
Abstract
Introduction:
Vertical banded gastroplasty (VBG) was a common bariatric procedure by laparotomy and or at the beginning of the laparoscopy, but nowadays it is almost an abandoned procedure. However, the young generation of bariatric surgeons should be aware about this procedure especially for revisional cases. Roux-en-Y gastric bypass (RYGB) is considered the procedure of choice for the revision of VBG.
Materials and Methods:
The evolution of revisional surgery to RYGB has known several technical steps. At the beginning, the procedure was performed with no gastric resection. Then a limited resection of the ancient staple line along with the fibrous tissue under the previous band or mesh was performed. The purpose of this article is to describe a simplified operative technique to simultaneously resect the ancient staple line and the calibration band.
Results:
After the initial viscrerolysis, an attempt to distinguish the course of the ancient section line of the stomach during the VBG is done. The dissection can become extremely challenging, with too much fibrosis and nonanatomical planes of dissection. At this point, we counsel to abandon the anterior direct dissection of the upper part of the stomach and to switch to a posterior dissection with the approach of greater curvature. Driven by the potential advantages (no risk of mucocele or gastrogastric fistula), for the past several years, we have changed the technique from resecting only the ancient staple line to perform a partial gastrectomy. The gastrectomy is larger and includes the complete resection of the gastric fundus, ancient staple line, the region with the mesh inside, and part of the gastric body. Once the stomach is extracted, the subsequent steps are similar to those of a primary RYGB.
Conclusion:
The procedure of choice for the revision of VBG is represented by RYGBP. Associating an atypical gastrectomy of the previous staple line with the region of mesh migration is a safe approach, eliminating the risk of mucocele.
Introduction
Vertical banded gastroplasty (VBG) and the gastric bypass were two of the most common bariatric procedures by laparotomy and the trends continued in the initial period of the laparoscopy, but nowadays it is almost an abandoned procedure. 1 However, the young generation of bariatric surgeons should be aware about this procedure, because VBG has a 29% to 56% incidence of revision in the long term.2,3 Common indications for revision are regain of weight due to staple-line disruption, gastric pouch and stoma dilation, change of eating habits to sweet eaters, and stenosis at the stoma outlet with vomiting and reflux.4–7
Roux-en-Y gastric bypass (RYGB) is considered the procedure of choice for the revision of VBG as well.3–8 Problems such as recurrent nausea and vomiting or severe gastroesophageal reflux resolve promptly after conversion. During the revisional procedure, a particular attention should be offered to the gastric pouch to avoid postoperative complications (e.g., mucocele and leaks). 8 Initially, a partial resection of the ancient staple line was proposed. The purpose of this article is to describe a simplified operative technique to simultaneously resect the ancient staple line and the calibration band.
Materials and Methods
The evolution of revisional surgery to RYGB has known several technical steps. At the beginning, the procedure was performed with no gastric resection. As described by Marmuse and colleagues, 8 after an initial period, we have decided to perform a limited resection of the ancient staple line along with the fibrous tissue under the previous band or mesh. When a silicone band is present, the withdrawal is easily performed, whereas no attempts are made to remove the mesh as it is often migrated and incorporated into the stomach wall.
Driven by the potential advantages (no risk of mucocele or gastrogastric fistula), for the past several years, we have changed the technique from resecting only the ancient staple line to perform a partial gastrectomy. The gastrectomy is larger and includes the complete resection of the gastric fundus, ancient staple line, the region with the mesh inside, and part of the gastric body.
Results
Any surgical history of laparotomy does not contraindicate the laparoscopic approach. The patient is placed in reverse Trendelenburg position and a five-trocar technique is used. The classical trocars position includes a 10-mm optical trocar in the umbilicus, a 5-mm subxiphoid port for the liver retractor, two operator trocars to the left and right of the midline, and a 5-mm assistant port is placed in the left anterior axillary line. Once the pneumoperitoneum is created by the open approach, an extensive adhesiolysis is started (Fig. 1) by dissecting the abdominal adhesions, especially between the liver and the stomach.
