
Abstract
Duplication anomalies of the kidney represent common congenital malformations of the urinary tract. A duplex kidney has often one pole that is poorly or nonfunctioning. In this last case, surgery may be indicated to remove the nonfunctioning pole. The most common indications for partial nephrectomy in pediatrics include symptomatic vesicoureteral reflux to the nonfunctioning pole and/or ectopic ureter or ureterocele causing urinary incontinence. In this article, we describe the technique of laparoscopic partial nephrectomy in infants and children with duplex kidney. A surgical procedure properly executed following critical technical steps is the key factor for the success of surgery.
Introduction
Duplex kidney is a congenital anomaly of the urinary tract commonly encountered in pediatric patients and is usually asymptomatic if uncomplicated. It becomes symptomatic when it is complicated by vesicoureteral reflux (VUR), ureterocele, pelviureteric junction obstruction (most commonly in the lower pole) and ectopic ureteric insertion causing wetting in girls. 1
A duplex kidney has often one pole that is poorly or nonfunctioning. In this last case, surgery may be indicated to remove the nonfunctioning pole. 2 The surgical treatment of pediatric patients with duplex kidney depends on different factors such as the parenchymal function of each renal unit and presence of concomitant anatomic abnormalities, such as ectopic ureterocele or VUR.3–5 Currently, different surgical approaches can be used to perform partial nephrectomy such as posterior retroperitoneal, lateral retroperitoneal, laparoscopic transperitoneal and more recently robotic approach.6–8
In our experience, in case of duplex kidney with a nonfunctioning pole, laparoscopy represents the approach of choice to treat this pathology.2,9
This chapter is focused on the operative technique of laparoscopic partial nephrectomy (LPN). This study received the appropriate Institute Review Board (IRB) approval.
Materials and Methods
Preoperative phase
Preoperative workup includes renal ultrasound (US), dimercapto succinic acid (DMSA) renal scan, and/or a magnetic resonance urogram. A cystoscopy may help to clarify the anatomy in selected cases. In infants and small children (<15 kg), we usually perform preoperatively a bowel preparation using simethicone, enema, and low-residue diet.
Furthermore, antibiotic prophylaxis should be administered preoperatively either with a broad-spectrum medication or according to the child's specific urine testing.
Parents must sign a specifically informed consent before surgery.
The surgical procedure is performed under general anesthesia with orotracheal intubation and myorelaxation. A Foley bladder catheter and a nasogastric tube are placed just before surgery.
Positioning
For LPN, the patient should be placed in a semilateral decubitus position, with the ipsilateral side elevated using a pad underneath. The surgeon and the assistant stand in front of the patient, facing the pathology and the monitor on the patient's back (Fig. 1). This positioning uses the gravity to let the colon fall down, allowing an easy dissection of the ureter downward till the bladder entry and a safe access to the hilar vessel. A 10-mm 30° laparoscope is adopted as we usually extract the resected moiety through the optic orifice. We usually start the procedure using three trocars, and in case of challenge we add a fourth port, more frequently on the right side to retract the liver or alternatively on the left side to retract the spleen or the loops. We prefer to adopt 5-mm working trocars so as to use intraoperatively a clips applier for vessel control, a sealing device, or a peanut, which has 5-mm diameter. The trocars are placed in triangulation with the optic to have a better ergonomics (Fig. 2): one 10-mm port is placed transumbilically for the optic and two 5-mm working ports are introduced in the upper and lower quadrant, ipsilaterally to the pathology side.

The patient is positioned in semilateral decubitus on the operative table with the screen on his back and the surgeon and the assistant in front of him. Color images are available online.
