
Abstract
Background and Aim:
Endoscopic injection sclerotherapy is effective for the treatment of gastric variceal bleeding, but may cause fatal ectopic embolism. Spontaneous portosystemic shunts are one of the risk factors for ectopic embolism. This present study aims to evaluate the efficacy and safety of clip-assisted endoscopic cyanoacrylate injection for the treatment of acute gastroesophageal variceal bleeding.
Methods:
The medical records of patients with gastroesophageal varices (GOVs) who underwent clip-assisted cyanoacrylate injection at the Ningbo First Hospital from March 2017 to August 2020 were reviewed. The outcomes were immediate hemostasis rate, early rebleeding rate, late rebleeding rate, and procedure-related complications. The gastrorenal and splenorenal shunts were evaluated by the computed tomography angiography.
Results:
A total of 9 patients with GOVs (GOV1 and GOV2) were analyzed, and 4 of the patients had spontaneous portosystemic shunts. The average number of clips used in each patient was 2.11 ± 1.96, and an average of 5.11 ± 1.76 mL of cyanoacrylate was injected into each patient. All patients completed immediate hemostasis. Two patients experienced rebleeding, including 1 case of early rebleeding and 1 case of late rebleeding (both due to cyanoacrylate extrusion) during a median follow-up of 367 days (interquartile range 270–855 days). Five patients underwent follow-up endoscopy; eradicated gastric varices (GVs) were revealed in 1 patient, and shrunken GVs were found in 4 patients. No serious complications, including ectopic embolism, were observed.
Conclusion:
The present study showed the efficacy and safety of clip-assisted endoscopic cyanoacrylate injection in acute GOV bleeding, but these results require verification by randomized controlled studies with larger sample numbers.
Introduction
Gastroesophageal variceal bleeding is one of the serious complications of decompensated cirrhosis, accounting for 30%–40% of cirrhosis-related mortality. 1 Gastric varices (GVs) have a lower incidence than esophageal varices (EVs), but they have a higher bleeding rate and mortality, resulting in a poorer prognosis. 2 According to the classification system proposed by Sarin et al., 2 GVs are classified into gastroesophageal varices (GOVs) and isolated gastric varices (IGVs). GOV1 is associated with EVs and continues to the lesser curve of the stomach, while GOV2 continues to the greater curvature of the stomach. GOV2 has a relatively higher recurrence and rebleeding rate than GOV1. 3
According to the Baveno VI Consensus Workshop, endoscopic cyanoacrylate injection is recommended for hemostasis of acute bleeding from GVs. 4 However, cyanoacrylate injection may cause fatal embolism of important organs, including the lungs, brain, and kidneys,5–7 especially in patients with gastrorenal shunts (GRSs) and splenorenal shunts (SRSs). Many techniques have been proposed to prevent ectopic embolism, including balloon-occluded retrograde transvenous obliteration (B-RTO), endoscopic ultrasound (EUS)-guided treatment with combined coils and cyanoacrylate, and transjugular intrahepatic portosystemic shunt (TIPS).8–12 It has also been reported that endoscopic clipping before cyanoacrylate injection may block blood flow and prevent ectopic embolism. 13
In this present study, we report 9 patients with acute GOV bleeding who underwent clip-assisted endoscopic cyanoacrylate injection. The novel procedure was demonstrated to be safe and efficient for emergency hemostasis of GVs.
Materials and Methods
Patients with acute GOV bleeding (active bleeding from GOV1 or GOV2 varices) were hospitalized and underwent clip-assisted endoscopic cyanoacrylate injection in the Department of Gastroenterology, Ningbo First Hospital, from March 2017 to August 2020. The data were retrospectively collected.
