
Abstract
Objective:
Chronic appendicitis (CA) is a diagnosis characterized by long-standing right lower quadrant pain. We analyzed clinical, morphological, and immunohistochemical studies of the appendix to confirm the adequacy of surgery for CA in children with chronic right lower quadrant pain.
Patients and Methods:
We carried out comparative studies of clinical presentations and results of morphological and immunohistochemical studies of remote appendicitis in 55 children with chronic recurrent lower quadrant pain (CRLQP).
Results:
Morphological and immunohistochemical studies revealed three types of changes in the appendix. Type 1 (n = 21)—chronic inflammation. Inflammatory leukocyte infiltration was localized within the mucous membrane of the appendix. An immunohistochemical study revealed a significant (P < .01) increase in the expression of CD106 (vascular cell adhesion molecule 1) and in the number of matrix metalloproteinase 9 (MMP-9) positive cells. Type 2 (n = 20)—lymphoid hyperplasia. Morphological changes were characterized by lymphoid infiltration of the mucosa and submucosa of the appendix. Immunological changes were characterized by an increase (P < .01) in the expression and number of MMP-9, expression of CD106 positive cells, an increase in the expression of collagen IIIα in combination with a decrease in the expression and number of positive vascular endothelial growth factor (VEGF) and vasoactive intestinal peptide cells. Type 3 (n = 12)—catarrhal inflammation. Morphological changes were characterized by impaired blood circulation only in the mucous membrane, without destructive or inflammatory changes. Immunological changes were characterized by an increase (P < .01) in the expression and number of VEGF-positive cells, which may indicate a response to local hypoxia of the appendix and explain neovascularization in a chronic condition. The abdominal syndrome after appendectomy was noted to disappear in 89% of patients. The established changes in remote appendicitis, other than acute inflammation, make it possible to consider reasonable appendectomy a way of treating CRLQP in children.
Conclusions:
We have identified immunohistochemical and morphological changes pointing to autoimmune and vascular mechanisms of appendix damage in children with CRLQP. Laparoscopic appendectomy helps to eliminate abdominal pain in most CA patients.
Introduction
Abdominal pain is a most common presentation in children. Diagnostic and therapeutic approaches to acute appendicitis (AA) are clearly defined and do not present difficulty in most cases.1,2 Chronic appendicitis (CA) is a rare condition; the rate of its occurrence is 1.5%–3% of all cases of recurrent abdominal pain characterized by long-standing right lower quadrant pain. For the first time, CA was reported by Crymble and Forsythe in 1949. 3 If chronic abdominal syndrome with pain localized in the right lower quadrant lasts for longer than 3 months, diagnostic laparoscopy is administered followed by appendectomy.4,5 As a rule, after appendectomy the pain syndrome subsides.
We analyzed clinical, morphological, and immunohistochemical studies of the appendix to confirm the adequacy of surgery for CRLQP children.
Materials and Methods
We carried out comparative studies of clinical presentations and results of morphological and immunohistochemical studies of remote appendicitis in 55 cases treated over the period from 2008 to 2020. Mean age at operation was 10.8 years (range, 7–16 years). This study was approved by the local ethical committee at the university. Parents of the patients included in the study provided their informed consent for an analysis of clinical information including images such as ultrasound protocols and X-rays. Permission was given to publish these materials anonymously, without disclosing the patient's identity.
The mean number of preoperative clinical visits or emergency admissions for recurrent pain was 5 (range, 2–8). There were 33 boys and 22 girls. The criterion for inclusion was recurring abdominal pain lasting >6 months. Criteria for exclusion from the study group: concomitant gastrointestinal disease, irritable bowel syndrome, and no catamnestic follow-up after surgery. The intensity of pain syndrome was assessed using Pain Faces Scale.6,7 Clinical presentations were assessed using international prognostic scores (Pediatric Appendicitis Score and Alvarado score). 8
Clinical investigations included a full blood count, serum urea, and C-reactive protein. All patients had abdominal ultrasound, fiberoptic duodenogastroscopy, and irrigography. An indication for laparoscopic appendectomy was the presence of right lower quadrant pain persisting for >6 months, without signs of peritoneal irritation. All procedures were performed by laparoscopic technique. The follow-up took place at 6–12 months after surgery. The surgery outcome was considered satisfactory if pain syndrome had subsided altogether, and unsatisfactory if it recurred.