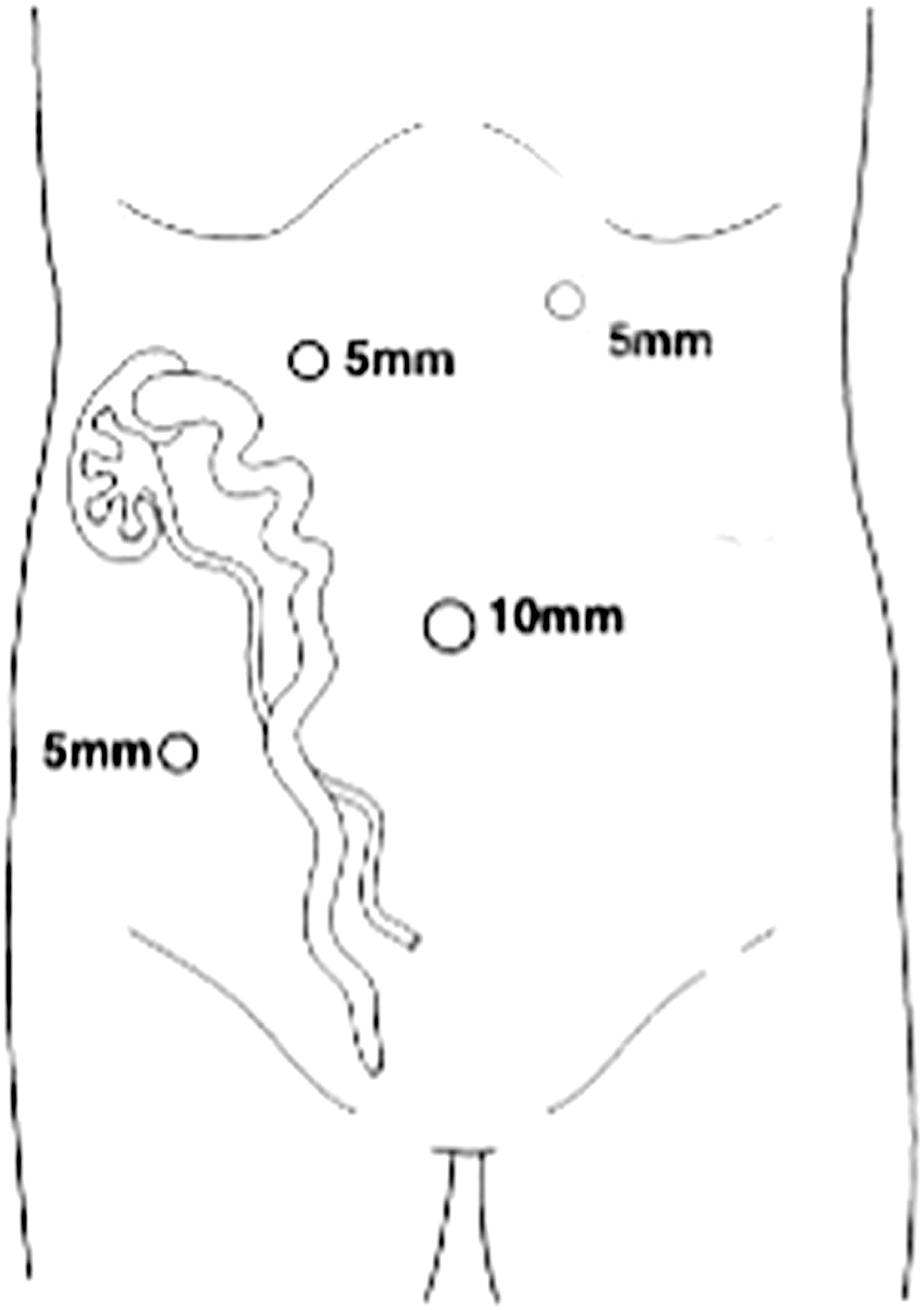
We prefer to use four trocars: one 10-mm 30° optic trocar in the umbilicus and two 5-mm working trocars and a fourth 5-mm trocar to retract the liver or the spleen.
Technique
Step 1—Cystoscopy
Before starting laparoscopy, we usually perform a cystoscopy to introduce an open-end ureteral catheter into the ureter of the normal functioning pole, which is helpful intraoperatively to easily identify the ureter of the functioning moiety and avoid injuring it during the dissection of the nonfunctioning moiety ureter. A 9.5F operative cystoscope is adopted in this step. More recently, before starting ureteral dissection, we inject an indocyanine green (ICG) solution into the ureteral catheter, to better identify the ureter of the normal moiety using the ICG fluorescence technology.
