
Abstract
Introduction:
The aim of this report is to present our technique and outcomes of single incision laparoscopic percutaneous extraperitoneal closure of internal ring (SILPEC) for incarcerated inguinal hernia (IIH) in children.
Patients and Methods:
The medical records of all children undergoing emergency SILPEC for IIH after unsuccessful attempted manual reduction between June 2016 and September 2020 at our center were reviewed. For SILPEC, two trocars 3.5–6 mm were placed through a single umbilical incision. A 17G epidural needle and a small wire–lasso were used for extraperitoneal closure of the internal ring.
Results:
From a total of 2904 consecutive patients with inguinal hernia (IH) undergoing SILPEC, 104 patients (3.6%) had IIH. There were 84 boys and 20 girls with a median age of 18.5 months (ranged 1 month to 11 years). At the time of surgery under general anesthesia IIH was found to be spontaneously reduced in 26.9%; the hernia contents were bowel in 52.9%, great omentum in 13.5%, and ovary in 6.7% of the patients. All hernias were successfully reduced without additional ports or conversion to open surgery. Patent contralateral processus vaginalis (PCPV) was detected intraoperatively in 44.2% of the cases. The median operative time was 24 minutes for unilateral and 30 minutes for bilateral procedures. The median postoperative stay was 1 day. At a median follow-up of 28 months, there was no case of hydrocele, testicular atrophy, or iatrogenic cryptorchism. The postoperative cosmesis was excellent as all patients were virtually scarless. Recurrence occurred in 1.9% with no significant difference (P = .669) compared to the 1.4% recurrence rate of the 2800 patients with ordinary IH undergoing elective SILPEC during the same study period.
Conclusions:
SILPEC for IIH in children is feasible, safe, with excellent postoperative cosmesis, and no significant difference in hernia recurrence between emergency SILPEC for IIH and elective SILPEC for ordinary IH.
Introduction
Incarcerated inguinal hernia (IIH) is a common surgical emergency in children. Compared to the ordinary inguinal hernia (IH), the surgical repair for IIH presents a challenge for the pediatric surgeon since it often occurs in small infants and is associated with higher risk of complications and recurrence.1,2 The conventional laparoscopic approach for pediatric IIH has been reported to be safe and efficacious.2–13 However, there are few studies with limited number of patients examining the feasibility and efficacy of single incision laparoscopic percutaneous extraperitoneal closure of internal ring (SILPEC) for pediatric IIH.14–16 We report our single center experience of SILPEC in a large series of pediatric patients with IIH.
Materials and Methods
This study was approved by the Institutional Review Board of Saint Paul Hospital, Hanoi Vietnam. The data of all children undergoing SILPEC for indirect IH from June 2016 to September 2020 at our center were prospectively collected. We conducted a retrospective chart review of all patients with IIH who have undergone emergent SILPEC after unsuccessful attempts at manual reduction. The preoperative diagnosis of IIH was made by history–taking, clinical examination, and ultrasound.
According to our protocol, manual reduction without sedation or anesthesia is first attempted on all patients with IIH. If the manual reduction is successful without complications, the surgical repair is scheduled as an elective procedure after several days. All patients with irreducible IIH would otherwise undergo emergent SILPEC. In this report, these cases of irreducible IIH are referred to as “incarcerated inguinal hernia.”
SILPEC procedure description: The patient is placed in supine position on the table with the surgeon standing on the right, the assistant on the left, and the monitor at the left end of the table.
Under general anesthesia, no attempt of manual reduction is done on the table without laparoscopy. Through a 10-mm vertical umbilical incision, a 6-mm trocar for the camera is inserted superiorly with CO2 insufflation at 8–10 mm Hg and a second 3.5-mm trocar placed in the lower part of the incision for a 3 mm grasper (Fig. 1).
