
Abstract
Background:
Endoscopic tattooing of colorectal tumors enables tumor localization and determination of appropriate surgical margins. It becomes very difficult to detect the distal surgical margins (DSMs) of rectal tumors in patients who obtain clinical complete response (cCR) after neoadjuvant therapy. In this study, our aim is to examine the benefits of endoscopic tattooing of the tumor before neoadjuvant therapy in patients with locally advanced rectal cancer in accurate localization of the previous tumor and in providing appropriate DSMs in cases with cCR.
Patients and Methods:
The patients who were diagnosed with locally advanced rectal cancer, received neoadjuvant therapy and subsequently achieved cCR, and underwent surgery between January 2015 and October 2020 were included in the study. The patients were divided into two groups according to whether they were endoscopically tattooed before neoadjuvant chemoradiotherapy.
Results:
A total of 49 cases were included in the study. Significantly better DSMs were observed especially in female gender in the tattooed group. DSMs were found to be closer to the resection margins in the nontattooed group. It was found that endoscopic tattooing had a significant effect on the DSM in the regression analysis (P = .06, R2 = 0.47). It was determined that laparoscopy or open surgery alone did not differ in terms of DSMs but open surgery together with tattooing was found to be strongly effective in providing larger DSMs.
Conclusion:
In locally advanced rectal cancer, endoscopic tattooing of the distal margin of the tumor before neoadjuvant therapy is a reliable and effective method for obtaining a safe DSM and not leaving the residual tumor at the lower end of anastomosis, especially in cases of cCR.
Introduction
Neoadjuvant chemoradiotherapy (CRT) followed by total mesorectal excision (TME) has become the standard treatment for locally advanced rectal cancer.1–3 Clinical complete response (cCR) occurs in nearly half of patients after neoadjuvant therapy. cCR is defined as an absence of residual mass, ulceration, or stenosis within the rectum by endoscopic examination. Pathological complete response (pCR) is the absence of any viable tumor cells in surgical specimens. Approximately half of the patients with cCR have residual tumor cells upon microscopic examination. 4 Considering that accurate detection of pCR in patients with cCR is only possible with histopathological examination of the resection specimen, it appears that the surgery of these patients is especially important in terms of distal surgical margin (DSM).
It is very difficult to determine DSM of rectal tumors in patients who obtain cCR after neoadjuvant therapy. If there is no mark that identifies the previous tumor location, when cCR is encountered, either the total rectum is removed or there is a risk of leaving residual disease with a rectum transection above the tumor location. If an adequate and safe DSM is not obtained, local recurrences due to tumor regrowth may occur in a short time, and on the contrary, if the tumor is resected with wide margins, serious postoperative morbidity may be encountered.
Especially with the development of laparoscopic surgical techniques, endoscopic tattooing of colon tumors has become more widely used. However, endoscopic tattooing of rectal tumors varies according to the surgeon's preference, since the operation to be performed is standard TME and the location of the tumor can be determined by methods such as digital rectal examination (DRE) and proctoscopy.5,6 In this study, the contribution of tattooing distal margin of the tumor before neoadjuvant therapy in patients with locally advanced rectal cancer to localize the previous tumor location accurately and to provide appropriate DSM in cases with cCR was investigated.
Materials and Methods
The data of the patients who were diagnosed with locally advanced rectal cancer, received neoadjuvant therapy, and subsequently achieved cCR and underwent surgery between January 2015 and October 2020 were retrospectively analyzed. The study was approved by the ethics committee of Health Sciences University, Sisli Etfal Training and Research Hospital (approval number: 2568; approval date: 15/10/2019). The patients who were operated without neoadjuvant therapy due to synchronous colonic tumor or early stage tumor, those who underwent abdominal perineal resection (APR), and those with cCR after neoadjuvant therapy were excluded from the study.
We classified the individuals into two groups according to whether they were endoscopically tattooed before neoadjuvant CRT. Group 1 was the tattooed group and group 2 was the nontattooed group. Age, gender, body mass index (BMI), tumor location in the rectum, time interval, surgical technique, operative time, rates of frozen section, distal and radial surgical margins, tumor regression scores, and number of lymph nodes (LNs) removed were analyzed and compared between the groups.