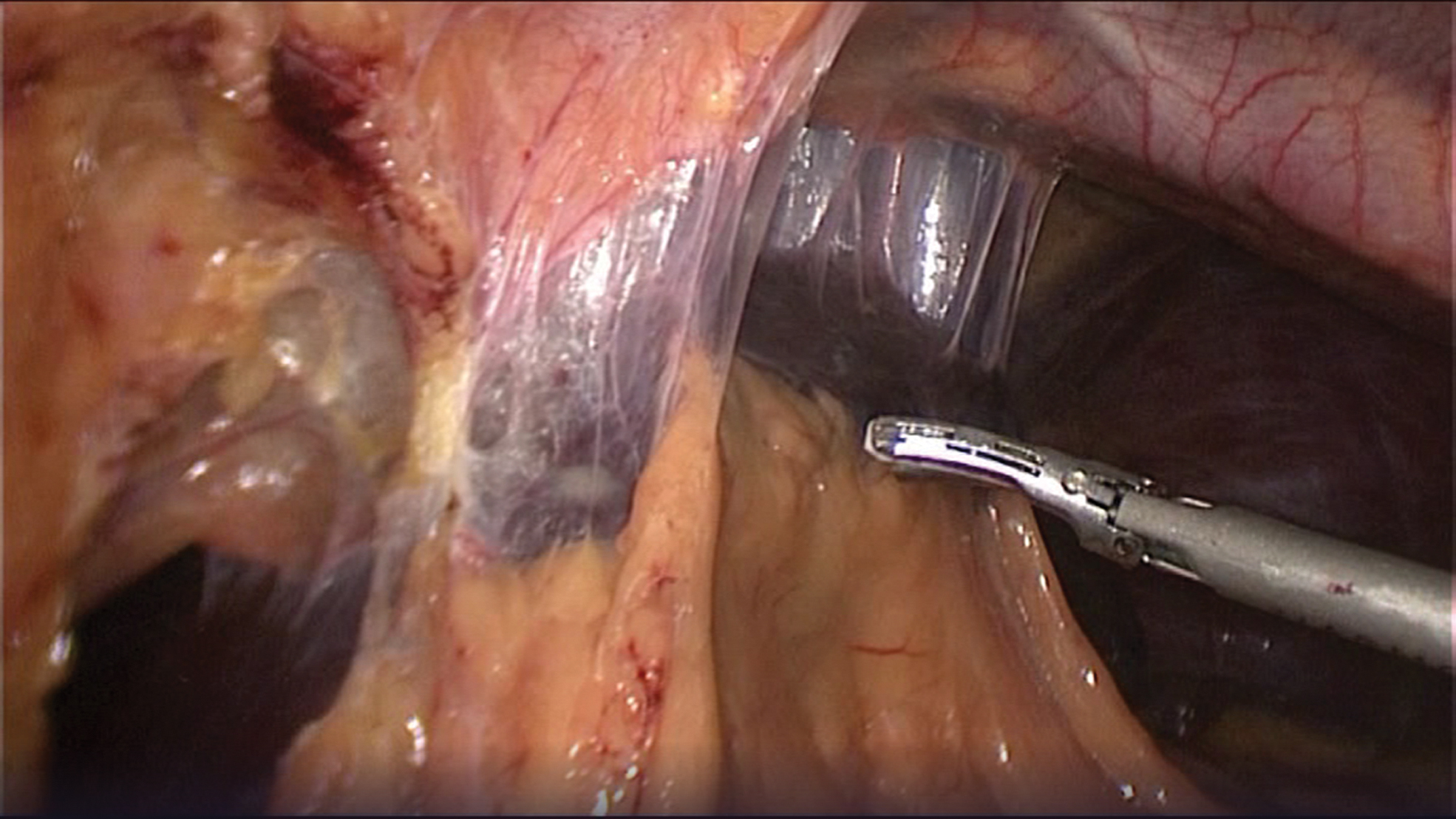
Initial aspect. Color images are available online.