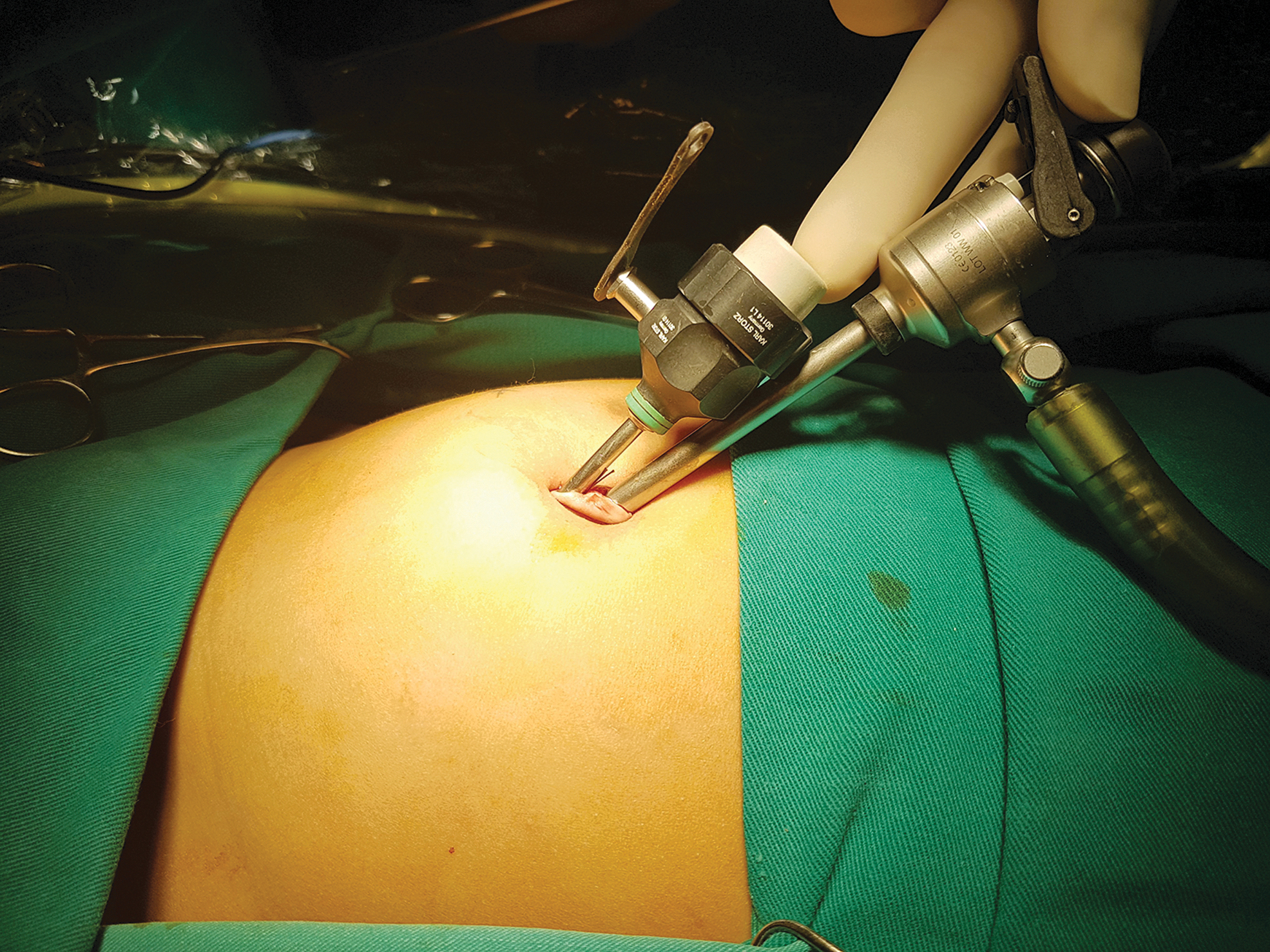
Placement of two trocars through a single 10-mm umbilical incision. Color images are available online.
Under laparoscopic control, the herniated content was reduced by a combination of external manual pressure and internal pulling with a bowel grasper. The reduced organ was checked for any lesion and viability. If resection or repair is needed, the organ is delivered outside the abdomen through a small extended umbilical incision.
