
Abstract
Background:
Percutaneous internal ring suturing (PIRS) is a laparoscopic procedure that has demonstrated its safety and efficacy as a method of hernia repair in younger children but without evidence among the adolescent population. The aim of this study was to determine the success of PIRS outcomes for hernia repair in the adolescent population.
Methods:
All adolescents who were operated on using the PIRS method for inguinal repair during the 5-year study period in a single center were included in a prospective cohort study. The main outcome of the study included treatment outcomes in a term of recurrence rate. The secondary outcomes include other treatment outcomes such as complications, conversion to an open procedure, and reoperation rates, as well as duration of anesthesia and surgery, duration of hospital admission, and the level of carbon dioxide pneumoperitoneum.
Results:
In 51 adolescents (72.5% males) with a median age of 13 years and median follow-up of 44 months, a total of 57 PIRS procedures were performed. There were 30 (58.8%) right hernia repairs, 15 (29.4%) left hernia repairs, and 6 (11.8%) bilateral hernia repairs. The median surgical time was 10 minutes for unilateral and 18 minutes for bilateral hernia repair. The median length of hospital stay was 24 hours. Only one (1.95%) intraoperative complication occurred during surgery, an inferior epigastric vein injury. No complications or recurrences were observed during the follow-up period.
Conclusions:
PIRS has proven to be simple, safe, and effective method for groin hernia repair in adolescent population. This method provides excellent overall and cosmetic outcomes. There is a low incidence of complications and recurrences. According to our results, PIRS could be considered to become a possible approach for groin hernia repair in adolescents.
Introduction
Among the human population, the most common reason for admission into the surgical unit would be due to a groin hernia, with an incidence of 25% in the whole population. 1 There is a bimodal distribution of inguinal hernias with two peaks of incidence: first occurring in patients aged from 0 to 5 years, and second between the ages of 70 and 80 years. 1 After the age of 50 years, an increasing incidence of inguinal hernia has been reported.1,2 The surgical approach for treatment of inguinal hernia differs significantly between the children and adults. In the pediatric population, due to the predominance of indirect hernias, the standard of treatment is open or laparoscopic high hernia sac ligation, which carries extremely low recurrence rates.3–6 In contrast, as direct hernias dominate in adults, the surgical approach is completely different from that in children.
Today, open or laparoscopic tension-free hernioplasty using synthetic mesh became a standard of treatment of adult inguinal hernia.6–8
According to the World Health Organization, individuals from ages 10 to 19 years are considered adolescents. Given the above, adolescents who are no longer children and are not yet adults represent a “no man's land,” and there has not been a concise agreement among surgeons on the most appropriate method of surgical treatment for inguinal hernias in this age group. 9 The type of surgery performed in this specific age group is highly influenced by the operating surgeon's preferences. As is logical, adult general or abdominal surgeons most commonly repair these hernias using the same principles as in adults (mesh repair), whereas pediatric surgeons usually perform adolescent hernias repair without using mesh (a high sac ligation).9,10
Several potential complications may be associated with mesh use, for example, seroma formation, surgical site infection, and pain.7,9,11 Also, there are conflicting data in the literature regarding the effect of synthetic meshes on fertility.9,12 Having said that, the ideal outcome would be to avoid using mesh in adolescents with an inguinal hernia. Hernias are uncommon in this age group, and the literature is very limited regarding outcomes of treatment in adolescents undergoing hernia repair. Several studies demonstrated that both open and laparoscopic high ligation are effective modalities of treatment in adolescents with inguinal hernia with an acceptable recurrence rate.9–11,13,14 Moreover, increased chronic pain has been reported in adolescents when mesh was used for inguinal hernia repair. 11
Recently, percutaneous internal ring suturing (PIRS) has become a popular method for pediatric hernia repair. It has proven to have excellent outcomes and is a method with a fast learning curve.5,15 The median age in most of the reports is between the ages of 2 and 5 years.5,15–19 In the available literature, there are no data regarding outcomes of treatment using PIRS in adolescents. The goal of the present study was to evaluate the efficiency and long-term results of PIRS treatment in inguinal hernia repair in the young adolescent population.
