
Abstract
Background:
Intraoperative findings during laparoscopic cholecystectomy (LC) are highly unpredictable and operative difficulty varies from straightforward to very challenging procedures. Several studies described predictors of technical difficulty and graded intraoperative findings of LC; however, none specifically reported on the effect of such factors on clinical outcomes. This study aims to evaluate if preoperative characteristics of patients undergoing LC predict how likely they are to fail to be day case (DC).
Methods:
Data of patients who underwent LC from 2015 to 2017 were retrospectively analyzed. Subjects were divided into four groups, according to Nassar's classification of intraoperative difficulty. Differences in frequencies were evaluated with the the chi square and post hoc chi square tests or Fisher's exact test; logistic regression analysis was used to identify independent variables that were predictors of intraoperative complexity, postoperative morbidity, and length of stay.
Results:
A total of 1043 patient were included with male to female ratio of 1:2.5. Older age, male gender, and comorbidities were associated with higher Nassar score (P < .0001); Nassar 3 and 4 were predictors of postoperative morbidity (P < .05). The DC rate was 74.2% (Nassar 1), 75.8% (Nassar 2), 61.1% (Nassar 3), and 26.2% (Nassar 4), respectively. Age ≥60 years (P < .05), body mass index ≥35 (P < .05), and Nassar 3 and 4 (P < .05) were predictors of increased conversion from DC to inpatient (IP) stay.
Conclusion:
LC can be safely performed on a DC basis even when surgery is technically challenging. The need of IP stay can be predicted in comorbid old adult men with anticipated higher Nassar's score.
Introduction
Laparoscopic cholecystectomy (LC) is a common surgical procedure, and it is estimated that in the United Kingdom nearly 70,000 cases are performed every year. 1 Surgical complexity ranges from straightforward to a very challenging operation and intraoperative features impact on clinical outcomes. 2 Although uncomplicated procedures can be safely performed as day case (DC) with excellent results,3–5 complex surgery is associated with higher postoperative morbidity rates and prolonged hospital stay. 2
In the published literature, there are different classifications of the degree of technical difficulty of LC.6,7 These tools allow for a homogeneous description of intraoperative findings and are proven to correlate with postoperative outcomes. 2 They, however, rely on procedural complexity only. To our knowledge, there are no data on how patients' preoperative features impact on technical aspects of LC and clinical outcomes.
Aim of this study is to evaluate if preoperative characteristics of patients undergoing LC predict how likely they are to fail to be DC.
Methods
Ethics
Local institutional review board approval was obtained for the study. All data were fully anonymized at the time of collection and, therefore, individual informed consent was not required.
Context
The Royal Devon and Exeter NHS Foundation Trust, United Kingdom, is a district general and teaching hospital. At our institution, LC is performed with a standard four-trocar technique. Unless there is compelling clinical or social need, surgery is routinely scheduled on a DC basis. However, during technically challenging procedures, when there is clinical concern of an increased risk of postoperative fluid collection or bile leak, an abdominal drain is left in the Morrison pouch; in such cases, patients are kept in hospital for observation.
Patients
All the patients who underwent LC from 2015 to 2017 were considered for the study. Cases were identified from the hospital information center database. Exclusion criteria were planned open surgery, common bile duct exploration during LC, and patients with incomplete clinical records.
Data collection
Subjects were divided into four groups, according to the Nassar's classification of intraoperative difficulty of LC. 7 Patients' demographics, body mass index (BMI), comorbidities, American Society of Anesthesiologists (ASA) score, postoperative mortality, complications, length of stay, and readmission rate were retrospectively evaluated.
Nassar's scores were calculated based on the operative notes and were checked separately by 2 different researchers, to ensure a higher degree of objectivity. Postoperative mortality, morbidity, and readmissions were considered when occurring within 30 days after LC. Complications were reported using the Clavien–Dindo classification. 8
Data analysis
Statistical analysis was conducted using R version 3.6.3 (R Foundation for Statistical computing, Austria). Means were compared using the ANOVA and post hoc ANOVA tests, medians were compared using the Kruskall–Wallis test. Pairwise comparisons and categorical variables were evaluated using the chi square and post hoc chi square tests or Fisher's exact test. Multiple regression analysis was applied to test if patients' characteristics were predictors of intraoperative complexity based on the Nassar's classification, postoperative morbidity, and length of stay, respectively; results were given as odds ratio (OR) and confidence interval (CI). Statistical significance was set when P < .05.