Immunohistochemistry studies were made using UltraVision (LabVision, UK) detection systems, standard sets of primary polyclonal antibodies to vascular endothelial growth factor (VEGF), matrix metalloproteinase 9 (MMP-9), CD106 (LabVision), vasoactive intestinal peptide (VIP), and collagen IIIα1 (GeneTex, USA). The nature of immunohistochemistry reaction was appraised visually by points, taking into consideration the intensity of staining or the number of positively stained cells using standard morphometry. 9
Statistical analysis
The data were analyzed using the SPSS version 17 statistical package for the social sciences (SPSS Inc., Chicago, IL). The significance of differences between the groups was assessed using nonparametric tests. The clinical informative value of diagnostic tests, sensitivity, and specificity was assessed using receiver operating characteristic (ROC) analysis.
Results
In patients with CRLQP, the intensity of pain syndrome was 5.4 points (95% confidence interval [CI] 4.5–6.2; degree of freedom [df] 10.1) and the Alvarado score was 3.5 points (95% CI 3.1–4.0; df 16). ROC analysis showed a low prognostic value of the Alvarado score and Pediatric Appendicitis Score (area under the curve [ACU] 0.09; 95% CI 0.01–1.0; P < .0001) in determining the indications for surgery
ROC analysis permitted determination of signs specific for CA: nonmigrating pain (AUC 0.71; 95% CI 0.63–0.79; P < .0001), no tension of anterior abdominal wall (AUC 0.83; 95% CI 0.77–0.9; P < .0001), no hyperthermia (AUC 0.68; 95% CI 0.6–0.77; P < .0001), no leukocytosis (AUC 0.78; 95% CI 0.71–0.86; P < .0001), and no neutrophil shift in leukocyte formula (AUC 0.75; 95% CI 0.68–08; P < .0001).
Ultrasound signs of CA were the following: obstructed appendiceal lumen due to sclerosing, thinning out walls, hyperechoic structure of mucosa and submucosa with heterogeneous echotexture, and appendix diameter not more than 6 mm (Fig. 1).
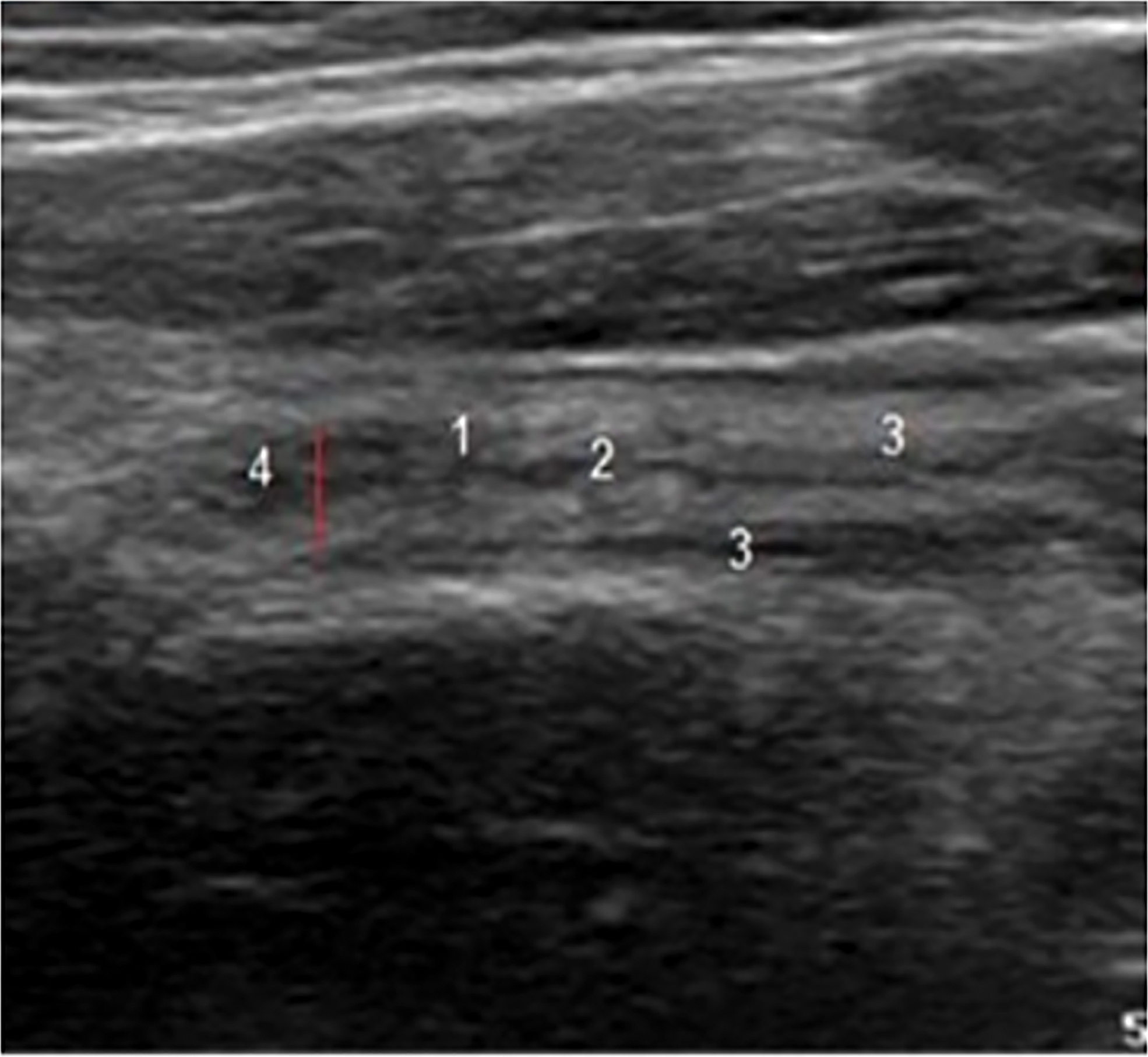
Longitudinal sonogram of patient B with chronic abdominal syndrome and right lower quadrant pain: 1—uneven obstructed lumen of appendix vermiformis; 2—hyperechoic submucosa; 3—muscular layer of uneven thickness; 4—appendix vermiformis diameter 5 mm. Color images are available online.
ROC analysis demonstrated low specificity and accuracy of ultra sound in determining the signs specific for CA; it did not exceed 35%.
The management method of choice in CRLQP is surgical exploration, most typically laparoscopic, followed by an appendectomy. A follow-up at 6 months after surgery detected no recurrence of pain syndrome in 100% of patients with CA.
Inmmunohistochemistry studies revealed three types of appendiceal changes in children with CRLQP.
Type 1