A 1.5 mm stab wound is made on the abdominal wall superiorly to the internal inguinal ring at its 1 o'clock position. A 17G epidural needle is inserted perpendicular to the abdominal wall through the stab wound and directed under the peritoneum anterior to the testicular vessels and the vas, from the internal ring at 1 o'clock toward 8 o'clock where it enters the peritoneal cavity. The 3 mm grasper is used to manipulate the peritoneum at the internal ring to assist with this maneuver. A wire lasso is inserted through the needle lumen into the abdominal cavity, and the grasper at the 3.5 mm port was used to thread a 2.0 suture into the lasso. The needle is pulled out of the abdomen together with the lasso and one end of the suture.
The epidural needle is inserted again through the same stab wound and threaded under the peritoneum from 1 o'clock toward 8 o'clock in the other direction and goes into the peritoneal cavity through the same previous needle exit site. The lasso is inserted again through the needle lumen, catching the other end of the suture inside the peritoneal cavity with the assistance of the grasper, and then the needle with the lasso and the other suture end is pulled out. At this time, the suture lays extraperitoneally 360° around the internal ring with both its ends outside the abdomen. The scrotum and inguinal canal are squeezed to evacuate the residual gas and/or fluid before the suture is tied.
The contralateral internal ring is explored with the assistance of the 3 mm grasper. If the contralateral processus vaginalis is found to be patent, it is closed using the same technique. The umbilical incision is closed with 6.0 polyglactin suture, and the inguinal stab wound was taped without any suture.
The patients resume oral feeding after 3–6 hours and are discharged on the next day if the recovery is uneventful, with outpatient clinic visits at 1 month and 3 months and at 6-month interval by telephone or clinic visits as needed.
We collected data of patient age, gender, body weight, presence of uni- or bilateral hernia, clinical presentations, intraoperative findings, operative time, hospital stay, complications, and hernia recurrence. Comparison between groups was done using the Student's T-test, Mann–Whitney test, chi-square test, or Fisher exact test as appropriate. A P value <.05 is considered to be statistically significant.
Results
From a total of 2904 consecutive patients with IH undergoing SILPEC during our study period, 387 patients (13.3%) were admitted to the emergency department for incarceration. IIH was reduced successfully in 281 (73.1%) of the patients. They were all scheduled for late elective surgery. The remaining 104 patients (26.9% of IIHs or 3.6% of all IHs) underwent emergency SILPEC, with 84 boys (80.8%) and 20 girls (19.2%) at an age range of 1 month to 11 years. The prevalence of irreducible IIH was 3.4% for boys and 4% for girls with IH (P = .580, Table 1).
Clinical Characteristics of Patients with Ordinary Versus Incarcerated Inguinal Hernia
The significance of italic values is P < 0.05.
Number calculated in boys only.
The median age for ordinary hernia versus IIH is 37 months versus 18 months (P = .04, Table 1). Infants under 12 months of age have a significantly higher risk of incarceration (odds ratio = 2.138; 95% confidence interval: 1.408–3.295; P < .0001).
IIH was noted on the right in 63.5% of the patients with a right:left ratio of 1.7:1, with no difference compared to ordinary hernia. Incarceration on the right and the left side IH was seen in 4.2% and 3.1% of the patients, respectively (P = .131). No incarceration was seen in the 90 patients with bilateral IH (compared to the 13.3% with unilateral hernia, P = .076).
At the time of laparoscopy, IIH was found to be spontaneously reduced in 28 patients (26.9%). The herniated contents were bowel in 55/104 patients (52.9%) with small bowel in 41 patients (39.4%), cecum in 13 patients (12.5%: cecum with appendix—2.9%, cecum with appendix and terminal ileum—9.6%), sigmoid colon in 1 patient (0.9%), great omentum in 14 patients (13.5%), and ovary in 7 patients (6.7%, Table 2).