Results
Sample characteristics
Overall, 1090 patients underwent cholecystectomy; 47 cases were excluded because of planned open surgery (2), common bile duct exploration performed at the same time of LC (16), and incomplete clinical records (29). Finally, 1043 patients were included in the study (Fig. 1).
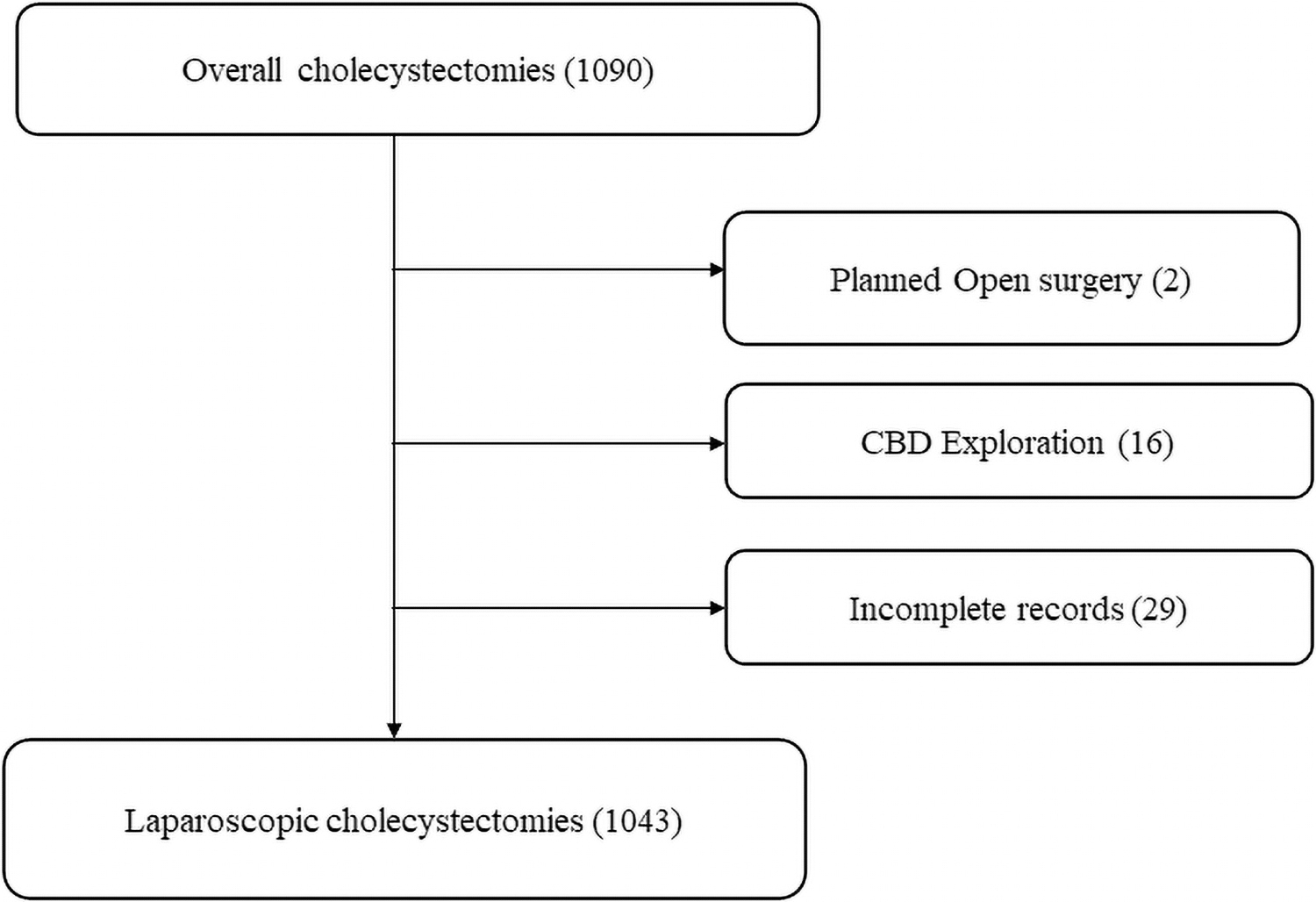
Patients' selection. CBD, common bile duct.
