
Abstract
Congenital esophageal stenosis (CES) is a very rare clinical condition found in 1 per 25,000 to 50,000 live births. There are three histological types of CES described: tracheobronchial remnants, fibromuscular stenosis (FMS), and membranous stenosis. The first-line treatment in most cases is the conservative treatment (dilatation with a Savary bougie or balloon), but in some CES types, dilatation may be ineffective or result in esophageal perforation with serious complications or lethal outcome. Resection of the stenotic segment and end-to-end esophageal anastomosis was formerly presented as the most common surgical treatment option for CES. However, esophagoplasty is a safe and feasible alternative for surgical treatment of esophageal stenosis in children. Our aim is to report two cases of FMS submitted to thoracoscopic esophagoplasty. Both cases started with dysphagia and refusal after transition to solid diet, at 6 months old, and the radiological examination showed stricture of the distal esophagus. Esophagoplasty was performed with the patients in prone position. The stenotic esophageal wall was incised longitudinally and transverse synthesis was performed. After surgery, the patients had prompt recovery, without recurrent stenosis, remaining asymptomatic, with good diet acceptance.
Introduction
Congenital esophageal stenosis (CES) is manifested as an intrinsic circumferential narrowing of the esophagus lumen present at birth, although not necessarily symptomatic in the neonatal period.1,2
It is an extremely rare clinical condition found in 1 per 25,000 to 50,000 live births. 2 The incidence of other associated congenital anomalies ranges from 17% to 33%, and is frequently associated with esophageal atresia. Other described malformations are cardiac anomalies, diaphragmatic hernia, intestinal atresia, anorectal malformations, and chromosomal anomalies (trisomy 21).2,3
The most widely used classification of CES is based on histological types and consists of three categories: tracheobronchial remnants (TBR), fibromuscular stenosis (FMS), and membranous stenosis (MS). Symptoms usually begin at the age of 4–10 months with introduction of semisolid or solid fooding, depending on the location and the degree of the stenosis. Most common symptoms are progressive dysphagia and vomiting. 4
It can be investigated by contrast study, endoscopy, ultrasound, and computed tomography (CT). The definitive diagnosis and classification are possible by histopathology. 2
Dilatation and surgery are the possible treatments for CES. The choice of the procedure depends on the pathohistological type, location, and severity of the stenosis. 2 Resection of the stenotic segment and end-to-end esophageal anastomosis was formerly presented as the most common surgical treatment option for CES. However, recently, thoracoscopic repair of esophageal pathologies 5 in prone position 6 has become frequent and a more conservative, safe, and feasible alternative for surgical treatment in children, as shown in our reports. We report two cases of CES, in which the infants underwent thoracoscopic esophagoplasty successfully.
Case Reports
Case 1
Three-year-old boy with a history of vomit, dysphagia, and refusal of solid foods starting at 6 months old. The patient had previous diagnosis of bilateral radial hypoplasia and aqueductal stenosis. Radiological investigation with contrast was performed, which demonstrated a stricture at the distal third of the esophageal lumen (Fig. 1), and endoscopy suggested FMS type of CES. The patient was referred for surgical approach and was placed in prone position for a thoracoscopic approach. Esophagoplasty was performed. Upper GI endoscopy was associated to identify the stenotic esophageal segment and then the stenotic esophageal wall was incised longitudinally 2 cm above and 2 cm below the stenosis and transverse synthesis, interrupted suture with 4/0 prolene, was performed. Intraoperative biopsy was collected and pathology confirmed FMS of the esophagus. He presented an esophageal leak on the second postoperative day, which was clinically treated by Penrose drain and spontaneously closed. The patient evolved satisfactorily and was discharged on the 22nd postoperative day with appropriate dietary intake.

In case 1, preoperative radiological investigation with contrast showed an abrupt narrowing in the lower esophagus. No evidence of a tracheoesophageal fistula or gastroesophageal reflux.