The inclusion criteria were as follows: (1) liver cirrhosis confirmed by history, imaging, or biopsy; (2) presented with melena or hematemesis on admission or during hospitalization, and active bleeding from GOVs confirmed by endoscopy; and (3) age ≥18 years. The exclusion criteria were as follows: (1) severe diseases, including cardiac, brain, lung, or renal insufficiency; (2) regional portal hypertension; (3) comorbid hepatocellular carcinoma not meeting the Milan criteria or other malignancies; and (4) a history of previous endoscopic variceal sclerotherapy, tissue adhesive injection, esophageal variceal band ligation, TIPS, liver surgery, or transplantation.
Finally, 9 patients were included in our study. Written informed consent was obtained from these patients before the procedure. The study was approved by the Ethics Committee of Ningbo First Hospital (IRB approval No. 2021RS017) and conformed to the guidelines of the Declaration of Helsinki.
Before endoscopic treatment, the liver function reserve was evaluated by the Child-Pugh (CP) score, and appropriate medications, such as terlipressin and somatostatin, were administered. Endoscopic treatment was performed under general anesthesia. First, GVs were classified according to morphology as follows: tortuous (F1), nodular (F2), and tumorous (F3). 14 Clip-assisted endoscopic cyanoacrylate injection was then performed to obturate the F2- or F3-type varices.
First, a metal clip was placed on the narrow part of the varices to clamp all the varices and surrounding tissue as fully as possible. The procedure was repeated if necessary, until the inflow vein bulged and the outflow vein collapsed. After the blood flow was blocked, a “modified sandwich method” (lauromacrogol, cyanoacrylate, and normal saline) was used to obliterate the GVs. First, the inflow of vein was punctured with a needle, and lauromacrogol was injected (Tianyu Pharmaceutical Co. Ltd., Shanxi, China) followed by N-butyl-2-cyanoacrylate (Histoacryl, B. Braun, Melsungen, Germany) and lauromacrogol. Then, the needle was quickly withdrawn, and the injection point was slightly pressed to prevent leakage. Similar procedures were performed to block the outflow until the entire vein was stiff. In addition, endoscopic lauromacrogol injection or band ligation was performed in patients with moderate to severe EVs.
After 48–72 hours of fasting, a liquid diet was given for 2 or 3 days. Third-generation cephalosporins, terlipressin, and somatostatin were routinely administered for 3–5 days following the procedure. Patients with severe anemia (Hb <60 g/L) or massive blood loss were given blood transfusion.
The follow-up data were collected from medical records, telephone follow-ups and outpatient follow-ups. Initial hemostasis, rebleeding, and postoperative complications were evaluated. The initial hemostasis referred to the successful control of bleeding within 48 hours after treatment. Rebleeding was defined as the occurrence of hematemesis or melena requiring hospitalization. Early rebleeding was defined as bleeding occurring within 30 days of initial hemostasis, while late rebleeding was defined as bleeding occurring after 30 days. 15 Postoperative complications included fever, systemic infection, local infection, chest pain, abdomen pain, dysphagia, or ectopic embolism. Since there was little time for computed tomography angiography (CTA) before emergency hemostasis, all patients underwent CTA postoperatively to evaluate the GRS and SRS.
Statistical analysis was performed with IBM SPSS STATISTICS (V.22.0). Data for continuous variables are presented as the mean ± standard deviation or median (interquartile range [IQR]) where appropriate.
Results
The clinical characteristics of the 9 patients are shown in Table 1. All patients were male, with an average age of 56.78 ± 13.37 years. According to the etiology, 5 patients (55.6%) had hepatitis B cirrhosis, and 4 patients (44.4%) had alcoholic cirrhosis. One patient had comorbid hepatocellular carcinoma meeting the Milan criteria (11.1%). According to the CP score, 4 patients (44.4%) were CP class A, 3 patients (33.3%) were class B, and 2 patients (22.2%) were class C. One patient (11.1%) presented with melena, while the other 8 patients (88.9%) presented with both hematemesis and melena. Five patients (55.6%) received blood transfusion. Three patients (33.3%) had a history of variceal bleeding, and 2 patients (22.2%) had portal vein thrombosis.