Patients' characteristics are described in Table 1. There were 746 (71.5%) women, 297 (28.5%) men, the female-to-male ratio was 2.5:1. Mean age was 54.4 (range 15–94). Subjects in Nassar 3 and 4 groups were older and male gender was more represented in Nassar 4 (P < .0001). Data on BMI were available in 367 (35.2%) patients and there was no difference among groups (Table 1). ASA scores were higher in Nassar 4 (P < .05).
Patients' Characteristics and Perioperative Data
All bold values are significant.
ANOVA.
Chi square/Fisher's exact test.
ASA, American Society of Anesthesiologists; BMI, body mass index; DCS, day-case schedule; IPS, inpatient schedule; LC, laparoscopic cholecystectomy; NS, not significant.
Surgery was scheduled as DC in 848 (81.3%) cases, whereas inpatient (IP) admission was planned in 195 (18.7%); patients in Nassar 3 and 4 groups had a higher proportion of planned IP schedules (P < .05).
Perioperative data
LC was performed on elective basis in 970 (93%) cases, as an emergency in 73. The proportion of emergency surgery was higher in Nassar 3 (11.7%) and 4 (8.8%, P < .05).
Conversion to open was necessary in 1 patient (0.09%) who belonged to Nassar 4 group.
An abdominal drain was placed at the end of surgery in 122 patients and the distribution among groups was Nassar 1 (16), Nassar 2 (15), Nassar 3 (57), and Nassar 4 (34). The higher proportion of abdominal drains in Nassar 3 and 4 was statistically significant (P < .0001). Predictors of higher operative difficulty (Nassar 3 and 4 scores) were age >60 years, male gender, and urgent LC (Table 2).
Predictors of Higher Operative Difficulty
All bold values are significant.
CI, confidence interval; LC, laparoscopic cholecystectomy; NS, Not significant.
Postoperative outcomes
Mortality and morbidity
No postoperative mortality occurred. As described in Table 3, postoperative complications developed in 28 (2.7%) patients and Nassar 4 group had the highest incidence (10.3%, P < .0001). The severity of complications did not differ among groups. A bile leak occurred in 9 (0.9%) cases, 8 of which were in Nassar 3 and 4 groups. Causes of bile leak were common hepatic duct injury (2) and misplacement of the surgical clips on the cystic duct stump (7), respectively. In none of the cases a leak was detected intraoperatively; an abdominal drain was placed in 6 patients who remained in hospital, and 3 went home on the same day of surgery. In 8 cases, the leak had a delayed presentation, as the patients were discharged home; one of those who remained in hospital developed an early leak that was treated with laparoscopic suturing of bile duct injury. The remaining patients were treated with laparoscopic washout (4), endoscopic retrograde cholangiopancreatography and biliary stent (3), and biliary reconstruction (1), respectively.
Patients' Outcomes
All bold values are significant.
CBD, common bile duct; DC, day-case stay; IP, inpatient stay; IV, intravenous; LOS, length of stay; NS, not significant.
Predictors of postoperative complications were Nassar 3 (OR 5.1, 95% CI 1.66–22.1, P < .05) and Nassar 4 (OR 12.2, 95% CI 3.36–57.8, P < .05) scores.
Hospital stay
As shown in Table 3, median hospital stay was 0 days (range 0–23 days) and patients in Nassar 3 and 4 groups stayed longer (P < .0001). Among those who were listed as DC, 587 (69.2%) went home on the day of surgery; the DC rate was lower in Nassar 4 (P < .0001). The remaining 261 stayed in hospital because of challenging surgery (93), anesthetic reasons (28), medical conditions (28), and social circumstances (112). Within this group, 126 (48.3%) were >60 years old; the BMI was recorded in 94 cases and in 27 (28.7%) was ≥35.
Age ≥60 years, BMI ≥35, Nassar 3 and 4 scores were independent predictors of conversion from DC to IP stay (Table 4).