Case 2
Ten-month-old boy with history of choking and dysphagia after transition to solid diet, at 6 months old. CES was suspected and radiological investigation was performed, showing stenosis of the distal esophagus. Patient was referred for surgical approach. On the operating room, endoscopy was performed to identify the stenotic area by thoracoscopy. Esophagoplasty was performed with the patient in prone position. The esophageal wall was incised longitudinally 2 cm above and 2 cm below at the stenotic area, and transverse synthesis with separated total suture stitches, with 4/0 prolene, was performed. Intraoperative biopsy was collected and histopathological examination diagnosed esophageal fibrosis (FMS). Patient had an uneventful post-op, until the sixth postoperative day, when he swallowed a piece of a plastic spoon while feeding, which got stuck in the suture, and caused fistula with further mediastinal collection. CT-guided drainage was performed and the fistula resolved spontaneously. Six years after surgery, the patient remains asymptomatic with good diet acceptance.
Operative procedure
We perform a thoracoscopic mobilization of the esophagus in prone position with right prone posterior approach. The patients were intubated in a nonselective way. Then, they were turned to prone position, leaving the abdomen free to allow respiratory movements. The right arm is abducted above 100°. On the right side of the patient, stand the surgeon and the camera surgeon. On the left side, stand the second assistant and the scrub nurse. The monitor is positioned at the left shoulder of the patient (Fig. 2). CO2 pneumothorax is created by closed Veress technique in fifth intercostal space (ICS), maintaining insufflation pressure of 6–8 mmHg. Three 5-mm ports are used. A 30° scope is used for the entirety of the procedure. The ports sites are: (A) in the fifth ICS under the scapula's angle, for camera; (B) fourth ICS 7 cm from the spinous process for right-hand working; and (C) seventh ICS 7 cm on the same vertical line as (B) for the left-hand working (Fig. 3). A flexible upper gastrointestinal endoscope can be placed into