Using a 25 gauge sclerotherapy needle, 0.5–0.75 mL of India ink (SPOT®; GI Supply, Camp Hill, PA) was injected into the submucosal layer. The India ink was injected at three to four circumferential sites and 2–3 cm distal to the tumor. Indian ink is a permanent opaque black pigment. For accurate staging of neoadjuvant CRT applied rectal carcinoma, it is important to keep in mind that when microscopic remnants of tumor are not found, area of the prior tumor localization must be entirely sampled by the pathologists.
All surgical procedures were performed by the surgeons experienced in the surgery of colorectal cancer. Low anterior resection (LAR) or very-low anterior resection (VLAR) was performed in all cases in accordance with the principles of TME, which is the standard technique for rectal tumor surgery. Operations were performed through either the open or the laparoscopic approach. The cases that had been converted from laparoscopic to open technique were included in open technique.
Macroscopic description of the surgical specimen and the tumor; stage of cancer; local tumor depth of invasion (T); the presence and number of nodal metastases (N); the presence of distant metastases (M); and the status of the proximal, distal, and radial surgical margins were documented in the pathology report. The modified Ryan scheme for tumor regression score recommended by the College of American Pathologists, which evaluates the extent of rectal wall involvement regardless of LNs status, was used for grading tumor response to neoadjuvant therapy. The patients with ypT0 stage, indicating pCR in the rectal wall (regression score 0), were not included in the surgical margin analysis of the groups.
Statistical analysis
Statistical analyses were performed with SPSS version 25 (Statistical Package for the Social Sciences, Chicago, IL). The conformity of continuous variables to normal distribution was evaluated with the Kolmogorov Smirnov test. The Student's t-test was used to compare continuous variables with normal distribution, and Mann–Whitney U test was used to compare not normally distributed continuous variables between two independent groups. Chi-square test was used to compare categorical variables. Binary logistic regression model was used to assess and identify the cause and effect relationship between variables. The differences were considered to be statistically significant with P < .05.
Results
Elective surgery according to TME principles was performed in 198 patients who received neoadjuvant therapy with the diagnosis of locally advanced rectal cancer, and cCR was achieved in 61 (30.8%) patients. Thirty-two (16.1%) patients achieved pCR. Among the patients with cCR, 12 patients underwent APR and were excluded from the study. The study was carried out in the remaining 49 patients. Of the patients, 26 (53%) achieved pCR. Operative and histopathological findings of the patients analyzed with their demographic and clinical characteristics according to the groups are given in Table 1.
Demographic, Clinical, and Operative Characteristics, Histopathological Data of the Groups
BMI, body mass index; LN, lymph node; ypT, pathological tumor stage after neoadjuvant chemotherapy.
There was no statistically significant difference between the groups in terms of both demographic and preoperative clinical characteristics. The effects of demographic and clinical variables on intraoperative and histopathological variables were analyzed. There was no significant correlation between age, gender, time interval, and intraoperative variables. However, there was a significant correlation between BMI and operative time, and between tumor location and surgical technique (Table 2).
P values of Correlations Between Demographic Clinical Variables and Intraoperative Variables
Values shown in bold signify p < 0.05.
BMI, body mass index.
In regression analysis, BMI showed a significant effect on the operative time in both groups (group1: R2 = 0.73, P = .001 and group 2: R2 = 0.71, P = .001). When all cases were examined according to BMI, the mean operative time was found to be 197.18 ± 8.2 minutes in cases with a BMI of <30 kg/m2, whereas it was found to be 289.41 ± 18.13 minutes in cases with a BMI of ≥30 kg/m2. High BMI was associated with prolonged operative time (P = .001).
No significant correlation was found between the operative technique and the operative time in both groups (group 1: P = .16 and group 2: P = .96). The mean operative time for the laparoscopic technique was 257.81 ± 79.09 minutes, for the open technique it was 205.83 ± 37.20 minutes in group 1 (P = .17). The mean operative time for the laparoscopic technique was 218.33 ± 69.82 minutes, for the open technique it was 216.94 ± 73.36 minutes in group 2 (P = .73).
