
Abstract
Background:
Congenital diaphragmatic hernia (CDH) is a relatively common congenital anomaly, typically requiring repair in the neonatal period. Approaches to surgical repair of a CDH are varied. A small defect may be repaired primarily while a large defect often requires a patch repair. Minimally invasive and open techniques have been reported to have varying benefits and outcomes.
Materials and Methods:
The authors describe their technique of CDH repair and present a review of the literature.
Results:
In a stabilized neonate with a small-to-moderate CDH defect, a thoracoscopic primary repair with biological mesh underlay (or a patch repair if needed to reduce tension) represents our approach of choice to treat this pathology. However, attention to specific technical details is required to minimize incidence of recurrence.
Conclusions:
The data favor a minimally invasive approach to CDH repair in the appropriate patients.
Introduction
Congenital diaphragmatic hernia (CDH) is a relatively common congenital anomaly, occurring in ∼1 of 2000–5000 births. A Bochdalek (posterolateral) hernia is the most common CDH encountered in the neonatal period. In severe cases, CDH can be accompanied by physiological changes related to hypoplastic lung and pulmonary hypertension, requiring extracorporeal membrane oxygenation (ECMO) and specialized care to improve survival. 1 Ultimately, with survival, the diaphragmatic hernia defect will require repair in the neonatal period. Approaches to surgical repair of a CDH are varied including: open or minimally invasive technique, repair through the chest or abdomen, primary repair or additional patch repair, or reinforcement. Minimally invasive approach has been reported to have benefits of decreased small bowel obstruction and no ventral hernias, but a higher recurrence rate. In a stabilized neonate with a small-to-moderate CDH defect, a thoracoscopic primary repair with biological mesh underlay (or a patch repair if needed to reduce tension) represents our approach of choice to treat this pathology. However, attention to specific technical details is required to minimize incidence of recurrence. This article is focused on the operative technique of thoracoscopic neonatal CDH repair.
Preoperative considerations
Patient selection and timing of the operation are very important as not all newborns are candidates for minimally invasive CDH repair. Unless the baby is going to be repaired on ECMO, the basic principle for both open and minimally invasive surgical (MIS) repairs is that the baby needs to be stable enough to tolerate the operation. Preoperative evaluation with an echocardiogram can reveal hemodynamically significant cardiac defects and assess the severity of pulmonary hypertension. These data may influence timing and method of repair. Ideally, repair is delayed until the pulmonary artery pressures are less than systemic pressures. 2 Ultimately, a baby will tolerate both an open and MIS repair if they are on lower ventilator settings and do not require significant levels of medications to support their blood pressure. Along these lines, the baby should be stable enough to be transported to the operating room. If not, support with ECMO or an open repair at bedside in the neonatal intensive care unit may need to be considered. Timing of the operation should be based on these hemodynamic and respiratory factors. Critical care management of pulmonary hypertension, hemodynamic, and respiratory support are vitally important and are discussed elsewhere.1,3
Early in a surgeon's experience, they may want to choose the MIS approach for larger newborns, but ultimately, the operation is not much more difficult in a smaller baby as the hypoplastic lung leaves significant space in the chest and great visualization in all sizes of babies.
Some institutions prefer to use a paralytic for 12–24 hours before the planned operation to decrease the bowel gas and make reduction easier. This certainly does reduce the bowel gas but is probably unnecessary if you have a functioning orogastric tube on suction.
Perioperative antibiotics can be considered, given the possibility of using a mesh for the repair. A first-generation cephalosporin is a reasonable choice if there is no known colonization with drug-resistant bacteria.
An arterial line and Foley catheter should be considered for a sicker baby but may not be necessary for a very stable neonate if your repair is consistently well under 3 hours in duration. This operation most commonly has minimal blood loss, but a starting hematocrit of >30% makes any operation better tolerated in a neonate.
For anesthetic considerations, no single-lung ventilation is required. The babies tend to have a hypoplastic lung, giving plenty of space in the chest for visualization for the operation. It is advantageous to use an initial paralytic until the bowel has been reduced from the chest into the abdomen. Carbon dioxide (CO2) insufflation in the chest is used to assist in this process as well. Once the first suture has been placed in the diaphragm, the paralytic is allowed to wear off and the insufflation is decreased to a minimum.
Positioning
For thoracoscopic CDH repair, the patient should be positioned in the decubitus position with the side of the defect up and with an axillary roll and appropriate padding. Of great importance, padding is used to elevate the body and allow the head to rest slightly lower with the arm extended in the direction of the endotracheal tube (Fig. 1). Without this adjustment, the head and arm will impair movement of the camera and instruments throughout the operation.