Type 1 (n = 21) chronic inflammation of the appendix with atrophy of the mucous membrane and fibrosis of appendix wall. Inflammatory white blood cells (WBC) infiltration is localized within the appendiceal mucosa. Abnormal immunohistochemistry findings manifest as greater expression of vascular cell adhesion molecule (CD106/VCAM-1) and a greater number of MMP-9 positive cells (Fig. 2).
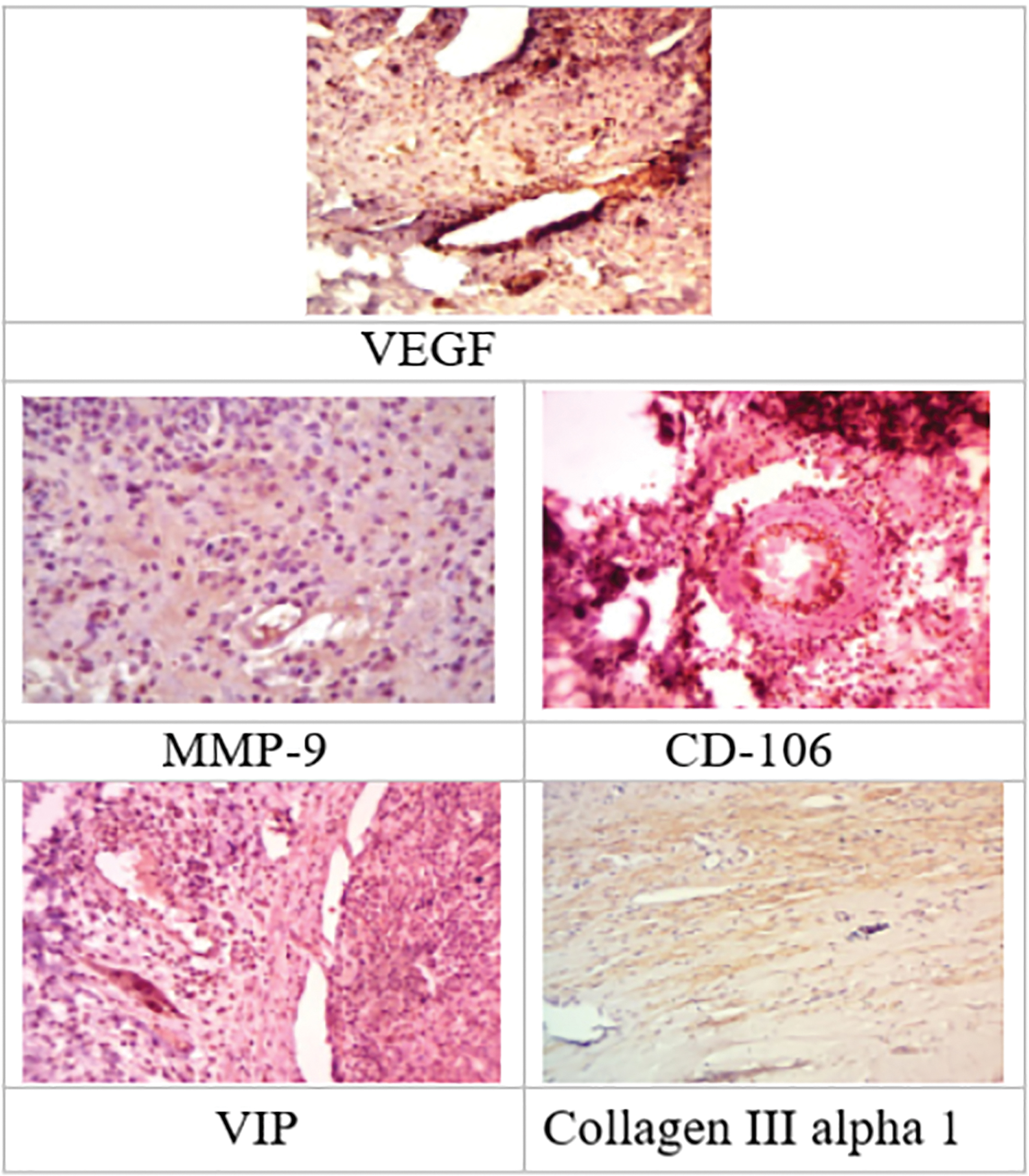
Histology of abnormal appendices in CA with signs meeting the criteria of chronic inflammation. Immunohistochemistry reaction with primary antibodies, DAB visualization counterstained with hematoxylin. Primary magnification × 100, × 200. CA, chronic appendicitis; DAB, 3,3′-Diaminobenzidine; MMP-9, matrix metalloproteinase 9; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide. Color images are available online.
Type 2
Type 2 (n = 20) lymphoid hyperplasia of the appendix (LHA) with infiltration of the mucosa and submucosa, desquamation of surface epithelium, hyperplasia of lymphoid follicles, edema of connective tissue stroma, and fragmentation of elastic and reticular fibers, dilation and blockage of blood vessels, thickening of the vascular walls. The cortical layer of mesenteric lymph nodes shows a lower lymphocyte count with emerging centers of lymphoid cell proliferation and accumulation, which corresponds to chronic inflammation. Abnormalities detected by immunohistochemistry were greater expression and higher number of MMP-9 positive cells and of CD106/VCAM-1, greater expression of collagen IIIα1, lower expression and lesser count of positive cells expressing VEGF and VIP (Fig. 3).