Clinical Characteristics of Boys Versus Girls with Incarcerated Inguinal Hernia
The significance of italic values is P < 0.05.
IIH, incarcerated inguinal hernia.
All herniated contents were reduced successfully without conversion to open surgery or the use of additional ports. In one infant with incarcerated terminal ileum - cecum–appendix, a cecal perforation was found and brought out for repair by a small extension of the umbilical incision. Oophorectomy was performed in a patient with nonviable ovary. Patent contralateral processus vaginalis was detected intraoperatively in 44.2% of the cases. The median operative time was 24 minutes for unilateral versus 30 minutes for bilateral procedure.
There was no intraoperative complication. Postoperative transient scrotal edema/hydrocele was noted in 16.7% of the male patients. There was no wound infection. The median postoperative stay was 1 day. At a median follow-up of 28 months (range 7–57 months), no hydrocele, testicular atrophy, or iatrogenic cryptorchism was found. Recurrence occurred in 2 patients (1.9%), and both successfully underwent redo SILPEC (Table 1). The postoperative cosmesis was excellent as all patients had no visible surgical scar (Fig. 2).

Postoperative cosmesis 3 months after SILPEC. SILPEC, single incision laparoscopic percutaneous extraperitoneal closure of internal ring. Color images are available online.
Compared to the ordinary IH, the median operative time for IIH was significantly longer (23 and 30 minutes for uni- and bilateral procedure versus 19 and 25 minutes, respectively, P = .000); the incidence of postoperative transient hydrocele was significantly higher (16.7% versus 0.17%, P = .000). The median postoperative hospital stay was 1 day for both ordinary and incarcerated IH. There was no significant difference in the recurrence rate between elective SILPEC for ordinary IH and emergent SILPEC for IIH (1.9% versus 1.4%, P = .669, Table 1).
Comparing the clinical characteristics of boys and girls with IIH, there were no significant differences in terms of age, body weight, laterality of IH, clinical presentations, postoperative hospital stay, and recurrence. However, the most common herniated organ was the bowel in boys versus the ovary in girls (P = .000); the operative time in girls was significantly shorter than in boys (20 minutes versus 24 minutes, P = .000) (Table 2).
Discussion
The reported incidence of incarceration in children with IH ranges from 3% to 17%,1,2 and the incidence of unsuccessful manual reduction of IIH ranges from 0.5% to 3.4% of all IHs.7–9,12,16 In our series, the incidence of 13.3% for incarceration and 3.6% for irreducible IIH of all IHs was within the range of the reported data. In our series, IIH was found more often in boys and on the right side, similarly to what we found for the ordinary IH. While some authors reported a higher incidence of IIH in girls 16 or the left side IIH in girls, 7 our study did not show that incarceration was related to gender or laterality. Consistent with other reports,1,2,16 IIH in our series was found to be significantly more common in the younger age group, particularly at <12 months.
Compared to the ordinary IH repair, the emergent open repair for IIH is reported to be associated with a higher rate of intra- and postoperative complications such as injury to vas and testicular vessel, wound infection, testicular atrophy, as well as a higher recurrence rate.1,2
Laparoscopic repair for ordinary IH has gained a wide popularity among pediatric surgeons worldwide. Compared to open herniotomy, systematic reviews showed that laparoscopic hernia repair is equally efficacious in terms of recurrence17–20 but with the advantages of decreased postoperative complications,19,20 better wound appearance, 18 and the ability to explore and repair the contralateral side to prevent metachronous hernia. 17 However, there are few comparative studies between laparoscopic and open approach for IIH, and their results demonstrated that laparoscopic herniorrhaphy for IIH is equally efficacious 8 or associated with fewer complications than open repair. 9
To avoid the higher complications of an open repair in IIH, the conventional approach for IIH is manual reduction and delay of the surgical repair for 1 or 2 days, with emergent surgery for unsuccessful manual reduction.1,2 In our opinion, this approach can be valuable for laparoscopic repair as well. Our results showed that nearly three fourth of IIH could be manually reduced without sedation or anesthesia and can be similarly managed with elective repair one or several days later to reduce the risks of surgery and general anesthesia in an emergency setting. Some authors have recommended immediate 10 or a shorter delay 11 in laparoscopic herniorrhaphy for IIH after successful manual reduction. However, more extensive studies are needed to prove the safety and cost-effectiveness of these approaches in larger cohort of patients.