Materials and Methods
Patients
Between October 1, 2015, and April 1, 2021, a prospective, single-center cohort study on 51 adolescents undergoing 57 PIRS procedures for inguinal hernia repairs was conducted. Inclusion criteria were all adolescents aged 10–17 years, who underwent PIRS for the repair of their inguinal hernia at the Department of Pediatric Surgery, University Hospital of Split, with a minimum of 6 months of follow-up. Patients were excluded from the study if they were out of the determined age range, patients operated on by open approach or a multiport laparoscopic approach. Also, patients were excluded if they had a follow-up of less than 6 months or if they had incomplete data.
For each patient, specific data were recorded: a complete medical history, general demographic data, hernia laterality, surgical details (intraoperative findings, additional trocar introduction, level of carbon dioxide [CO2] pneumoperitoneum, intraoperative complications), duration of surgery, length of anesthesia, extent of hospital stay, treatment outcomes, and recurrence rate.
Parents or legal guardians of the patients signed informed consent before inclusion to the study. The study was approved by the Ethics Review Board of our hospital with reference No. 500-03/20-01/09.
Outcomes of the study
The main outcome of the study included treatment outcomes in a term of recurrence rate. The secondary outcomes include other treatment outcomes such as complications, conversion to an open procedure, and reoperation rates, as well as duration of anesthesia and surgery, duration of hospital admission, and the level of CO2 pneumoperitoneum.
Study protocol, surgery, and follow-up
On the day of the operation, patients were admitted to the hospital. Their personal information was noted into the Study protocol, such as their demographic data and medical history. Over a period of 6 years, we evaluated the outcomes, recurrences, safety, and efficacy of the PIRS method. PIRS technique was described in our previously published studies (Fig. 1), with the only difference being that a 5 mm laparoscope (Olympus, Tokyo, Japan) was used.5,15

PIRS technique:
During their follow-up after the surgery, certain parameters were recorded, such as their degree of pain, duration of hospital admission, and any possible complications. Twenty-four hours after surgery, all patients were discharged. On weeks 1 and 4 after surgery, patients attended a follow-up appointment, where no recurrences or complications were noted. The follow-up regimen included a physical examination at 1, 3, and 6 months after operation. No potential late-onset complications or hernia recurrences were noted.
Methods of data collection and processing
The corresponding data were extracted from the study protocols. The Microsoft Excel for Windows Version 11.0 (Microsoft Corporation, Redmond, WA, USA) and SPSS 24.0 (IBM Corp, Armonk, NY, USA) software programs were used for data analysis. The median and interquartile range (IQR) were used for an asymmetrically distributed quantitative variable or an ordinal variable. To describe a distribution of a categorical variable, we used absolute and relative frequencies.
Results
Over the study period, 57 inguinal hernia repair procedures using PIRS were undergone by 51 adolescents, with an average follow-up time of 44 months (IQR 35, 51). The procedure was performed in 14 females (27.5%) and 37 males (72.5%) with an average age of 13 years (IQR 12, 16). The patients who have undergone hernia repair are distributed by their age at the time of the operation and can be found in Figure 2. The majority of the patients we encountered were 12 years old at the time of the operation (n = 10; 19.6%), and at this age, we found the most number of surgeries being performed.

Distribution of patients based on age at the time of surgery. Color images are available online.
The lowest number of operations was performed at the age of 11 years (n = 3; 5.9%). Table 1 contains a summary of patients' demographic data. There were 30 (58.8%) right, 15 (29.4%) left, and 6 (11.8%) bilateral hernia repairs. All procedures were performed by the PIRS method and were successful. No procedures required conversion to open repair. All repairs that are reported here were performed electively. The average duration of surgery for unilateral and bilateral hernias was 10 minutes (IQR 8, 14) and 18 minutes (IQR 14.5, 24), respectively (Fig. 3).