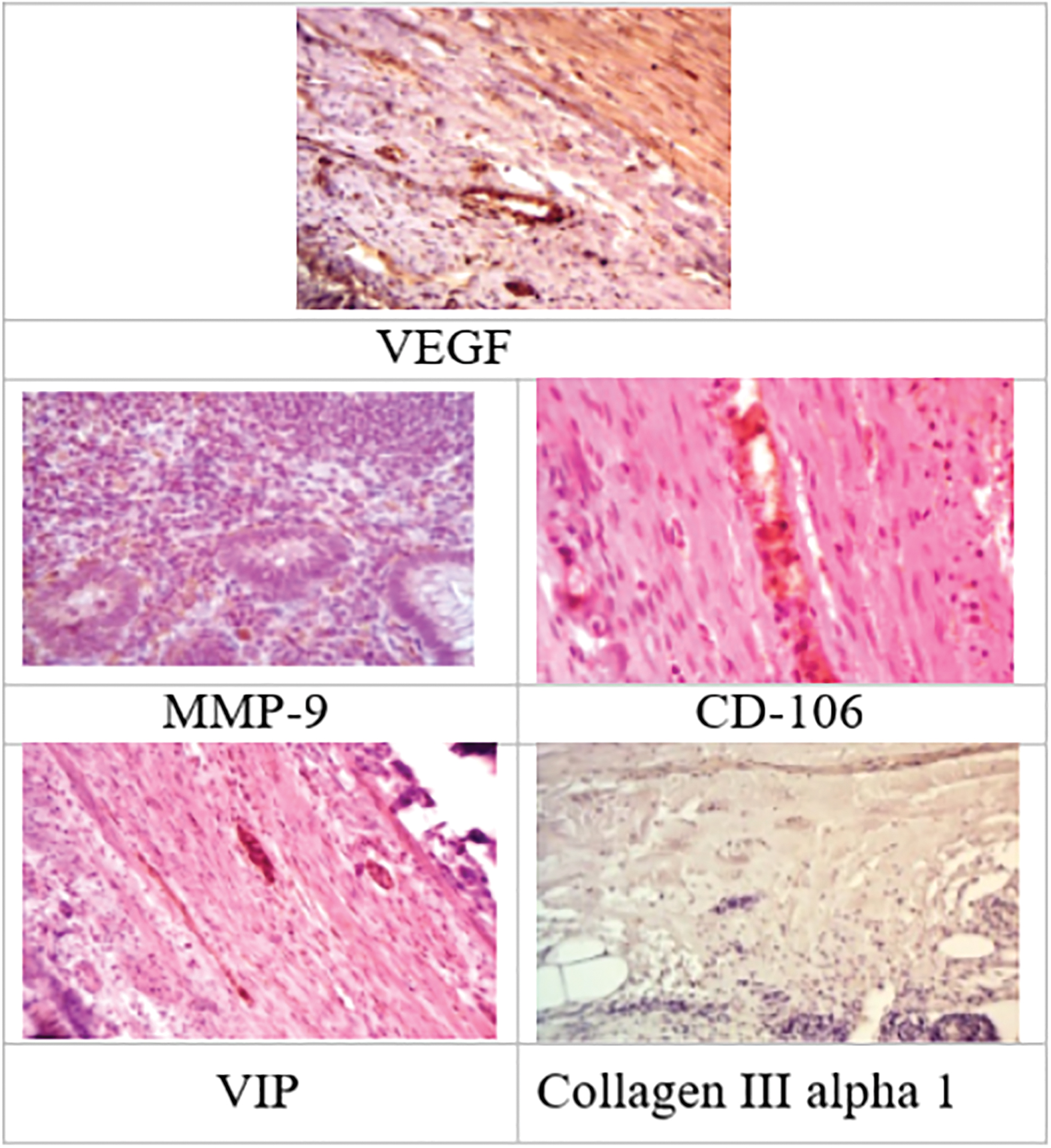
Histology of abnormal appendices with lymphoid hyperplasia. Immunohistochemistry reaction with primary antibodies, DAB visualization counterstained with hematoxylin. Primary magnification × 100, × 200. DAB, 3,3′-Diaminobenzidine; MMP-9, matrix metalloproteinase 9; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide. Color images are available online.
Type 3
Type 3 (n = 12) catarrhal inflammation, manifested by impaired blood circulation in the mucous membrane without destruction and inflammation in the appendix. Immunology abnormalities were greater expression and lower number of MMP-9 positive cells and of CD106/VCAM-1, VIP, collagen IIIα1 (Fig. 4).