Step 2—Colon detachment and ureteral isolation
In the laparoscopy phase, as the loops slide down due to the semilateral decubitus position, the Toldt's line is incised and the colon is detached and lowered. Then, the Gerota's fascia is opened to access the kidney. Alternatively, a transmesocolic approach can be adopted to access the kidney, but it may be challenging especially in older children due to the presence of abundant fatty tissue in the meso and increased risk of vascular injury. For this reason, we prefer to detach the colon. This step can be performed using monopolar electrocautery or a sealing device that allows a faster and safer surgery without bleeding. After division of the Gerota's fascia, the ureter of the affected pole is isolated and dissected upward to the kidney. After ICG injection into the ureteral catheter, the ureter (green) is more easily identified and isolated (Fig. 3).

The ureter of the normal moiety view using standard view (left) and ICG view (right). ICG, indocyanine green. Color images are available online.
Step 3—Nonfunctioning moiety isolation
Thereafter, the affected moiety is isolated and its vascularization is identified and isolated separately. During this phase we prefer to adopt ICG fluorescence technology: the ICG solution (dosage 0.3 mg/mL per kg) is injected into a peripheral vein and in a matter of 30–120 seconds the kidney vascularization is easily identified using fluorescence (Figs. 4 and 5). Once identified, the vessels of the nonfunctioning pole are clipped and divided. Another option to manage the vessel is to seal them using sealing devices.
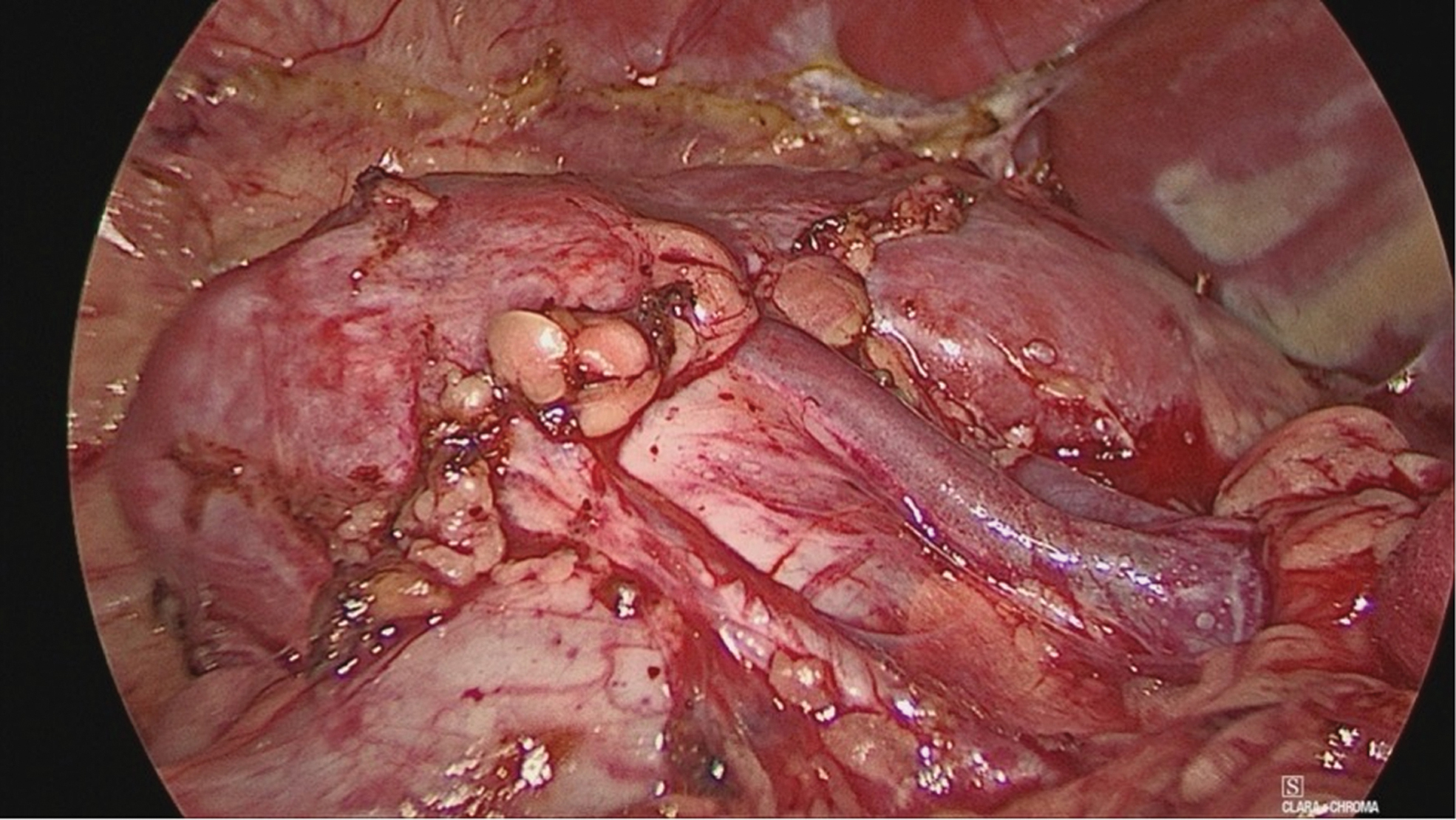
View of the main renal vessels and two lower pole vessels at standard white light imaging in a lower pole partial nephrectomy. Color images are available online.