Clinical Characteristics and Perioperative Conditions of 9 Patients
CP, Child-Pugh; EV, esophageal varice; GOV. gastroesophageal varice; GRS, gastrorenal shunt; GV, gastric varice; HCC, hepatocellular carcinoma; SRS, splenorenal shunt.
All 9 patients were diagnosed with liver cirrhosis with GOV bleeding, and endoscopic hemostasis was performed in the acute phase of bleeding. The endoscopic characteristics and treatment are shown in Table 1.
Two patients (22.2%) had GOV1 bleeding, whereas 7 patients (77.8%) had GOV2 bleeding. Five patients (55.6%) presented with F2-type varices, whereas the other 4 patients (44.4%) had F3-type varices. The process of clip-assisted endoscopic cyanoacrylate injection in GOV bleeding is shown in Figure 1. During the treatment, the average number of clips for each patient was 2.11 ± 1.96 with the following distribution: 1 clip was used in 5 patients; 2 clips were used in 2 patients; and 3 or more clips were used in 2 patients. Each patient was injected with 5.11 ± 1.76 mL of cyanoacrylate. Four patients were treated for EVs at the same time. Among these patients, 3 patients were treated with lauromacrogol injection, and 1 patient was treated with ligation. According to postoperative CTA, 2 patients had GRS, 1 patient had SRS, and 1 patient had both GRS and SRS. Figure 2 shows the image of a GRS in a patient.
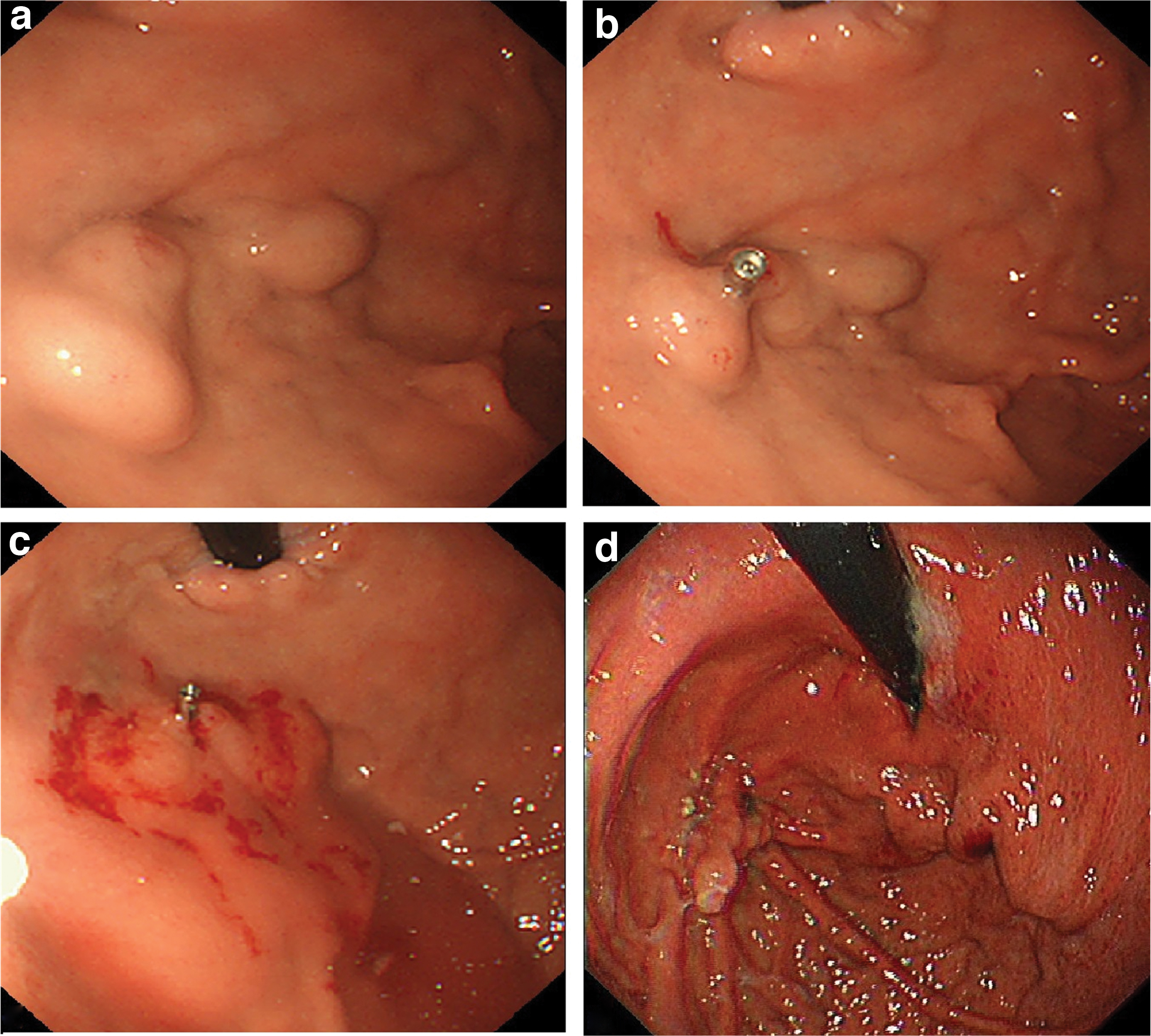
Clip-assisted endoscopic cyanoacrylate injection.
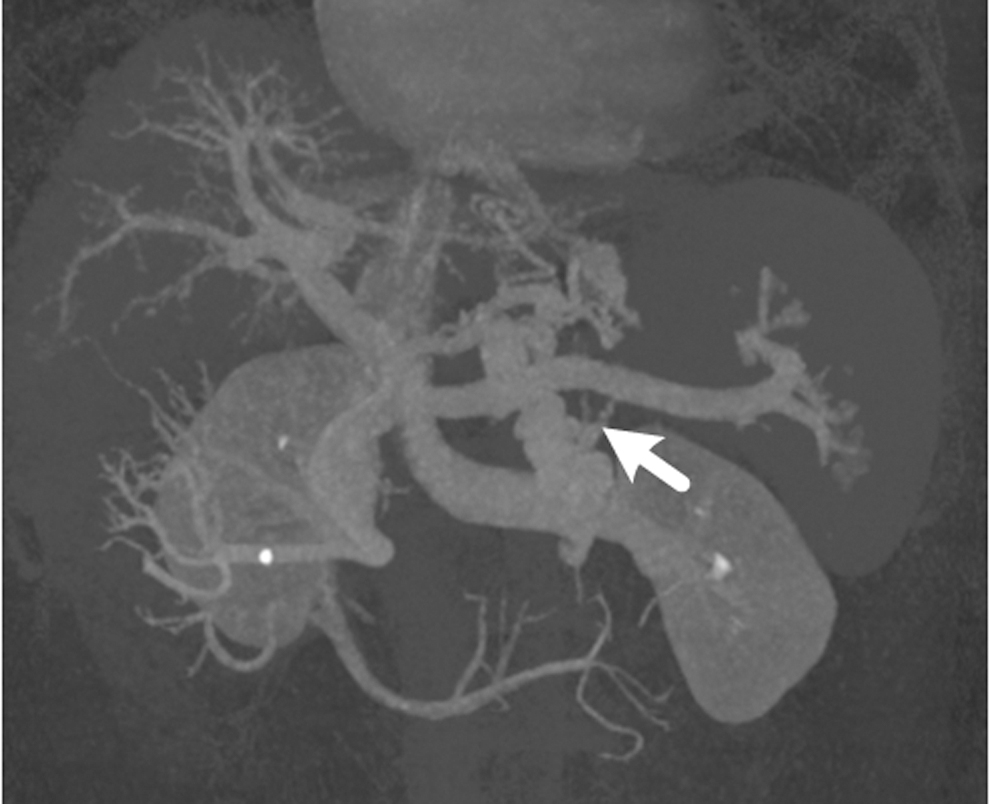
A gastrorenal shunt displayed by computed tomography angiography (The white arrow points the gastrorenal shunt).