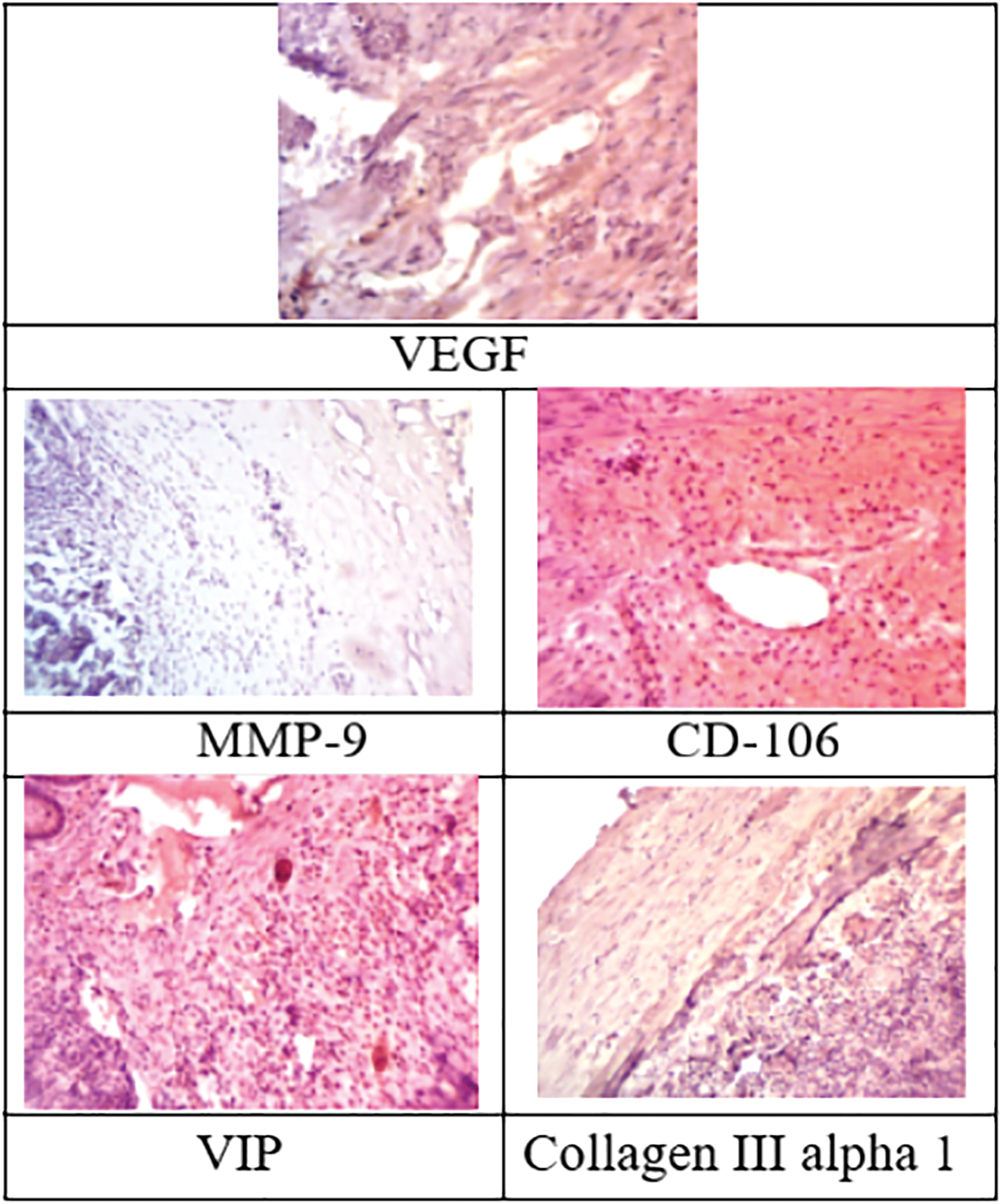
Histology findings of catarrhal appendix vermiformis. Immunohistochemistry reaction with primary antibodies, DAB visualization counterstained with hematoxylin. Primary magnification × 100, × 200. DAB, 3,3′-Diaminobenzidine; MMP-9, matrix metalloproteinase 9; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide. Color images are available online.
Discussion
Management of recurrent abdominal pain requires a prolonged hospital stay, work-up, and conservative treatment, which does not always prove effective. The diagnosis of CA can be made in patients with right lower quadrant pain who show no peritoneal signs or any abnormality in laboratory tests. Up to date, there is no clear-cut approach to CA management.
Among indications for surgery, the prevailing factor is the presentations: persisting pain syndrome, absence of any concomitant disease, and ineffectiveness of conservative approach.10,11 An analysis undertaken by the authors steers us toward this point of view. No specific clinical signs were found that would help determine indications for appendectomy in CRLQP patients. Right now CA appears to be a diagnosis by exclusion without any clear clinical signs. Considering the low prognostic value of international appendicitis scores for CA diagnosis, the scope of investigations and indications for surgery must be subject to unequivocal regulation.