the esophagus to lift it, to make the repair easier. Esophageal wall was incised longitudinally in the stenotic area, and transverse synthesis with separated full thickness suture stitches were performed. A nasogastric tube was left in the esophageal lumen for 7 days and fed the patients on post-op day 1. Oral food was started after 7 days post-op with an esophagram. A video demonstrating this technique is available online (Supplementary Video SV1).
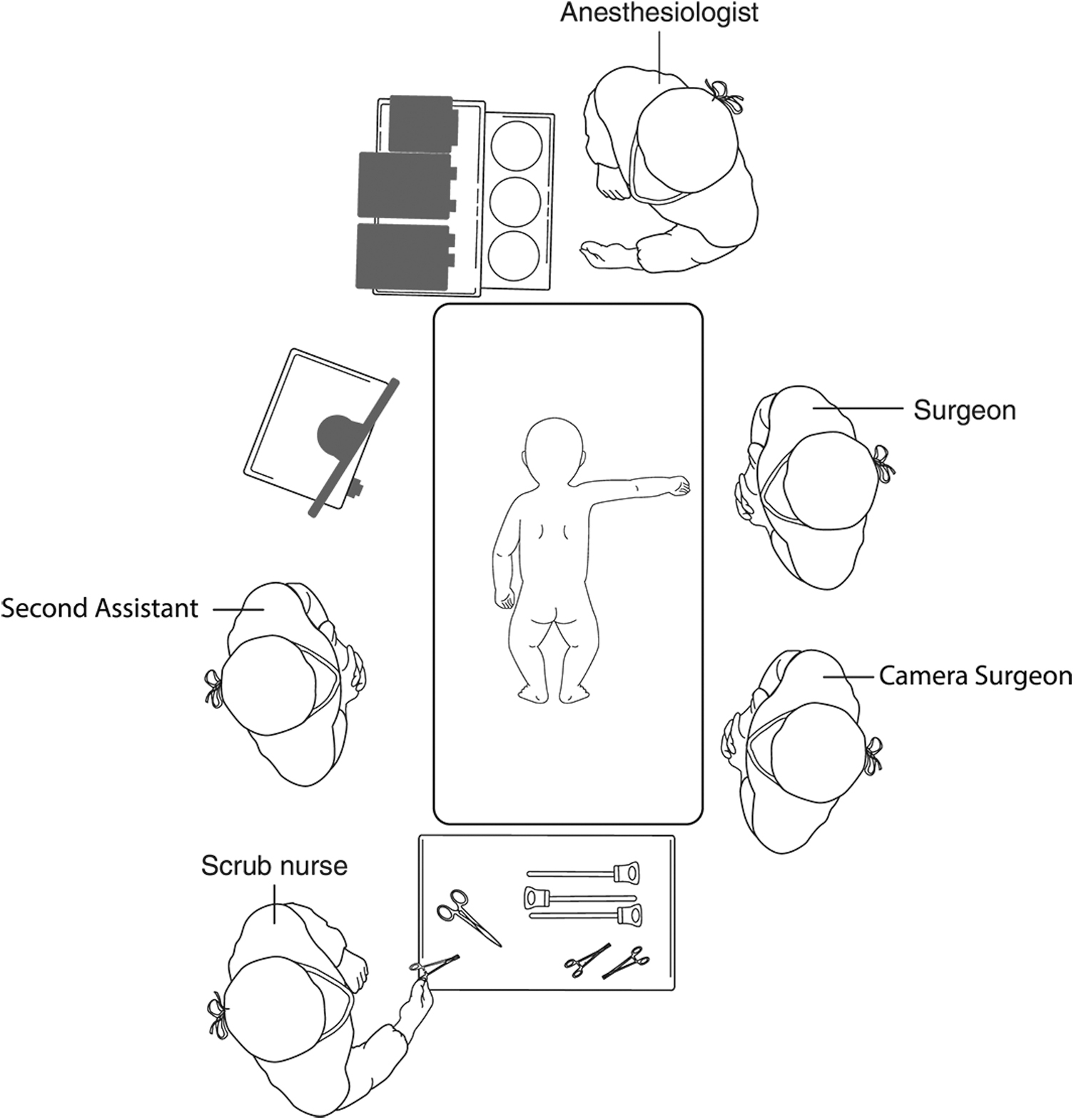
Position of the patient, surgeons, anesthesiologist, scrub nurse, and video monitor.
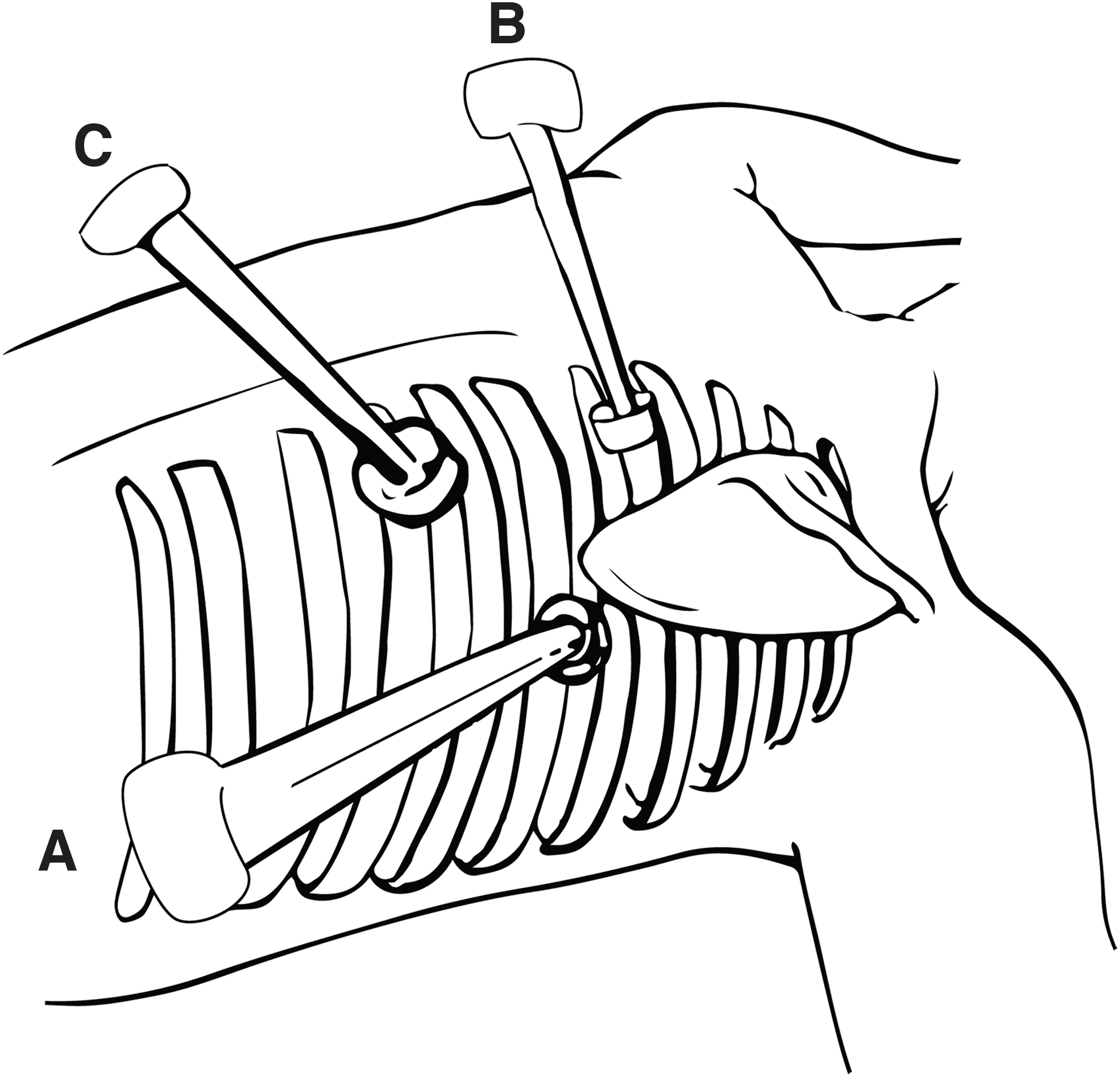
Sites of the three ports:
Discussion
Initial symptoms of CES usually are progressive dysphagia and vomiting, but can include failure to thrive and food impaction, and in cases of severe stenosis, hypersalivation, respiratory distress, stridor during feeding, developmental deficits, regurgitation of liquids, aspiration pneumonia, and even lethal pneumonia, can be noted. Owing to the variety of symptoms and low prevalence, the CES diagnosis can be delayed and the mean age of diagnosis is 12 months old.2,4,7 Dilatation and surgery are possible treatments for CES. The procedure of choice depends on the pathohistological type, location, and severity of the stenosis. The first-line treatment in most cases is the conservative treatment (dilatation with a Savary bougie or balloon), 1 but in some CES types, for example TBR, 6 dilatation may be ineffective or result in esophageal perforation with serious complications or lethal outcome.
In FMS and MS types, Suzuhigashi et al. demonstrated, in a study with 40 CES patients, that, in general, balloon dilatation is an effective treatment, but the risk of complications with balloon was higher than expected: 26.9% of the FMS treated with balloon dilatation resulted in perforation, 22.2% needed a radical operation after dilatation, and 25.9% remained symptomatic. 4 Furthermore, other complications of dilatation methods were reported, such as recurrent stenosis, bleeding, sepsis, mediastinitis, aspiration pneumonia, and cardiac arrest. Therefore, balloon dilatation must be carefully indicated and performed in FMS.2,4