In our series, >25% of the IIH was found to be spontaneously reduced at the time of laparoscopy. Myorelaxation during general anesthesia can facilitate IIH spontaneous reduction. For the irreducible IIH during emergent repair, some authors attempted manual reduction while the patient is under general anesthesia before surgery.7,12 For an open repair, the risk of unrecognized lesions of the reduced organ, especially gangrenous bowel, has been reported. 1 We do not recommend blind manual reduction while the patient is under general anesthesia if a laparoscopic repair is anticipated, since an inspection of the herniated content could be done, the manual reduction can be further facilitated with the use of the laparoscopic grasper, and widening of the internal ring with insufflation of the peritoneal cavity might assist in the reduction. These benefits of the laparoscopic approach over the open repair for IIH have been reported.2–7
Other advantages of the laparoscopic approach for IIH include easier closure of the internal ring from within the peritoneal cavity to avoid the edematous and distorted anatomy of the inguinal canal2–9,12; better vision with camera magnification to reduce the risks of vas and vessel injury; and the ability to diagnose and repair a patent contralateral processus vaginalis to prevent metachronous IH.8,9,12
Conventional laparoscopic surgery (CLS) using two to three ports at separate skin incisions is the most common approach for laparoscopic repair of pediatric IH, including IIH.2–12,17–20 A wide variety of techniques have been described for intra- or extraperitoneal closure of the internal ring in CLS with good outcome.21–23 Single site or single incision laparoscopic repair has more postoperative cosmesis advantage than CLS. 24 Different techniques for single site laparoscopic techniques for IIH have been described, namely the use of a transumbilical two-port technique with a round needle and intracorporeal knot 13 or with a percutaneous straight needle and extracorporeal knot 14 or a single port technique. 15
Our technique of a transumbilical modification of the original LPEC technique for IH was first reported by Takehara et al. 23 Compared to CLS, the disadvantages of our SILPEC technique may be instrument crowding and difficulties with intracorporeal suturing. Our SILPEC technique for IIH is simple and easy since all surgeons, including the junior doctors, in our department can perform the procedure with good outcome; since our operative time seems shorter than seen in most other reports on open repair or CLS with intraperitoneal closure for IIH4,7,8; since no additional port or open surgery conversion was necessary, no intraoperative complication was seen. This is in contrast to the open repair of IIH, which is still considered to be a demanding procedure that often requires more experienced surgeons.8,9 From our experience and others’, 14 a laparoscopic assisted approach of exteriorizing the damaged organ by extension of umbilical incision for further repair is highly feasible and efficacious.
Our extensive experience with nearly 3000 SILPEC repairs for IH, including IIH, showed excellent postoperative cosmesis as all the patients had no visible scar. However, evaluation of the postoperative cosmesis in this report was still based on subjective opinions of the surgeons and the patient's parents, and more objective measures are warranted in further studies.
Our study is the first one to directly compare the outcomes of SILPEC for IIH versus ordinary IH. Our results showed that emergency SILPEC for IIH has comparable results as elective SILPEC for ordinary IH for most outcome measures, namely postoperative hospital length of stay, complications, and recurrence except for the expected IIH transient scrotal edema/hydrocele in boys.
In conclusion, our SILPEC technique for IIH in children is feasible, safe, with excellent postoperative cosmesis, and no significant difference in the recurrence rate between emergency SILPEC for irreducible IIH and elective SILPEC for ordinary IH.
Footnotes
Acknowledgment
The authors thank Prof. Ai Xuan Holterman for her help in editing of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study and preparation of this paper.