The mean hospital stay was 15.78 ± 4.29 days, and the median follow-up time was 367 days (IQR 270–855 days). All the patients completed the initial hemostasis. Rebleeding occurred in cases 1 and 6, both of which were due to cyanoacrylate extrusion. In the first treatment of case 1, F3-type varices on the greater curvature were obliterated. On the 20th day after the procedure, melena occurred (early rebleeding), and subsequent endoscopy showed collapsed varices and extruded cyanoacrylate on the greater curvature. In the first treatment of case 6, F2-type varices of the gastric cardia nearing the fundus were obliterated. A slight melena occurred 40 days afterward (late rebleeding), and extruded cyanoacrylate in the cardia was found by endoscopy. Both patients recovered after secondary cyanoacrylate injection.
In addition, 5 patients underwent endoscopic surveillance in a median of 48 days (IQR 35–238 days) after the procedure, of whom one had eradicated varices and 4 had shrunken varices (Fig. 1; Table 1).
No serious complications occurred. No severe abdominal pain, chest tightness, shortness of breath, or spontaneous peritonitis occurred. No symptoms or signs related to ectopic embolism were observed. Three patients suffered from fever, and 1 patient suffered from hepatic encephalopathy (Table 1). These patients recovered after symptomatic treatment. No patients died during the follow-up period.
Discussion
The metal clip is a common apparatus that is frequently used for endoscopic hemostasis of nonvariceal upper gastrointestinal bleeding. In recent years, many studies have confirmed the significance of clips in acute gastroesophageal variceal bleeding.
Miyoshi et al. 16 first reported the usage of endoscopic variceal clipping (EVC) in preventing esophageal variceal bleeding in 9 cases. Yol et al. 17 proposed that EVCs effectively block the blood flow of large EVs and lower the risk of rebleeding, indicating that EVCs are not inferior to ligation. Mitsunaga et al. 18 conducted a 15-year observation to confirm the efficacy and safety of EVCs to prevent the progression of GOVs in children. Carlos et al. 19 reported successful EVCs in 6 patients with refractory cirrhosis and gastroesophageal variceal bleeding. Similarly, metal clips can also be used to clamp the varices before cyanoacrylate injection, which potentially blocks the blood flow of the large GVs and lowers the risk of rebleeding.
We reported 9 patients with acute GOV bleeding who were treated by clip-assisted endoscopic cyanoacrylate injection. The initial hemostasis rate was 100%, which was higher than that of 87%–100% in previous studies.15,20–23 Two patients (22.2%) experienced rebleeding, which was similar to the 17.1%–41% reported in previous studies.15,20–23 These 2 patients had GOV2 varices, suggesting a poor prognosis of this type, which was similar to the observations of a previous study. 3 Since same endoscopic procedures were performed by an expert endoscopist, and initial hemostasis was fully confirmed, the rebleeding was not attributed to technical errors. The reason for poor prognosis of GOV2 varices requires further study. Five patients completed the follow-up endoscopy in a median of 48 days (IQR 35–238 days), and the varices were eradicated in 1 patient and shrunken in 4 patients. The data indicated a favorable hemostatic effect of this technique.