The dissection advances carefully to the gastroesophageal junction and to the Hiss angle. Furthermore, an attempt to distinguish the course of the ancient section line of the stomach during the VBG is done. The dissection can become extremely challenging, with too much fibrosis and nonanatomical planes of dissection. At this point, we counsel to abandon the anterior, direct dissection of the upper part of the stomach, and to switch to a posterior dissection with the approach of the greater curvature. With the help of ultrasonic shears, we dissect the gastrocolic ligament, and we get into the omental bursa.
The gastric fundus is completely mobilized by dividing the short gastric vessels and the gastrophrenic ligament. This approach allows a less difficult dissection of the posterior adhesions consecutive to previous interventions in the supramesocolic floor. At the end of dissection, we should always see the left diaphragmatic crus. This is the anatomical landmark that allows us to say that the dissection of the fundus was complete (Fig. 2).

Identification of the left crus. Color images are available online.
After complete posterior mobilization, a window is created close to the stomach at the level of the lesser curvature, just above the stoma outlet. The maneuver to entry into the lesser sac is a lot facilitated by previous posterior mobilization. The dissection of the lesser curvature of the stomach is prolonged distally inferior to the lower border of the band/mesh placement. Then the stomach is transacted horizontally with the endoscopic stapler with a green cartridge proximal to the previous calibration.