Diagnostic laparoscopy is administered to patients with CA as a conclusive stage of work-up, secondary to all available noninvasive investigations. The objective of laparoscopy is to establish the possible cause of right lower quadrant pain rather than to explore the appendix itself. Reliable macroscopic signs typical of CA were as follows: appendix atrophy, and fecaloma in its lumen, diverticula, and mucocele. 12 Certain conditions of appendix vermiformis such as neurogenic appendicopathy are not visible macroscopically and can only be established by histology studies. 13 Thus, we believe that appendectomy is advisable even if laparoscopy did not reveal the apparent cause of abdominal syndrome. Complete subsidence of pain syndrome established by follow-up can be considered clinical proof of appendectomy effectiveness in CA patients. In our series of observations, complete recovery was noted in 100% of patients. Appendectomy in CA is not a wonder cure; however, due to elimination of the probable cause of recurrent pain syndrome, it produces complete clinical recovery.
Immunohistochemistry tests allowed receiving new data on the nature of inflammatory changes in the appendix vermiformis in patients with CRLQP. Detection of higher expression of CD106 (VCAM-1) and MMP-9 in appendices excised in patients with type 1 changes confirms the presence of chronic inflammation. MMP-9 is a zinc-dependent peptidase capable of cleaving proteins of extracellular matrix, mostly collagen types 1 and 4, regulating transcription of cytokines and growth factors that supposedly participate in tissue destruction. 14 MMP-9 can be activated by inflammation markers interleukin-6 and tumor necrosis factor as well as activated neutrophils. Recent research by A. Solberg showed that higher expression of MMP-9 was noted in perforated appendicitis. 15 Considerably higher expression of MMP-9 in CA patients detected by us results from a recurrent inflammation causing formation of fibrosis in the appendix. CD106 (VCAM-1) is a molecule of cellular adhesion, a transmembrane protein, member of immunoglobulin superfamily. This protein is expressed in the vascular epithelium in certain inflammations and is a way of adhesion and migration to endothelial cells for lymphocytes and monocytes, but not for neutrophils; it provides for endothelial proliferation during angiogenesis. 16 The high expression of VIP in CA patients correlates with findings by Di Sebastiano et al., who demonstrated more intensive VIP expression in a group of morphologically normal appendices in patients with AA signs. 17 The higher VIP expression we detected explains the ineffectiveness of conservative treatment for CA patients with persisting pain syndrome, which can be an argument in favor of surgery. Collagen IIIα1 is known to be synthetized at early stages of wound healing, but as the scar is formed, its synthesis declines with a gradual increase in collagen type 1 synthesis. In our study the greater cell count and higher expression of collagen IIIα1 can be considered a manifestation of sclerosis mechanism in conditions of chronic inflammation.
Detection of changes type 2 typical of LHA indicates difficulty with differential diagnosis of recurring abdominal pain. Lymphoid hyperplasia is the most common histology finding in pediatric patients operated for AA. According to data from cohort studies, the rate of LHA detection can be as high as 20%, which is considered to be extremely high. 18 However, immunohistochemistry of appendices with LHA revealed changes typical for an active course of chronic inflammation. Since no ultrasound signs of LHA in the form of inflammation of surrounding fatty tissue and mucosal hyperplasia were found, laparoscopic appendectomy in our study can be regarded an adequate approach to management. Besides, ineffective conservative management and persisting abdominal pain makes laparoscopic appendectomy an adequate approach to management of recurring pain syndrome in right lower quadrant.
The VEGF protein is a glycoprotein stimulating formation of new lymphatic and blood vessels. It is known to be a part of a system responsible for restoring oxygen transport to tissues in situations when blood circulation is insufficient or it is necessary to provide collateral circulation. 19 Higher expression of VEGF-positive cells may indicate a response to local hypoxia in CA patients and confirms neovascularization in conditions of a chronic pathological process. Changes detected in the form of vascular congestion indicate the presence of hypoxia as the prevailing factor of CA.
Thus, the revealed types of histological and immunohistological changes in appendices of CRLQP patients can be considered a recurring inflammation ultimately resulting in involution of the organ in the form of fibrosis. It appears that the established inflammatory changes in the appendix vermiformis in patients with CRLQP can be considered an argument in favor of surgery.
All found immunological and morphological changes in the appendix can be regarded as signs of CA.
Conclusion
Laparoscopic removal of appendix vermiformis after a comprehensive work-up can relieve abdominal pain in patients with CRLQP.
This study demonstrates that most patients with CRLQP have far-reaching changes in the structure of appendix vermiformis, meeting the criteria of chronic inflammation (which we regarded as signs of CA).
Footnotes
Acknowledgment
We thank Janna S. Martinson for the precious advice and suggestions during the revision of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.