Patients with GVs had GRS or SRS (60%–85%) more commonly than those with simple EVs (17%–21%). 24 According to the Sarin classification, 2 patients with GOV2 and IGV1 varices had GRS or SRS more frequently than other types. The percentage of spontaneous portosystemic shunts in our study (4 patients, 44%) was slightly lower than previous data, which may have resulted from the relatively small sample size. Spontaneous portosystemic shunts increase the risk of ectopic embolism after cyanoacrylate injection.5–7
Many techniques have been proposed to prevent ectopic embolism. B-RTO was invented to block the GRS before the embolism of GVs, and had high hemostasis rate. However, it required the preoperative CTA, and might lead to the aggravation of EVs and ascites.8,9 TIPS establishes a shunt with a stent between the portal vein and the hepatic vein. The early application of TIPS effectively achieves hemostasis and reduces mortality, 10 and it has been recommended as the gold-standard treatment by American association for the study of liver diseases. 8 However, it is difficult to apply TIPS to patients with severe decompensated cirrhosis because it increases the risk of hepatic encephalopathy. 11 EUS-guided treatment with combined coils and cyanoacrylate might lower the risk of ectopic embolism, using the coil as a stent to retain the glue in the varices. 12 This procedure has a high rate of hemostasis and few complications in GOV bleeding. 12
Unlike these techniques, clip-assisted cyanoacrylate injection requires no complicated instruments or procedures, which is more convenient for emergency hemostasis and more applicable in primary hospitals. The clip can separate large varices into multiple small varices, thus blocking the blood flow and preventing ectopic embolism. Li et al. 13 reported a case of GV with GRS, in which successful hemostasis was achieved using endoscopic clipping before cyanoacrylate injection. Two multicenter retrospective studies have evaluated shunts with preoperative CTA and indicated that clip-assisted cyanoacrylate injection might reduce the risk of ectopic embolism.25,26 However, research data are still lacking, and none of the present studies focus on acute GOV bleeding or emergency hemostasis without preoperative CTA.
In this study, we focused on emergency hemostasis of acute GOV bleeding without preoperative CTA. No symptoms or signs related to ectopic embolism were observed, suggesting the safety of the clip-assisted cyanoacrylate injection to a certain extent. As ectopic embolism is a rare complication, we explain here that the procedure could reduce the risk of embolism in the following two ways. First, the inflow of the vein bulged due to blood perfusion (felt hard when touched with the needle sheath), while the outflow collapsed (felt soft when touched with the needle sheath) after the clip was deployed. This indicated that the blood flow was blocked by the clip, which eventually lowered the risk of embolism. Second, postoperative CTA revealed the obturation of GVs and the confinement of glue to the varices, indicating an optimal effect of endoscopic obturation and embolism prevention.
Therefore, clip-assisted treatment may help reduce the risk of ectopic embolism for patients with GRS or SRS. Our study suggests that during emergency hemostasis with little time for CTA, the type and severity of GVs can help to evaluate possible shunts and the risk of ectopic embolism, in which case clip-assisted treatment can be applied if necessary.
Clip-assisted cyanoacrylate injection had several advantages. First, the initial hemostasis rate was high, and the rebleeding rate was relatively low. Second, no symptoms related to ectopic embolism were observed. For patients with spontaneous portosystemic shunts, the risk of ectopic embolism might be reduced. Third, compared with other techniques such as B-RTO and EUS-guided therapy, this procedure only required the participation of endoscopists, which is more convenient and applicable for primary hospitals.
Our study had several limitations. First, we used medical records instead of direct history collection from patients, which may have led to recall bias. Second, the sample size was small and the data came from a single center. Because some patients did not undergo endoscopic follow-up, we were unable to conduct a controlled study or further evaluate the long-term effectiveness and safety of the procedure. In future research, multicenter randomized controlled studies are required to confirm the clinical value of clip-assisted endoscopic cyanoacrylate injection in acute GOV bleeding.
Conclusion
We reported 9 patients with acute GOV bleeding who underwent clip-assisted endoscopic cyanoacrylate injection without preoperative CTA. The effective initial hemostasis, low rebleeding rate, and lack of symptoms related to ectopic embolism suggested the efficacy and safety of the procedure. This technique is a promising treatment for acute GOV bleeding, but its efficacy and safety require further verification by randomized controlled studies with larger sample numbers before wide application.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Zhejiang Medical Health Science and Technology Program (No. 2021KY992) and Ningbo Natural Science Foundation of China (No. 2019A610221).