The gastric pouch is created by cutting vertically the stomach medial to the ancient staple line. A particular care needs to be taken to avoid inadvertent crossing of the previous staple line. The refashioning of the gastric pouch can be technically challenging as it may result in the accidental creation of a “blind pouch,” which is a well-known pitfall of the conversion of VBG into RYGB.
At this moment, the stomach that will be resected (gastric fundus, the ancient staple line, and the part of the gastric body with the migrated mesh) is completely mobilized and well exposed as shown in Figure 3. The section of the stomach starts at the greater curvature and is completed toward the lesser curvature. The operative specimen is pulled out in a plastic bag and the extracorporeal dissection confirms the migration of the mesh inside the gastric wall (Fig. 4).
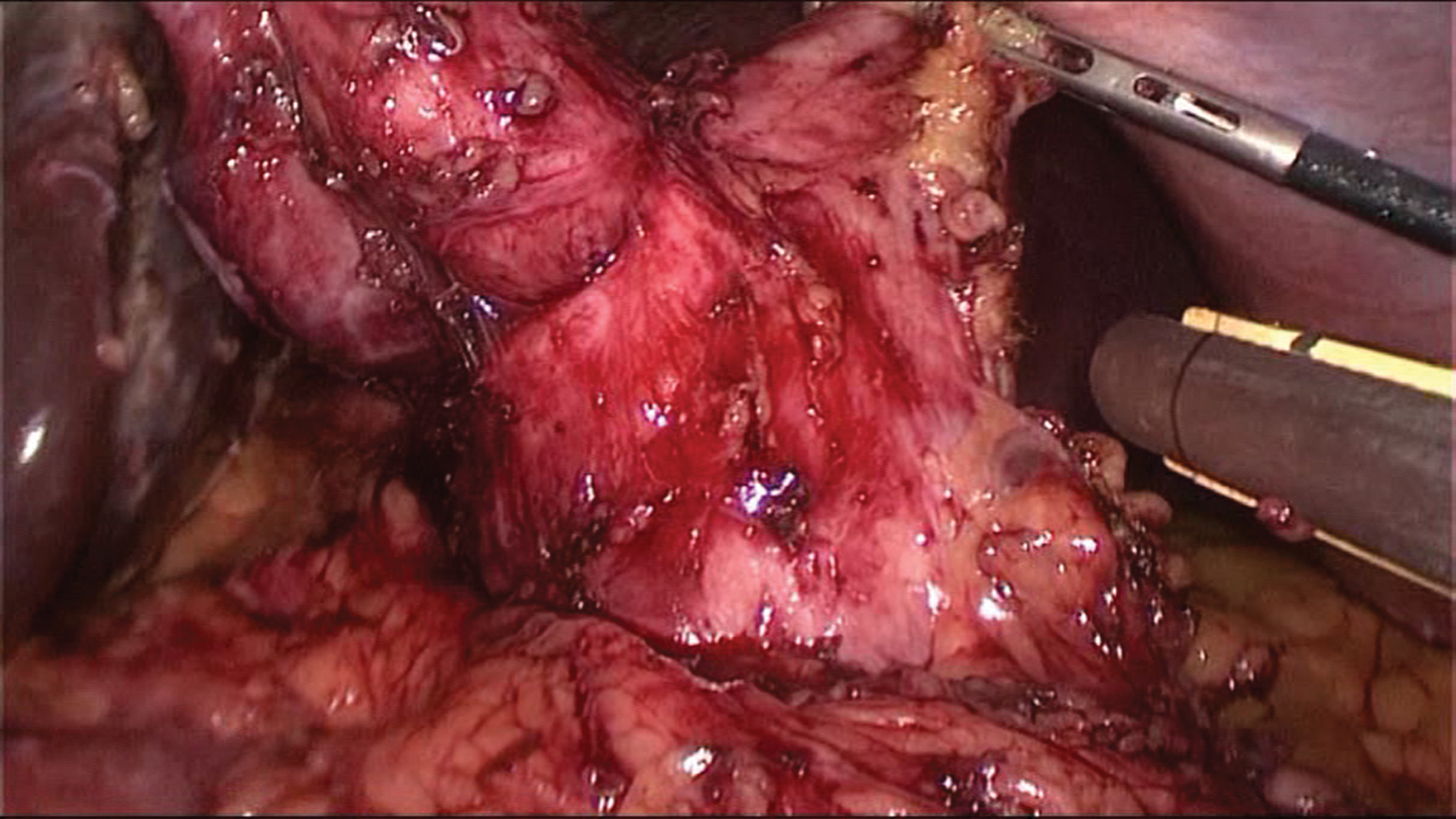
Complete mobilization of the stomach. Color images are available online.
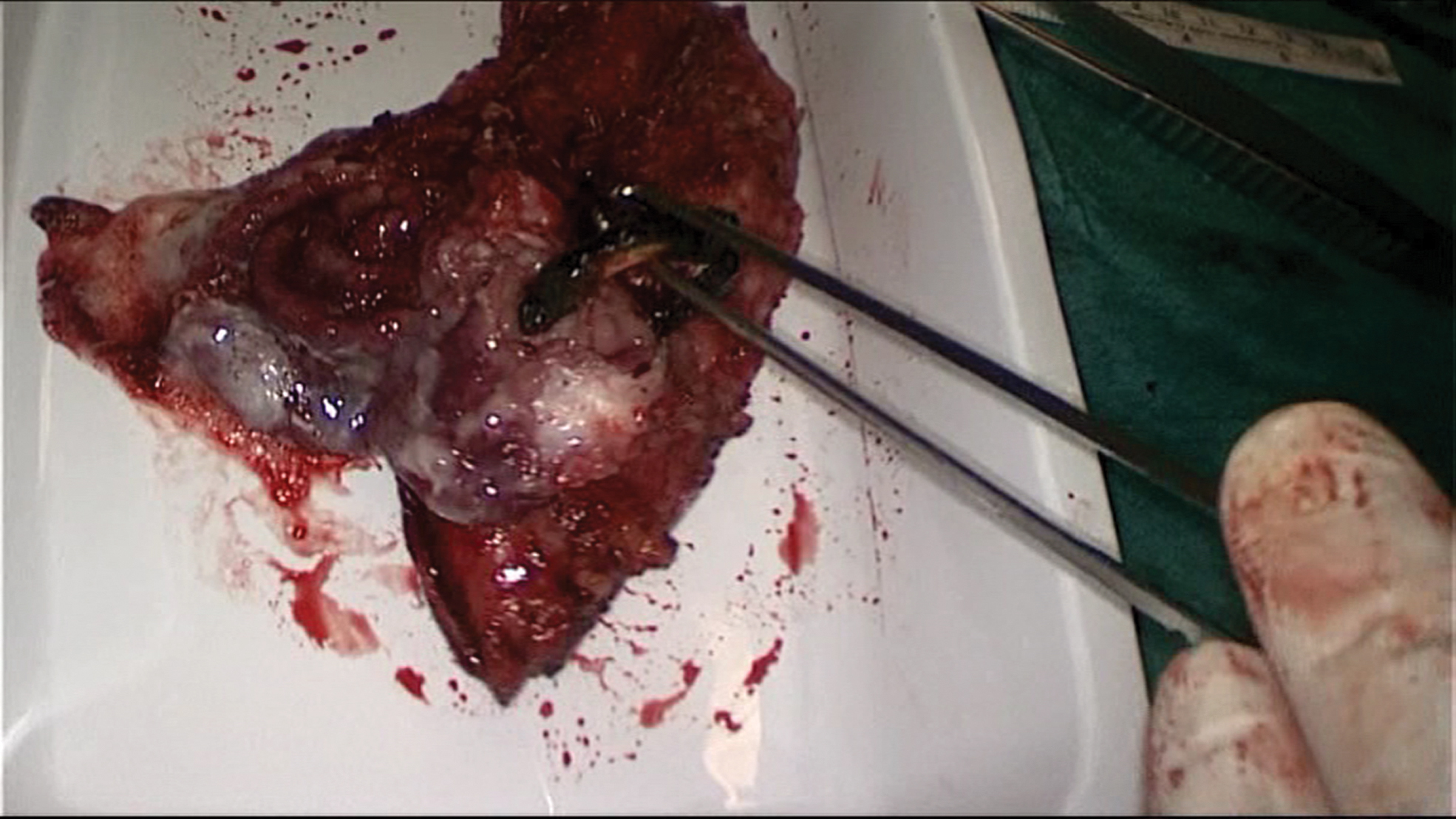
Partial migration. Color images are available online.
Once the stomach is extracted, the subsequent steps are similar to those of a primary RYGB. The Roux limb is prepared by dividing the proximal jejunum at a point of maximal mobility. A 100 cm long Roux-en-Y loop is fashioned 70 cm distal to the ligament of Treitz and brought up to the gastric pouch in an antecolic manner. A linear side-to-side gastrojejunal mechanical anastomosis is performed, and both mesenteric defects are closed.
Discussions