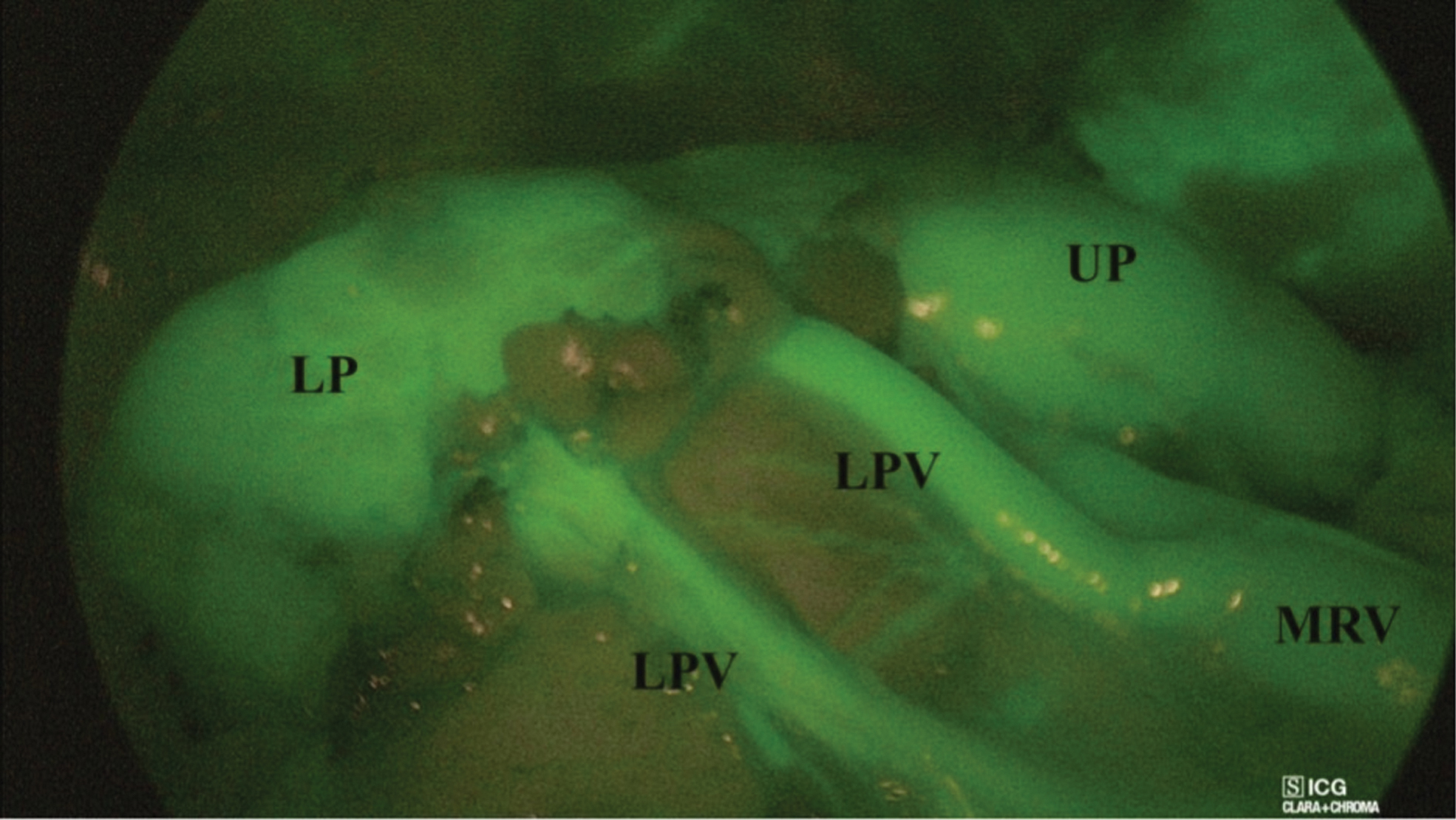
Using ICG-enhanced fluorescence, the renal vessels and renal parenchyma appear green. ICG, indocyanine green; LP, lower pole; LPV, lower pole vessels; MRV, main renal vessels; UP, upper pole. Color images are available online.