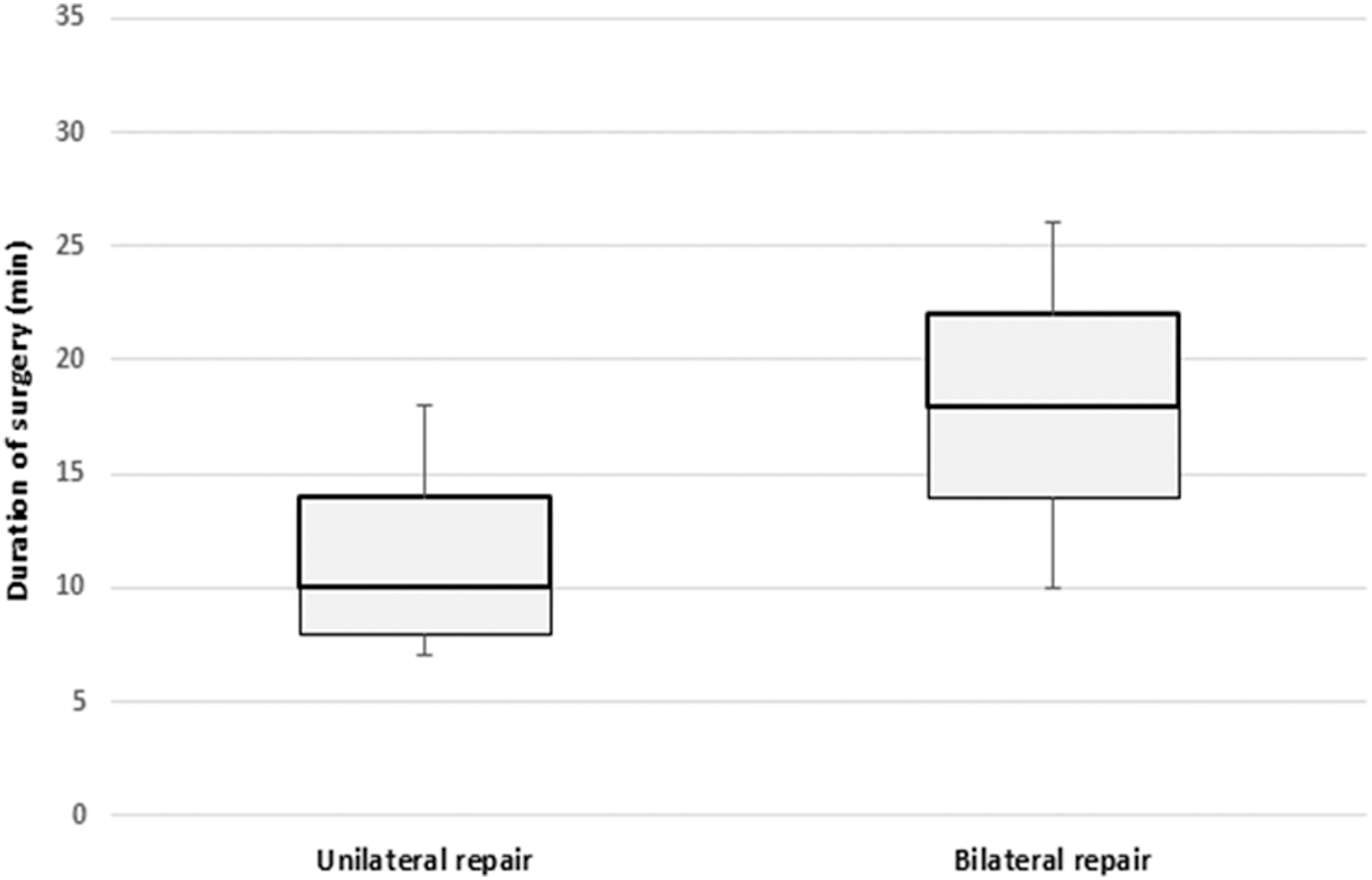
Comparison of duration of surgery for unilateral and bilateral repairs.