A significant and moderate correlation was found between tumor location and surgical technique in both groups (group 1: r = 0.48, P = .03 and group 2: r = 0.42, P = .02). The mean distance between the tumor and the anal verge was 5.6 ± 0.52 cm in the laparoscopy group and 7.5 ± 0.66 cm in the open group (P = .03) (Table 3).
Comparison of the Mean Distance of the Tumor According to the Surgical Technique Between the Groups
Values shown in bold signify p < 0.05.
When the effects of demographic and clinical variables on histopathological characteristics of non-pCR cases were analyzed, a significant correlation was found between gender and radial and DSMs in group 1 (radial margin: P = .01, r = 0.72 and distal margin: P = .03, r = 0.63). There was no significant correlation between gender and radial and DSMs in group 2 (radial margin: P = .11 and distal margin: P = .09) (Table 4). The mean radial surgical margin distance was 1.97 ± 0.23 cm in female gender and 0.92 ± 0.21 cm in male gender in group 1 (P = .01). The mean DSM distance was 3.07 ± 1.17 cm in female gender and 1.65 ± 0.78 cm in male gender in group 1 (P = .01).
The P values of the Correlations Between Demographic and Clinical Variables and Histopathological Variables
Values shown in bold signify p < 0.05.
BMI, body mass index; LNs, lymph nodes; ypT, pathological tumor stage after neoadjuvant chemotherapy.
Comparing the surgery techniques of the two groups, it was found that the laparoscopic technique was used more in group 1 and the open technique was used more in group 2 (P = .02). The rates of conversion and frozen section examination were evaluated between the groups and no significant difference was found. One case in group 1 and 2 cases in group 2 underwent additional resection due to DSM positivity (P = .49) (Table 5). In the case in group 1, the rectal remnant partially re-resected and anastomosis was performed in the distal rectum. In 2 cases in group 2, VLAR and anastomosis were performed by applying re-resection to the remnant rectal stump. The distance between the tumor and the anal verge before neoadjuvant therapy in the case in group 1 was 10 cm, and those in 2 cases in group 2 were 8 and 6 cm. Consequently, the DSM distance of the case in group 1 was reported as 2.4 cm, and those in the cases in group 2 were reported as 4.3 and 2.5 cm, respectively.
Comparison of Intraoperative Findings
Normal distribution.
Values shown in bold signify p < 0.05.
L/O, laparoscopic/open.
There was no significant correlation between surgical technique and conversion rates and histopathological variables. However, a negative correlation was found between the operative time and the radial surgical margin distance in both groups (group 1: r = 0.51, P = .03 and group 2: r = 0.49, P = .02) (Table 6). The mean operative time was found to be 240 ± 39.49 minutes in patients with a radial surgical margin distance of <1 cm, and 191.76 ± 47.33 minutes in patients with a radial surgical margin distance of ≥1 cm (P = .03). Positive correlation was found between pathological tumor stage after neoadjuvant chemotherapy and the operative time at the limit of significance in group 1, but it was not considered statistically significant (P = .05).
The P values of the Correlations Between Intraoperative Variables and Histopathological Results
Values shown in bold signify p < 0.05.
LNs, lymph nodes; ypT, pathological tumor stage after neoadjuvant chemotherapy.
Tumor regression scores and pathological T stages, radial surgical margins, and total and metastatic LN rates were found to be similar in non-pCR cases in both groups. Non-pCR cases were compared in terms of DSM (Figs. 1 and 2). The mean DSM distance was 2.17 ± 1.13 cm in group 1 and 1.20 ± 1.24 cm in group 2 (P = .02) (Table 7).
