
Abstract
The incidence of gallbladder disease in children is rising due to an increase in the development of nonhemolytic cholelithiasis in this age group. Laparoscopic cholecystectomy is the gold standard for treatment for gallbladder disease in adults and, with the technique's widespread adoption, it has now become the mainstay of treatment for gallbladder disease in children as well. Complications are infrequent and is now often performed as an outpatient surgery. Although the standard approach is through a 4-port technique, it can also be performed using a single-site technique. We describe our thoughts on laparoscopic cholecystectomy in children with a focus on the standard approach.
Introduction
Gallbladder disease in children has become increasingly more common for the past several decades. Similar to adults, the primary cause for gallbladder disease in children is cholelithiasis, although the incidence of pigmented stones from hemolytic disease is higher in compared with adults. 1
Furthermore, the presence of significant inflammation with acute and/or chronic cholecystitis is less common in children. However, the increase in gallbladder disease in children is due to the rise in nonhemolytic cholelithiasis from the Western diet and due to the recognition of biliary dyskinesia as a cause for gallbladder disease in this age group.2–4
Children >3 years of age with symptomatic gallbladder disease should undergo cholecystectomy. Surgical approach can be open or laparoscopic. The movement toward minimally invasive surgery began with the laparoscopic cholecystectomy; therefore, it has become the standard of care.5–10 Benefits of the laparoscopic approach include less discomfort, decreased length of hospital stay, improved cosmesis, and a faster return to activities. Therefore, we describe our operative technique of laparoscopic cholecystectomy.
Pre-operative Phase
The gallbladder is best evaluated by ultrasound (US). Sensitivity and specificity are >95% for detecting gallstones, although its accuracy is lower in children than adults.11,12 It also permits the evaluation of the hepatic ducts and the common bile duct (CBD) for the identification of stones or obstruction, in addition to other abnormalities in the liver or pancreas. Although a computed tomography (CT) scan can define the gallbladder inflammation and stones, delineation of the CBD is suboptimal with an abdominal CT and exposes children to unnecessary radiation. 13 The diagnosis of acute cholecystitis is made if the US reveals inflammatory changes such as a thickened gallbladder wall >4 mm, the presence of pericholecystic fluid, or a positive sonographic Murphy sign (tenderness with probe placement directly over the gallbladder). The diagnosis of symptomatic cholelithiasis is made if the US shows gallstones without inflammatory changes and is associated with symptoms.
For a patient with symptoms and examination findings consistent with acute cholecystitis but without stones on US, cholescintigraphy (hepatobiliary iminodiacetic acid [HIDA] scan) should be performed.99mTc-labeled iminodiacetic acid or an analogue is injected peripherally, is taken up by hepatocytes and processed by the same mechanism as bilirubin, which is then excreted in bile. This study is helpful in two ways. The diagnosis of acute cholecystitis is made if the gallbladder does not fill but the biliary tree is illuminated. False positives can occur in critically ill fasting patients and the use of intravenous morphine, which constricts the sphincter of Oddi enhancing gallbladder filling, can improve visualization of the gallbladder. In addition, a HIDA scan can allow calculation of the gallbladder ejection fraction with cholecystokinin-assisted or lipomul challenge. A normal gallbladder ejection fraction is ∼75%. A diagnosis of biliary dyskinesia is made if the ejection fraction is <35%.
Positioning
The patient is placed supine on the operating table. Two monitors are placed at the head of the table. Historically, decompression of the stomach is achieved with orogastric tube placement but this not necessary, nor is placement of a urinary catheter. 14 The surgeon operates from the patient's left side. A 10-mm umbilical port is the only large port needed to facilitate removal of the gallbladder from the abdomen, but a 5-mm telescope can be used to avoid switching scope sizes later. A 5-mm port, inserted in the epigastrium usually just to the right of midline (but more left in young patients for more working space), is the main operating port, allowing for the application of endoscopic clips to the cystic duct and artery. In children, if a 5-mm clip cannot adequately cross the duct, then the anatomy should be re-examined to assure this structure is, indeed, the cystic duct. Two additional instruments are positioned in the right abdomen in varying configurations for retraction of the gallbladder fundus cephalad and the infundibulum laterally. These instruments can be introduced without a port through a stab incision if the patient is not obese as these two instruments are not exchanged during the operation. This allows either 3- or 5-mm instruments to be introduced through very small incisions in lean or younger patients. 15 We position one of these ports near the midline between the two midline ports (umbilical and epigastric), so the surgeon does not have to reach across the patient very much, and the other is situated in the right mid-abdomen to facilitate cephalad retraction of the fundus.