Step 4—Nonfunctioning moiety resection
After the vessel ligation, a demarcation line shows the transection plane between the normal and the ischemic pole. In this step, we also use ICG-enhanced fluorescence, which is very helpful to delineate the anatomical boundary plane between the two moieties and finally check the perfusion of the normal moiety after the parenchymal resection (Fig. 6). The nonfunctioning moiety can be easily sectioned using sealing devices (Fig. 7).

ICG-enhanced fluorescence allowed to identify the demarcation line between the normal lower pole and the ischemic upper pole. ICG, indocyanine green. Color images are available online.

After vessel ligation, the nonfunctioning upper pole moiety is resected using sealing device. Color images are available online.
Step 5—Distal ureter isolation and ligation
After the parenchymal division, the ureter is isolated downward till the bladder dome. If VUR is present into the affected kidney moiety, the ureter should be isolated as far down as possible to the bladder base and ligated, using preferably an endoloop. If VUR is not present, the ureter is sectioned as far down as possible and left open.
Step 6—Nonfunctioning kidney and ureter removal
After the distal ureter division, the dissection of the nonfunctioning moiety is completed and the removed moiety with the ureter are extracted through the umbilical orifice.
Step 7—Final check and drain placement
The residual kidney is checked at the level of the resection plane to search for urinary leaks. Methylene blue dye can be injected through the ureteral catheter and in case of leaks, the identified opening of the residual collecting system can be sutured. Another option is to apply a nebulized biological glue to seal the resection line. An indwelling abdominal drain can be placed to assess postoperative urinary leakage.
Postoperative care
Oral feeding is reintroduced about 3 hours postoperatively. Analgesic requirement is very short: paracetamol (dosage 15 mg/kg at 8-hour interval) is usually administered for 12–24 hours postoperatively. Antibiotic therapy is performed until hospital discharge. Length of stay is about 2–3 postoperative days (POD), after the removal of bladder catheter and abdominal drain. During the follow-up, clinical controls are performed on 7th and 30th POD and thereafter annually. A renal Doppler US is performed 1 month and 1 year postoperatively to check the vascularization of the remaining kidney. A renal scintigraphy is performed 1 year postoperatively to evaluate the parenchymal function of the remaining pole.
Results
In our series, the median operative time was 95 minutes (range 80–125). The conversion rate of the procedure that is performed in our surgical unit by senior surgeons with strong laparoscopic background was 0%. It is important to underline that surgeons should accomplish this procedure only after a robust experience with total nephrectomy.