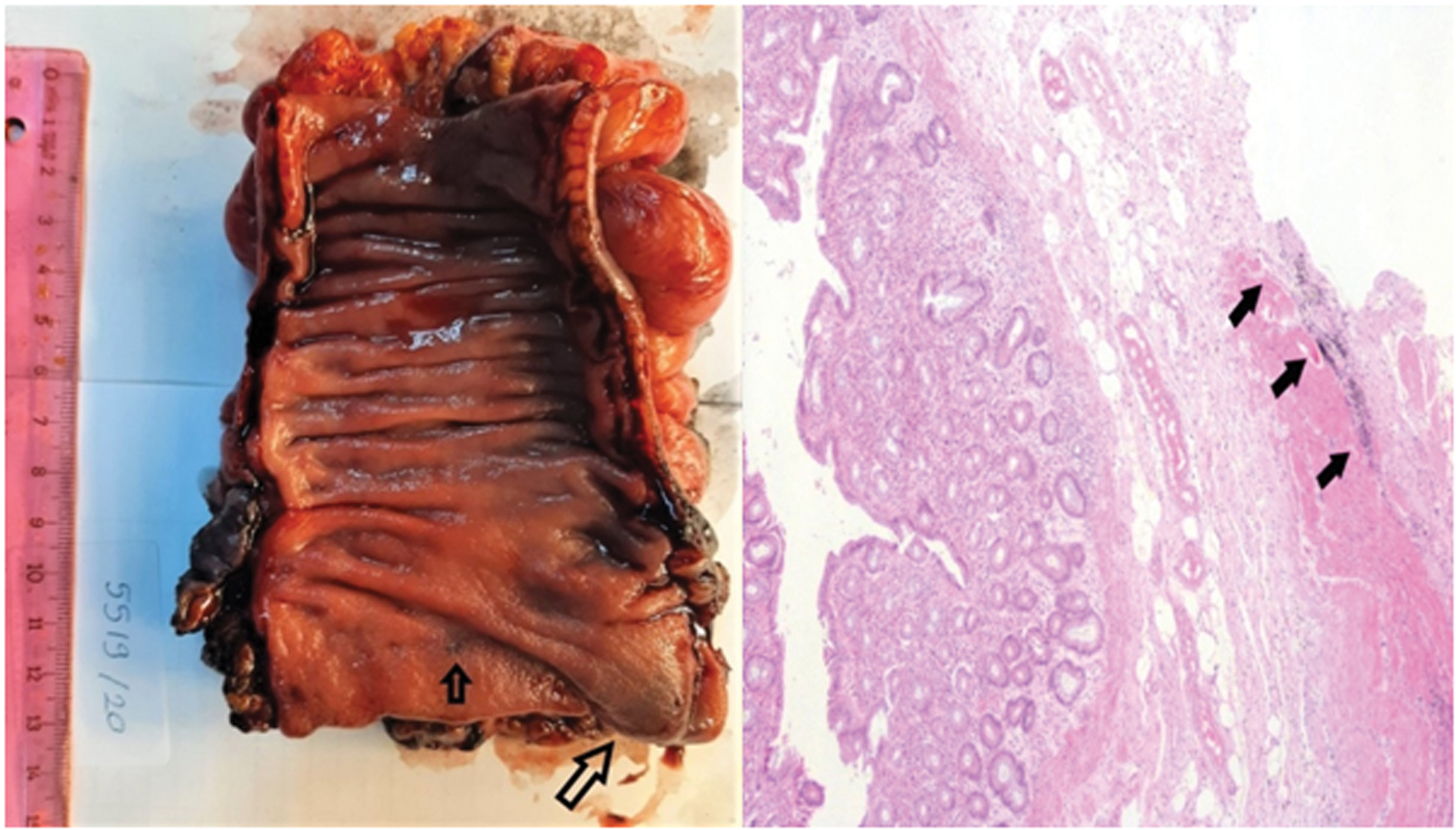
Macroscopic and microscopic images of tattooed rectum tumor resection specimen in a case with a clinical complete response. The appearance of the tattoo on the mucosal layer marked with arrows is shown on the left. A microphotograph of the black pigment of India ink is observed between regularly arranged structure of the mucosa, submucosa, and muscle fibers on the right. H&E, × 40. H&E, hematoxylin and eosin. Color images are available online.

A case with clinical complete response. Intraoperative and the sectioned macroscopic views of the nontattooed rectum specimen showing distal surgical margins. H&E, × 40. Color images are available online.
Comparison of the Rates and Averages of Histopathological Data
Normal distribution.
Non-normal distribution.
Values shown in bold signify p < 0.05.
LN, lymph node; ypT, pathological tumor stage after neoadjuvant chemotherapy.