Technique
Adequate cephalad retraction of the fundus and lateral retraction of the infundibulum allows visualization of the triangle of Calot without the need for repositioning the patient. Blunt dissection starts at the level of the gallbladder, which ensures accurate identification of the cystic duct regardless of how short or anomalous its course. Dissection is performed until the critical view of safety is visualized. This is important to correctly delineate the anatomy. The critical view is bounded by the CBD medially, the cystic duct inferiorly, the gallbladder laterally, and the liver superiorly.16–18 (Fig. 1). Ligation of the cystic duct is achieved with endoscopic clips and then divided between the clips so as to avoid CBD injury. Similarly, the cystic artery is ligated and divided. However, the cystic artery divides into anterior and posterior branches and if the artery is taken distally as it enters the gallbladder, it is small enough to be divided with cautery. This is done by grasping with the Maryland dissecting instrument to cauterize, then dividing it away from the CBD with monopolar cautery. Next, the gallbladder is dissected off the liver bed using cautery. Before complete mobilization from the liver, the dissection bed should be inspected to ensure hemostasis, and then the gallbladder is completely detached. If a 10-mm telescope was being used through the umbilical port it is exchanged for a 5-mm scope, which is then inserted into the 5-mm epigastric port. The specimen can then be extracted through the umbilical incision without using an endoscopic bag if there is little to no inflammation.

These four pictures depict the salient points for a laparoscopic cholecystectomy.
Although most surgeons utilize a 4-port approach, single-site laparoscopic cholecystectomy has also been described. For this approach, all instrumentation is placed through the umbilicus, resulting in a single 2-cm incision. In the United States, there are two main premanufactured ports used. The two devices are the SILS Port (Covidien, Norwalk CT) or the TriPort (Olympus America, Center Valley, PA) (Fig. 2). The SILS Port is a foam port with three working channels. An additional 3- or 5-mm instrument can be placed just to the left of the port. Use of a long telescope with this approach is helpful so that the assistant holding the telescope does not interfere with the operating surgeon. Another option is to place a single (usually 5-mm) port in the umbilicus with the additional instruments inserted through the fascia surrounding the port. Another option is to introduce individual low-profile 5-mm ports. Regardless of the technique and orientation of the instruments in a single-site approach, the principles of the procedure are the same as for the standard 4-port laparoscopic cholecystectomy.
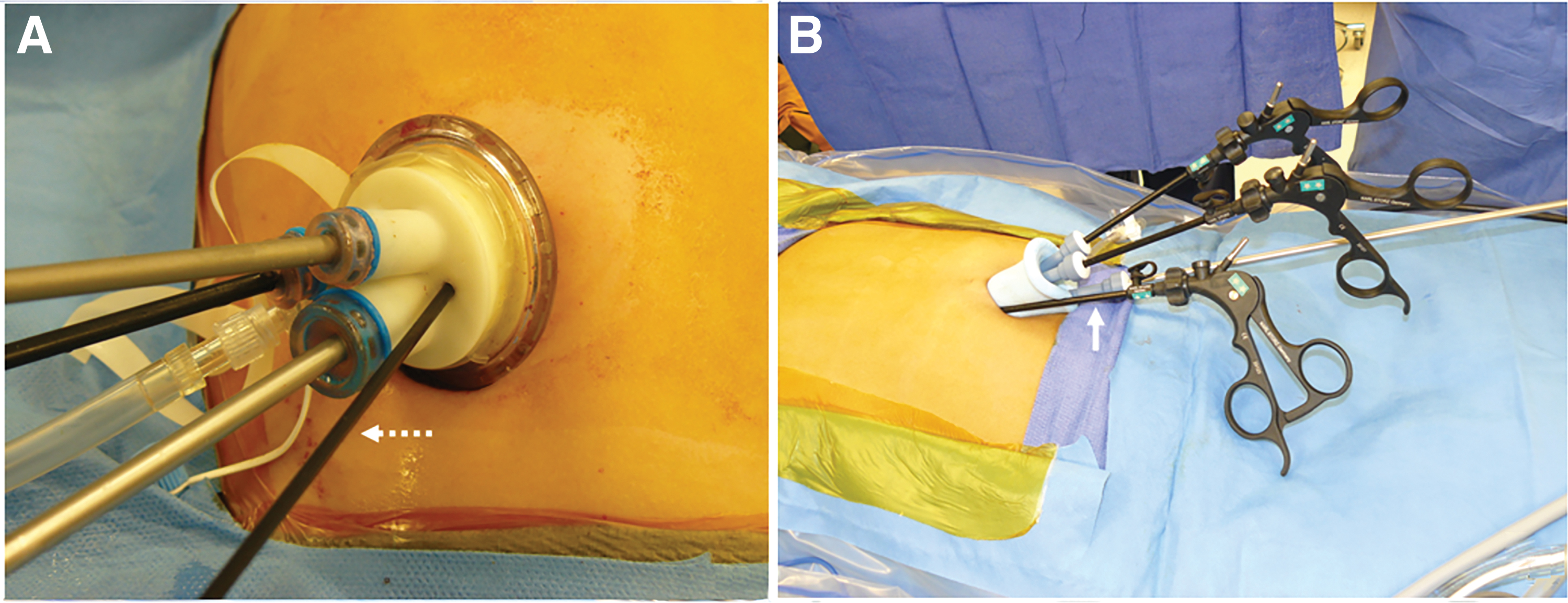
In the United States, a premanufactured port is often utilized for a single-site umbilical laparoscopic cholecystectomy. The two main devices used are the TriPort (Olympus America, Center Valley, PA) on the left and the SILS Port (Medtronic, Minneapolis, MN) seen on the right. The TriPort
Postoperative Care
Most children can be discharged within 24 hours. They may return to a regular diet right away. There is no need for postoperative antibiotics. Pain can typically be controlled with non-narcotic oral medications such as acetaminophen and ibuprofen alone; however, oxycodone is sometimes utilized in the first 48 hours for uncontrolled pain. We typically do not limit activity or place lifting restrictions postoperatively.