Patients' Demographic Data
ASA, American Society of Anesthesiologists, BMI, body mass index; IQR, interquartile range.
The median anesthesia time for unilateral and bilateral repairs was 24 minutes (IQR 21, 29) and 30 minutes (IQR 26, 37), respectively. The median duration of hospital stay after operation was 24 hours (IQR 8, 24). The average level of the CO2 pneumoperitoneum was 10 mmHg (IQR 10, 12). There was one (1.95%) intraoperative complication (Table 2). No postoperative complications, recurrences, or reoperations were recorded. The blood vessel injury was treated conservatively and without any consequence to the patient. No complications or hernia recurrence were found on follow-up visits.
Treatment Outcomes of the Patients
CO2, carbon dioxide; IQR, interquartile range.
Discussion
In this study, we evaluated the outcome of PIRS for the treatment of inguinal hernia among adolescents. The results of this study have proved that PIRS is a reliable and successful, minimally invasive method for treatment of inguinal hernias in adolescent patients. It has demonstrated to have outstanding outcomes, quick recovery, and a low incidence of complications and recurrences.
Of all ages of life, inguinal hernia incidence is lowest (<0.25%) in the adolescent population. 11 Due to this, study data on this population are extremely limited. Traditionally, open surgery was the most common procedure performed in this age range and was considered the gold standard of treatment.1,3,5,6 With the advancement of minimally invasive surgery, and the growing popularity among pediatric surgeons, it is important to validate that these techniques are not inferior to their open counterparts.4,14
PIRS is a method in which the internal inguinal ring is closed percutaneously, and it is performed under the guidance of a laparoscope placed in the umbilical port.
There are several advantages of laparoscopic surgery as opposed to open surgery, which includes avoidance of dissecting the vas deferens and spermatic vessels, significantly diminished pain, speedier recovery, and better cosmetic outcomes.5,15–19
All the studies published to date involving PIRS as the method of repair of inguinal hernias involve the pediatric population, where the average age of patients is 2–5 years.5,15–19 This study demonstrates the use of PIRS in adolescents aged 10–17 years. Adolescents lie in an intermediary zone between pediatric patients and adult patients due to their physical growth, development, and degree of physical activity. It is important that they do not experience postoperative restrictions and that they can resume daily functions. One study reported a return to normal on an average of 4 days after operation. 13
The pathophysiology of an inguinal hernia in adolescents is more similar to that in children than in adults. For this reason, in the past, they have been treated similarly. PIRS is proven to be a reliable and successful method for repairing inguinal hernias in children and now, in adolescents as well.
The aim of our study was to determine treatment outcomes in adolescent patients who had their inguinal hernias repaired using the PIRS technique. The success of a hernia surgery can be measured in various ways. One parameter is recurrence rate. Adult patients who undergo inguinal hernia repair with mesh may experience recurrences in ∼2%–5% of patients. 9 Children with inguinal hernias repaired by high ligation of the hernia sac in the open or laparoscopic approach can expect recurrences in 0.5%–4.0% of patients.3,5,15–19 However, data collection in adolescents is extremely limited. Moreover, increased chronic pain has been reported in adolescents when mesh was used for inguinal hernia repair. 11
In recent study, an acellular tissue matrix during Lichtenstein inguinal hernia repair was compared with high ligation of the inguinal hernia sac in adolescents. The authors reported no recurrences in a group of adolescents who received Lichtenstein repair using the acellular tissue matrix compared with a 6% recurrence rate in adolescents in whom high ligation of the sac was performed, but this difference was not statistically significant. They suggested that in this age group an individualized approach to the patients reduces recurrence rates. 20 Ninety-five percent of recurrences occur within 5 years, and this is within our study range. 13 Criss et al. reported that body mass index (BMI) may significantly influence recurrence rates in adolescents. 21 This was not a case in our patient sample. However, in this study, no recurrences were noted following the average follow-up of 44 months.
