients undergoing gastrostomy or GJ tube placement alone had a mean operative time of 66.6 minutes (SD 29.5). Tube diameter ranged from 12 to 16 Fr, median 14 Fr. Tube length ranged from 1.5 to 4.0 cm, mean 2.2 cm (SD 0.7). Twenty-seven (90%) patients underwent single port placement. One patient underwent endoscopic placement, without the use of a laparoscope. Of the 2 patients who had GJ tube placement, one had a total of three trocars placed to facilitate the takedown of a previous gastrocutaneous fistula (Table 2).
Operative Details Including Number of Trocars, Operative Time, and Feeding Tube Dimensions
Additional procedures included three endoscopies, one port placement, one urological procedure, one lung resection, one take down of gastrocutaneous fistula, and one bronchoscopy.
SD, standard deviation.
Complications
Within 30 days of follow-up, 5 patients (16.6%) had a local wound infection that required antibiotic treatment. Two of these patients were immunocompromised. Five (16.6%) patients developed granulation tissue that required treatment with silver nitrate or cauterization. No patients developed an infection requiring drainage or reoperation and there were no cases of peritonitis, or other intra-abdominal infection. No significant postoperative bleeding occurred. Three (10%) patients required tube replacement due to early unplanned dislodgment. Four (13.3%) patients had their tube exchanged due to malfunction or need for upsize. All were replaced successfully with the gastropexy noted to be intact (Table 3).
Thirty-Day Complications
Discussion
Laparoscopic tube gastrostomy placement remains a common procedure among children. This series describes our experience using T-fasteners without external bolsters to perform gastropexy during minimally invasive tube gastrostomy placement. We find this technique to be an efficient and secure method for gastropexy. There are several technical advantages offered by this method. A single trocar placed in the umbilicus provides adequate access to the peritoneal cavity and produces a good cosmetic result. A direct view of the stomach allows the surgeon to identify the ideal GT location and visualize the gastropexy. The T-fasteners allow excellent counter-tension on the stomach to allow dilation and transabdominal advancement of a primary button gastrostomy. The paired T-fastener technique eliminates the discomfort and pressure associated skin injury that often occurs with bolsters and eliminates the need for bolster or suture removal following the procedure. This is especially important in children, where suture removal or further tube manipulation can be particularly distressing.
A number of techniques for optimal gastropexy during GT placement have been described previously. Although the U stich is a commonly used technique, the use of T-fasteners has been proposed for patients with thick abdominal walls.6,7 Intracorporeal Stamm sutures have also been described; however, this can be a technically challenging laparoscopically. 8 Alternatively, nonabsorbable sutures may be used to create a temporary gastropexy, which are initially tied to the tube or skin and removed following the procedure. Mason et al. have also described a technique in which absorbable sutures are tied in the subcutaneous space. 9 Although often more technically challenging to place, subcutaneous sutures can eliminate the risk of pressure necrosis and skin erosion seen with external suture fixation and external bolster devices. 10 This benefit is also seen with the subcutaneous U-stitch, but we believe the modified T-fastener technique to be technically easier, especially in patients with a thick abdominal wall. In our experience, the transabdominal U-stitch technique becomes increasingly difficult above a thickness of 2 cm without the addition of an additional port, and it is for these patients where we have preferentially used this technique. This is demonstrated by the mean tube length of 2.2 cm, with a range up to 4.0 cm, which suggests patients in our institution in which this novel technique was employed had thicker abdominal walls.
There were no major complications reported among our patient cohort and no patients required hospital readmission due to procedure-related complications. Our rate of tube dislodgment (10%) was similar to rates reported in prior studies. In these studies, dislodgment rates ranged from 1.5% to 27.7%.2,5,11–13 Among studies using a similar technique to ours, with subcutaneous suture for gastropexy, a 7% rate of dislodgment is reported compared with our rate of 10%. 9 Sutherland et al. also performed a comparison of GTs placed by PEG, T-fasteners, and subcutaneous absorbable sutures. They found that T-fasteners had the lowest rates of dislodgment at a rate of 1.8% compared with 3.7% with transfascial subcutaneous sutures and 14% with PEG tubes. 11 Although our T-fasteners dislodgment rate is higher, we found an intact gastropexy among all patients who required tube replacement for dislodgment, which suggests that no case of tube dislodgment was a direct result of T-fastener failure. Thus, we believe our technique offers a secure gastropexy.
The rate of granulation tissue formation (17%) was lower than other studies that have reported granulation tissue rates ranging from 23.5% to 60.8%.2,6,11–13 Among T-fastener cases, granulation tissue was reported in 47.3% compared with 17% in our study, both of which are less than the reported 60.8% of subcutaneous suture cases. 11 In a previous study comparing the U-stitch technique to T-fasteners, a higher rate of granulation tissue was found in the U-stitch group. 7 No patients required surgical excision of granulation tissue in our series.
The infection rate in our series is higher than that reported by Petrosyan et al., who reported an infection rate of 2.5% in subcutaneous suture gastropexies, as well as Mason et al., who reported a 10.3% infection rate in their series of 301 patients who underwent gastropexy with subcutaneous U-stitch.9,10 Importantly, all patients responded to antibiotics and none required additional procedures such as incision and drainage. Since this technique was preferentially used on patients with thick abdominal walls, it is possible that the obese patients with thick abdominal walls in this patient cohort were more prone to infection. Three patients (10%) required elective tube exchange for upsizing. This may reflect the challenge of accurately measuring the stem length for primary button GTs in patients with thick abdominal walls, especially while in supine position.
There are several limitations to this study. It is a single-center study and thus the results of this cohort may not be generalizable to other institutions. The number of patients (30) represents a relatively small cohort and thus precludes subgroup analysis. The decision to use this technique was left to the individual surgeon, potentially contributing to selection bias. A prospective study with a larger patient population and randomization may help to better determine the efficacy of the paired T-fastener technique for gastropexy when compared with other commonly used techniques.
In conclusion, the paired T-fastener technique allows for simple and secure gastropexy during minimally invasive GT insertion and may be particularly useful in patients with thick abdominal walls.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work is funded in part by the Chairman's Fellowship, Department of Surgery, Boston Children's Hospital.