Results
For children with symptomatic cholelithiasis, symptoms usually resolve after laparoscopic cholecystectomy. When performed for biliary dyskinesia, resolution or improvement of symptoms after cholecystectomy has been reported in 44%–97%.4,19,20 Infectious complications are rare and removing any spilled stones can reduce the risk of infection.
The most feared complication of laparoscopic cholecystectomy is injury to the CBD. This complication is rare particularly as experience with laparoscopy has increased. However, although the rate of ductal injury with this procedure has decreased, about 1 per 1000 adults undergoing a laparoscopic cholecystectomy requires ductal reconstruction. 21 Complications in children will likely remain less than adults given the high percentage of adults presenting with severe inflammation of the gallbladder making it more difficult to discern dissection planes. Although very few pediatric patients present with such severe inflammation, any surgeon performing a laparoscopic cholecystectomy should be cognizant of the potential complications and know how to manage them.
If a ductal injury occurs during the operation, it is recommended to convert to an open procedure to repair the injury with a low threshold to perform a hepaticojejunostomy. 22 If an injury is identified after the operation, as in the case of some obstructive ductal injuries and delayed strictures, the injury can be temporized with percutaneous transhepatic drainage of the ductal system after which the patient should be referred to a center with experience reconstructing these injuries. In this setting, Roux-en-Y hepaticojejunostomy has a 98% success rate. 23
A bile leak after laparoscopic cholecystectomy often comes from the cystic duct stump or from the ducts of Luschka within the gallbladder fossa. A pressure gradient of ∼10 mmHg exists within the biliary system due to the sphincter of Oddi. Therefore, the majority of bile leaks will resolve with sphincterotomy and stent placement, which can be performed through endoscopic retrograde cholangiopancreatography.22–24
Complications after cholecystectomy in children most commonly occur in the setting of hemolytic disease and are related to the underlying disease. In a dated report of 364 cases from a national sickle cell disease study group, the complication rate was 39%. 25 These include sickle cell events in 19%, intraoperative or recovery room problems in 11%, transfusion complications in 10%, postoperative surgical events in 4%, and death in 1%. 25 Up to 20% of sickle cell patients undergoing abdominal surgery can get acute chest syndrome and the surgical approach does not seem to affect the incidence of this complication. For these patients, meticulous attention to perioperative management, following transfusion guidelines, and good pulmonary care can help reduce the incidence of complications.
Discussion
Regardless of the operative approach, laparoscopic cholecystectomy is safe and effective in children and has become a common procedure in pediatric surgery. After initial case series were reported, the single-site approach garnered a lot enthusiasm. The largest prospective randomized trial in children randomized 60 children to either a single incision or the standard 4-port laparoscopic cholecystectomy. 26 The results showed that the single-incision approach had longer mean operative times compared with the standard 4-port technique as well as greater surgical difficulty (Table 1). In addition, patients in the single-incision group had more pain requiring higher doses of postoperative analgesia and accrued more significant hospital charges. Since the main advantage purported by many surgeons was superior cosmesis, the patients from this trial were followed in the short and long term with a validated scar assessment tool. The results showed a marginal advantage in early follow-up (Fig. 3), and also a very small effect size at a minimum 18 months after the operation. 27 Multiple randomized trials and comparative series have been performed in adults confirming these findings of longer operative times with single incision and little other differences. In a Cochrane review of 9 randomized adult trials with 427 single-site patients compared with 428 four-port patients, those undergoing the single-site approach had longer operating times with low-quality evidence to support any benefit, whereas the safety profile remains unproven. 28 Interestingly, this meta-analysis also concluded no cosmetic benefit. Although the current data suggest no advantages for single-site laparoscopic cholecystectomy, the takeaway message is that any advantage potentially gained from the single-site approach is small if it exists and the surgeon should not labor through a difficult operation. If at any point there is technical difficulty with the single-site approach, additional instruments should be placed as there is little to no downside. Regardless of the technique used to remove the gallbladder laparoscopically, in the absence of other problems, these patients can safely be discharged after the operation with a low rate of readmission.29–31

These 2 patients both underwent a laparoscopic cholecystectomy.
Operative Data Comparing Patients Undergoing Laparoscopic Cholecystectomy Through a Single-Incision Approach Versus a 4-Port Technique
From: Ostlie et al. 26
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.