It was found that endoscopic tattooing had a significant effect on DSM in the regression analysis (P = .06, R2 = 0.47). The surgical technique alone did not have a significant effect on DSM (group 1: P = .38 and group 2: P = .19). The results of the univariate analysis revealed that open surgery together with tattooing had a significant effect on DSM (P = .04, R2 = 0.71). In addition, univariate analyses showed that tattooing together with gender also had a significant effect on DSM (P = .009, R2 = 0.74). Analyses of all factors that have significant effects on DSM are summarized in Table 8.
Univariate Analysis of Factors Affecting the Distal Surgical Margin in Both Groups
Values shown in bold signify p < 0.05.
Discussion
Neoadjuvant CRT applied in locally advanced rectal cancer is currently accepted as the standard treatment due to increased local control rates, sphincter preservation, and higher disease-free survival rates. In the literature, 11%–57% of patients develop cCR after neoadjuvant CRT.7,8 The pCR occurs in 10%–30% of rectal cancer patients.4,9–13 Concurrent with the literature, cCR and pCR were achieved by 30.8% and 16.1% of the patients, respectively.
The mean operative time was significantly longer in patients with a BMI >30 kg/m2. Increased visceral fat in obese patients causes technical difficulties of the procedure in terms of differentiating mesenteric vascular structures, mobilization of the colon, and maneuvering within a limited space.14,15 Although there is no randomized controlled trial showing the relationship between obesity and operative time in a systemic literature review by Hotouras et al., multivariate analyses have shown that BMI is an independent predictive factor for operative time.14–18
Laparoscopic surgery enables wide radical resection by providing an improved visualization of the pelvic area and a magnified and well-lit view of the structures in the surgical field. It is noteworthy that laparoscopic surgery is more commonly used for mid and low rectal cancers. The COLOR II trial is the largest randomized study comparing laparoscopic and open surgery for rectal cancer. A total of 1044 patients who underwent TME were included in this study, and a significantly higher rate of radial margin positivity (9%) was observed after laparoscopic surgery than radial margin positivity (22%) observed after open surgery in low rectal tumors. The DSM positivity presented with similar rates after laparoscopic and open surgery. 19 In contrast, the CLASICC and COREAN studies reported more radial margin positivity in low rectal tumors in open surgery than in laparoscopic surgery.20,21 A prospective analysis reported by Baik et al. evaluated 2011 rectal cancer patients and indicated that the laparoscopic surgery group had better radial surgical margin distances, and similar DSM and LN rates compared with open surgery. 22
In this study, it was determined that the radial and DSMs differed according to gender in the tattooed group. Radial and DSMs in male gender were shorter than the female gender. In contrast, there was no relationship between gender and surgical margin in the nontattooed group. The analysis was performed by taking all cases into consideration, it was found that the effect of female gender and tattooing together on DSM was better. Pelvic dissection and rectal transection are more challenging in men than in women due to the narrow pelvic cavity. It has been reported that this situation constitutes an important risk factor especially for conversion and postoperative complications, and laparoscopic surgery is technically more demanding.23,24 From this point of view, the higher rate of laparoscopic surgery in the tattooed group may have contributed to the difference in surgical margins in the male gender. Owing to the lack of tactile sensation in laparoscopy, it is very important for the surgical team to have the lesion tattooed preoperatively. The desire to dominate the lesion area by using the feeling of palpation and the concern of missing any possible palpable lesions during surgery are the leading reasons for the choice of open surgical technique in patients with cCR who have not been tattooed preoperatively.
Limited access to the deep pelvis, the proximity of the anterior wall of the rectum to anatomical structures, and complex pelvic anatomy create surgical challenges.25,26 Regardless of the surgical technique, positivity of surgical margin and perforation rate increases during anterior dissection.27–29 Previous studies have examined a number of clinical features including male gender, high BMI, large tumor diameter, narrow pelvic cavity, history of pelvic radiation, and laparotomy; these are reported to be predictive factors for difficult pelvic dissection, increased conversion rates, postoperative morbidity, long operative time, positive surgical margins, and poor quality of the surgical specimen.30–36 Randomized clinical trials have reported that the surgical approach is not associated with difficult pelvic dissection.27,37,38 In this study, mean operative times were similar between the groups. Similar to the literature, the factors affecting the operative time were found to be high BMI and close radial surgical margins, as mentioned before. This study also showed that surgical technique alone is not an effective factor on operative time and surgical margins.