Predictors of Conversion From Day Case to Inpatient Stay
All bold values are significant for <0.5 while 0.9 is not significant.
BMI, body mass index; CI, confidence interval; DC, day case; ERCP, endoscopic retrograde cholangiopancreatography; IP, inpatient; LC, laparoscopic cholecystectomy; NS, not significant.
Readmissions
Overall, 56 (5.4%) patients were readmitted to hospital and the rate did not differ among groups (Table 3). Twenty-eight underwent DC surgery (4.8%), and 28 were IP (6.1%). Causes of readmission are described in Table 3.
Discussion
Clinical outcomes of LC depend on several factors, including the technical difficulty of surgery. In clinical practice, anticipating whether LC will be straightforward or challenging is not always possible; in fact, unexpected degrees of complexity are often encountered. Nevertheless, the prediction of how likely surgery will be performed on a DC basis would be helpful when counseling patients in the preoperative setting, as that would aid in delivering clearer information on expectations and outcomes; in addition, that would allow a more appropriate surgical scheduling, which in turn would lead to a better planning and more efficient utilization of hospital resources. 1 Some authors had validated a preoperative risk score that uses patients' variables to predict difficult surgery 9 ; despite its accuracy, the calculation does not assess the impact on clinical outcomes.
In this study, few preoperative patients' characteristics were considered to predict both the technical difficulty of LC and postoperative outcomes. Complex procedures (Nassar 3 and 4) were reported in 34.4% of cases. Age ≥60 years, male gender, and urgent surgery were predictors of challenging surgery. Authors10,11 had hypothesized that old adults with gallstones may suffer from several episodes of acute cholecystitis and over time, the prolonged trauma of gallstones to the gallbladder mucosa stimulates the onset of chronic inflammation. Both conditions would eventually lead to the formation of local fibrosis, which makes surgery more difficult. 12 Male gender is another recognized predictor of challenging LC.13,14
Conversion to open was necessary in one Nassar 4 patient with hostile anatomy of the Calot's triangle caused by dense fibrosis. 15 As expected, the rate of postoperative complications was higher in Nassar 4 patients. Although the Clavien–Dindo score did not differ among groups, 8 out of 9 bile leaks occurred in Nassar 3 and 4 subjects. Interestingly, in those patients the complication had a delayed onset; 6 of them were even kept in hospital with an abdominal drain in place. Complex surgery was predictor of postoperative morbidity; it is acknowledged that the presence of dense fibrosis around the gallbladder and in the Calot's triangle is associated with a higher risk of iatrogenic biliary or vascular injuries.16,17 In this series, the DC rate was 69.2%; one third of patients who were initially scheduled as DC remained in hospital after surgery and the rate of conversion from DC to IP was higher in Nassar 4. Of note, 43% of them were kept in hospital for nonclinical reasons; the authors argue that perhaps this could be in part prevented by a better preoperative assessment of patients' personal circumstances. Age ≥60 years, high BMI, and higher Nassar scores were predictors of increased conversion from DC to IP stay. In the literature, it is recognized that high-risk patients and those whose surgery is challenging are deemed as not suitable for DC LC.1,18 Perhaps ensuring that patients over 60 are performed as early in the day as possible may potentially increase the chances of same-day discharge. The readmission rate did not differ among groups and was not associated to the surgical schedule either.
Conclusion
The retrospective nature of this study prevents from drawing definitive inferences; within these limitations, the authors conclude that LC can be performed on a DC basis even when surgery is technically challenging. The need of IP stay can be predicted in high-BMI old adults with anticipated complex surgery.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by A.O., I.N., M.R., S.T., and D.D.M. The first draft of the article was written by A.O. and D.D.M., and all authors commented on previous versions of the article. Conceptualization, methodology, and writing original draft preparation by A.O. and D.D.M. Formal analysis and investigation by A.O., I.N., and D.D.M. Writing review and editing by A.O., D.D.M., and A.M. Supervision by A.M., A.R.-S., and S.W. All authors read and approved the final article.
Ethics Approval and Consent to Participate
The study had been registered and approved by the Royal Devon and Exeter NHS Foundation Trust Governance Board—reference number 20-4863.
Consent to Participate
Participants' consent to the study was not obtained, as no identifying details were used.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.