The frequency of revisional bariatric surgery will continue to rise during the next years. 1 Despite a previous report, 9 in our experience the conversion of VBG to sleeve gastrectomy is an absolute contraindication due to the high risk of stenosis and gastric leak. In the literature, the procedure of choice for the revision of VBG is represented by RYGBP.3,5,8,10,11 This type of gastric resection associated with RYGBP was proposed according to some potential advantages
The decrease of the ghrelin values and the increase in the glucagon-like-peptide-1 and peptide YY values by resection of the entire gastric fundus were already proved in several studies.8–10 Peterli et al. have shown a more important decrease in the ghrelin level in procedures associated with gastric resection such as sleeve gastrectomy compared with RYGBP with no gastric resection.
The risk of mucocele between the old staple line of McLean and the new calibration of the gastric pouch is canceled by creating the gastric pouch medially to the ancient staple line. The classical region of the mucocele is resected.
This technique diminishes the risk of gastrogastric fistula, the gastric pouch being completely separated from the gastric remnant.
By the resection of an important part of the gastric body, we probably decrease the risk of gastric cancer on the gastric remnant.
Conclusion
The procedure of choice for the revision of VBG is represented by RYGBP. Associating an atypical gastrectomy of the previous staple line with the region of mesh migration is a safe approach, eliminating the risk of mucocele.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.