Accurate measurement of DSM is essential in cases of LAR, as the rectal tumor can be transected or the normal segment can be resected, leaving the tumor behind.39–44 Tumor regression after neoadjuvant therapy creates difficulties in differentiating the previous tumor site. 45 For this reason, methods such as intraoperative DRE or proctoscopy, and preoperative localization with endoscopic clips are used to determine DSM. However, these methods have disadvantages such as misplacement and migration of clips, dilated colon, and risk of microperforation during insertion.5,6,46 Endoscopic tattooing is the most commonly used method in colon tumors, but it is not frequently used in the localization of rectal tumors.44,47–53 The reasons are that rectum tumors can be accessed by DRE or proctoscopy due to their proximity to the anus, and the technical difficulty in identification of the dye due to the peritoneal envelope around the mesorectum.44,54 In a recent study evaluating 50 patients with preoperative tattoos, tattoo in the rectum wall and/or mesorectum could be observed in 40 patients. This study demonstrated that endoscopic tattooing is safer and more applicable for preoperative localization than other methods. 55 In addition, most of the studies have found that preoperative endoscopic tattooing is associated with shorter operative time and reduced blood loss.56,57
The anastomosis becomes technically more challenging for the surgeon if the distance of the resection from the anal verge increases in LAR. There is a tendency for VLAR–coloanal anastomosis involving excision of the total rectum to avoid “blind resection” especially in cases with cCR, and the surgery may have to be concluded with wide resections and increased morbidity.52,53,58 In a recent study involving 40 rectal cancer patients, DSMs in the tattooed group (mean ± SD 46.7 ± 16.4 mm) were found closer than in the nontattooed group (mean ± SD 62.9 ± 21.8 mm). In the study, it was reported that preoperative endoscopic tattooing prevented colorectal anastomoses to be made at very low levels and reduced protective ileostomy rates. 59
The DSMs were compared between the groups, and a statistically significant difference was obtained (group 1: 2.17 cm and group 2: 1.20 cm, P = .02). There are no studies suggesting endoscopic tattooing of the distal margin before neoadjuvant therapy to ensure the adequacy of resection in rectum tumors with cCR in the literature. The only study similar to the main idea of this study is about patients with cCR after neoadjuvant therapy reported by Torres et al. The study reported the cases underwent subsequent LAR after neoadjuvant therapy and had pCR in the resected specimen. The cases manifested tumor regrowth in the distal rectum in the early postoperative period that indicated the residual cancer remained in the distal portion of the anastomosis. 54 As a result, it was stated that endoscopic tattooing of the tumor before neoadjuvant therapy can simplify the process. 56
This study includes an extensive analysis involving the interaction of all variables with many factors that may be related to DSM. The main limitation of this study is not to have a large number of cases. Comorbid conditions, postoperative complications, and mortality of the patients were not included in the analysis because comorbid diseases are considered as factors that affect the operative time, conversion rates, postoperative morbidity, and mortality rates rather than providing a safe DSM. The recurrence rates were not included in this study because sufficient follow-up period is needed to analyze recurrence rates and adjuvant treatments and follow-ups of recent cases were not terminated due to time limitation.
Conclusion
Nowadays, it is expected that positive effects such as providing tumor regression and local control with neoadjuvant therapy in locally advanced rectal tumors, and the widespread and successful use of laparoscopic surgery bring additional problems. One of these problems is the difficulty in deciding the DSM during LAR due to complete tumor regression after neoadjuvant therapy. Understanding the distance and the relationships between tumor and anal sphincter before neoadjuvant therapy is the basis for an adequate resection, if the surgical plan was not initially established in the direction of APR. In locally advanced rectal cancer, endoscopic tattooing of the distal margin of the tumor before neoadjuvant therapy is a reliable and effective method for obtaining a safe DSM and not leaving the residual tumor at the lower end of the anastomosis, especially in cases of cCR.
Footnotes
Authors' Contributions
All authors have made substantial contributions to this article being submitted for publications. All authors critically reviewed the article and approved the final form.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.