A recent multicenter study coordinated by our group 2 reported a 19.2% postoperative complications rate. They included four urinomas, two symptomatic refluxing distal ureteral stumps, and four urinary leakages, and were classified grade two according to Clavien–Dindo classification. 10 No conversions to open surgery or intraoperative complications occurred in our series. The delayed urinary leakages were treated conservatively, leaving the bladder catheter and the drainage in situ until the complete resolution (maximum 10 days).2,9 In the same series, in 1 patient undergoing upper pole partial nephrectomy, the urinary leakage was identified intraoperatively. After injecting methylene blue dye into the ureteral catheter, the leakage site into the residual collecting system was identified and sutured using interrupted stitches. 2
The remaining complications (four urinomas and two symptomatic refluxing distal ureteral stumps) resolved spontaneously or using antibiotics and did not require any reoperations.2,9
At follow-up, renal Doppler US showed a normal residual kidney without parenchymal thinning or other anomalies in all patients, at 1 month and 1 year postoperatively. Renal scintigraphy reported no loss of function of the residual kidney (mean postoperative value: 37.8% versus mean preoperative value: 38.1%).2,9
Analyzing the literature of the past 10 years describing the outcome of LPN in children,6–8 no conversions were reported in all series. The median operative time ranged between 90 and 198 minutes whereas the median complications rate ranged between 7.4% and 52.9%.2–9,11–18
Discussion
LPN is technically more challenging than total nephrectomy. 13 Advanced technologies available on the market as HD cameras, miniaturized instruments, special sealing devices, ICG fluorescence technology, and biological glues are essential tools to perform partial nephrectomy in a safe way.12,19 In particular, new imaging technologies such as ICG-enhanced fluorescence allow easier intraoperative visualization of the kidney anatomy and its vasculature and subsequently safer dissection of the anatomic structures.7,19 Excluding tumors, the main indication for partial nephrectomy in children is the presence of complicated duplex kidney, with symptomatic VUR or ectopic megaureter/ureterocele causing incontinence. These conditions justify the indication to remove the nonfunctioning upper or lower pole. 7
This procedure is technically demanding and is also associated with a considerable risk of complications. In fact, during the dissection of the affected pole, there is the risk to injury the vasculature of the residual pole and the risk of urine leakage at the level of the parenchymal resection plane or the residual distal ureteral stump. 7
After the first description in the pediatric patients by Jordan and Winslow in 1993, 18 this procedure has reached a greater diffusion compared with the open approach, due to reported advantages of decreased length of stay, lower analgesic requirements, and better cosmetic results. 11 The procedure can be accomplished through a retroperitoneal or transperitoneal approach. 9 Although there is no evidence in the literature about the superiority of laparoscopy over retroperitoneoscopy to perform partial nephrectomy, it seems that laparoscopic approach is technically easier and more affordable than retroperitoneoscopy. 9 The most frequent complications reported in our LPN series were urinoma and prolonged urinary leakage from the parenchymal division line or the residual distal ureteral stump. 2 This leakage may be caused by the incomplete division of the affected moiety with persistence of excretive structures or by the opening of the collecting system of the residual moiety. Based on our experience, we believe that the prolonged leakage was more probably caused by an excessive peritoneal secretion secondary to colon detachment and mobilization. A trick that we adopted in our experience to avoid this complication was to inject methylene blue dye into the ureteral catheter placed into the normal ureter to check the integrity of the parenchymal resection line. In case of identification of a leakage point, this can be easily sutured or sealed using nebulized biological glue. The use of ICG-guided fluorescence imaging was very helpful to delineate the transection plane between normal and affected pole and perform a more precise parenchymal division.
In our experience, another common finding during the follow-up of children underwent LPN was the evidence on US of a simple anechoic cyst at the operative site, which occurred in about 50% of cases. The exact etiology of these cysts is unknown, but the most common hypothesis is that a seroma takes the place of the removed pole. In most cases, these cysts did not require any surgical treatment, remained unchanged or involved spontaneously 3–4 years after surgery. Based on our experience, we only advise annual clinical and US follow-up in patients who develop these cysts after LPN.
Other complications occurred in our series included breakthrough UTIs secondary to symptomatic residual distal ureteric stumps.2,9 For this reason, it is extremely important in case of associated VUR to isolate the ureter as far down as possible to the bladder entry and ligate it using clips or loops to avoid VUR into the residual stump. The transperitoneal approach to LPN and the use of a 30° optic provided the advantages of an excellent exposure of the kidney anatomy and hilar pedicle. Furthermore, the ICG-guided fluorescence was very helpful in different steps of the procedure: to identify the normal ureter and avoid its damage during dissection of the affected ureter; to identify the vascularization of the nonfunctioning moiety, delineate the transection plane after vessel division, and check the perfusion of the residual kidney after parenchymal resection.
In conclusion, our experience confirmed that LPN was technically easier compared with other minimally invasive approaches such as retroperitoneoscopy or prone position, but it is still considered a demanding procedure performed only in advanced pediatric centers with a robust experience in minimally invasive surgery. The main advantages of the transperitoneal approach included the clear identification of the urinary tract, the excellent exposure of the renal vasculature and the possibility to perform a total ureterectomy till the bladder entry.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.