The surgical treatment of choice in most cases of TBR CES is still the resection of the stenotic segment and end-to-end esophageal anastomosis, by thoracotomy or by thoracoscopy, as recently reported. 5 In the FMS type, this surgery is performed mostly after previous ineffective dilatation.
Esophagoplasty of the stenotic area with longitudinal incision and transverse synthesis is not commonly reported as a surgical option for the treatment of CES. However, in our two cases it was a safe and feasible alternative for CES in children. Although we reported esophageal fistulas in both cases, in case #2 we strongly believe that the leak developed because of the swallowing of the foreign body, and in case #1 the leak was directed by the Penrose drain resulting in spontaneous closure.
The thoracoscopy approach with the patient in prone position provides an excellent exposure for esophagoplasty, as reported in literature for adult patients. 8 The advantages of thoracoscopic approach of the esophagus in prone position are, above all, reduction of anesthesia time; decreased lung injury and preventing its retraction, because the lung collapses better due to a positive pressure pneumothorax associated with gravity in prone position; decreased bronchial and tracheal injuries, and excellent exposure of the operative field. In our two cases, the infants underwent thoracoscopic esophagoplasty with prompt recovery, without recurrent stenosis and with satisfactory follow-ups.
Ethical Approval
The Ethics in Research Committee of the Federal University of Paraná approved this study. The research was carried out considering the measures of protection, minimization of risks, confidentiality, and responsibility of the researcher and the institution. It is developed in accordance with national and international protocols, in addition to the basic principles of protection of the rights and dignity of human beings, as described in the Declaration of Helsinki (64th Fortaleza, Brazil, in October 2013) and in accordance with applicable local laws.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.