Another parameter that can be measured is complication rate. We recorded only one intraoperative complication. This may be attributable to the skill of a surgeon. It was previously reported that the total amount of complications in the PIRS method were significantly reduced after operating on 30–45 patients and achieved a minimum after 60 procedures. After performing 25–30 procedures per surgeon, the number of complications is very low. 15 The most frequent complications recorded for PIRS are intraoperative puncture of the blood vessels and postoperative hydrocele formation. 15
Previously, the initial usage of the PIRS technique had been associated with greater rates of ipsilateral recurrence and residual hydroceles. This could have been attributed to the inexperience of the operating surgeons or the use of absorbable or single sutures for very large defects.5,15,16,18,19,22 Also, complication rates are more frequent in premature infants and newborns compared with older age groups. 23 No cases of testicular atrophy or iatrogenic cryptorchidism after using the PIRS technique were recorded in the literature to the best of our knowledge. 24
In traditional laparoscopic hernia repair, it is necessary to place multiple trocars, and this has been associated with a prolonged surgery time due to intracorporeal suturing. This method can also increases postoperative pain and produce higher recurrence rates. The duration of a PIRS procedure is significantly lower than in classical three ports laparoscopic hernia repair. The average duration of operation for unilateral and bilateral repairs is 11–19 minutes and 18–24 minutes, respectively. 5 We recorded a median operative time of 8–14 minutes for a unilateral operation and 14.5–24 minutes for bilateral repairs in our study.
PIRS leaves a very cosmetically appealing result. Most patients report near invisibility of the scar after only a short time. Only very thin patients sometimes report that they can feel a subcutaneous suture. During the operation, a blunt needle is used to reach the peritoneum under direct vision, which avoids the anatomy of the groin structure. This produces less trauma and avoids leaving a surgical incision on the abdominal wall.5,15,16,18,19,22 In this study, we have not recorded any complications, such as suture granuloma, groin traction pain or discomfort, vas deferens injury, iatrogenic cryptorchidism, testicular atrophy, or hernia recurrence. Additionally, there is no need for tracheal intubation. Previous studies showed that the laryngeal mask airway is a valuable and sufficient device for the management of the pediatric airway for PIRS in children.25,26
Pain is a factor that affects patients' ability to return to normal functioning. One study reports that 6.7% of adolescents experience inguinal neuralgia after high ligation. Comparatively, 10%–11% of adults experience this. 13 A study involving children with a median age of 4.7 years reported inguinal neuralgia in 5.1% of patients. 27 None of the patients we have worked with have reported inguinal neuralgia. PIRS has led to a decreased level of pain, owing to a decreased surgical stress and inflammatory response. 22 PIRS is also not shown to affect or decrease testicular vascularization. 24
Our study is limited by having a relatively small population size involving patients with a healthy average BMI and no preexisting medical conditions. More research should be undertaken to determine would changing these parameters affect the outcomes of procedures. Another possible limitation is a single-center design of the study. Additional investigation should be taken to determine the effects of an adolescents' comorbidities on inguinal hernia repair, such as cardiac or gastrointestinal comorbidities, and the potential benefits of this minimally invasive method of repair with their chronic conditions, as the shorter operation time may be an attractive option in this population.
Conclusions
PIRS has proven to be an efficient, uncomplicated, and reliable method for inguinal hernia repair in adolescents. This method provides excellent overall and cosmetic outcomes. There is a low incidence of complications and recurrences. According to our results, PIRS could be considered to become a possible approach for groin hernia repair in adolescents.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.