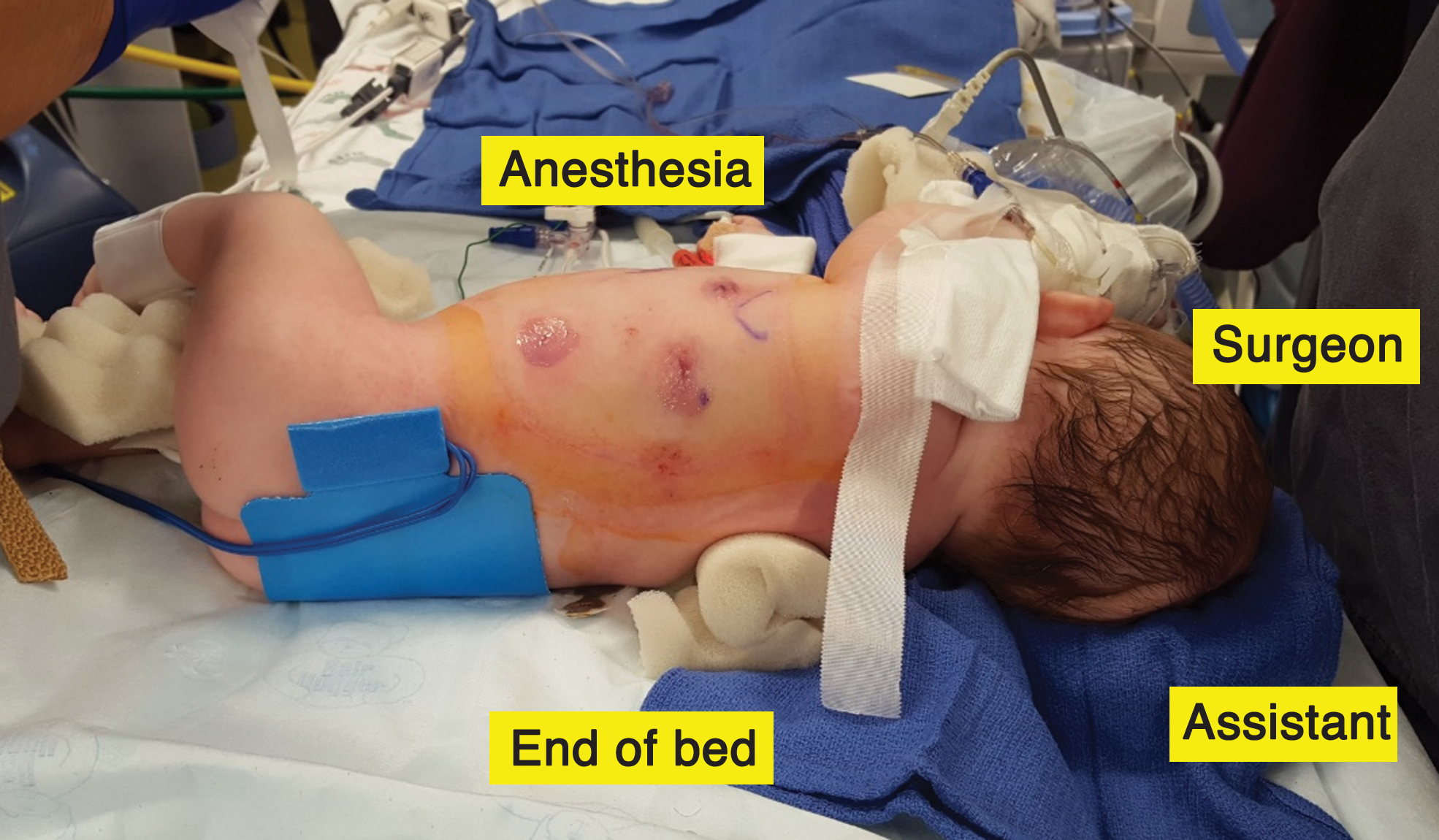
The baby is in cross-table lateral position at the end of the bed with the face directed toward anesthesia. Padding is used to elevate the body and allow the head to rest slightly lower with the arm extended in the direction of the endotracheal tube. Color images are available online.
The authors prefer to have the baby positioned cross-table at the end of the bed. The face is directed toward anesthesia at the head of the bed. The surgeon is at the baby's head, monitor at the feet, and assistant at the end of the bed (Fig. 1). This provides the most ergonomic position for surgeon and will maximize ability to complete the operation thoracoscopically. If it is necessary to convert to open (usually for a subcostal incision), this position can be maintained or the trocar sites can be closed and the baby repositioned. The baby is secured to the bed and sterilely prepped to include the neck, chest, and abdomen.
Equipment
Three or 5 mm laparoscopic trocars and equipment are used. Three trocars are used with the camera in the middle, anterior to the scapula in the mid-axillary line. The two working ports are placed slightly inferiorly on either side of the camera to allow for triangulation (Fig. 2).
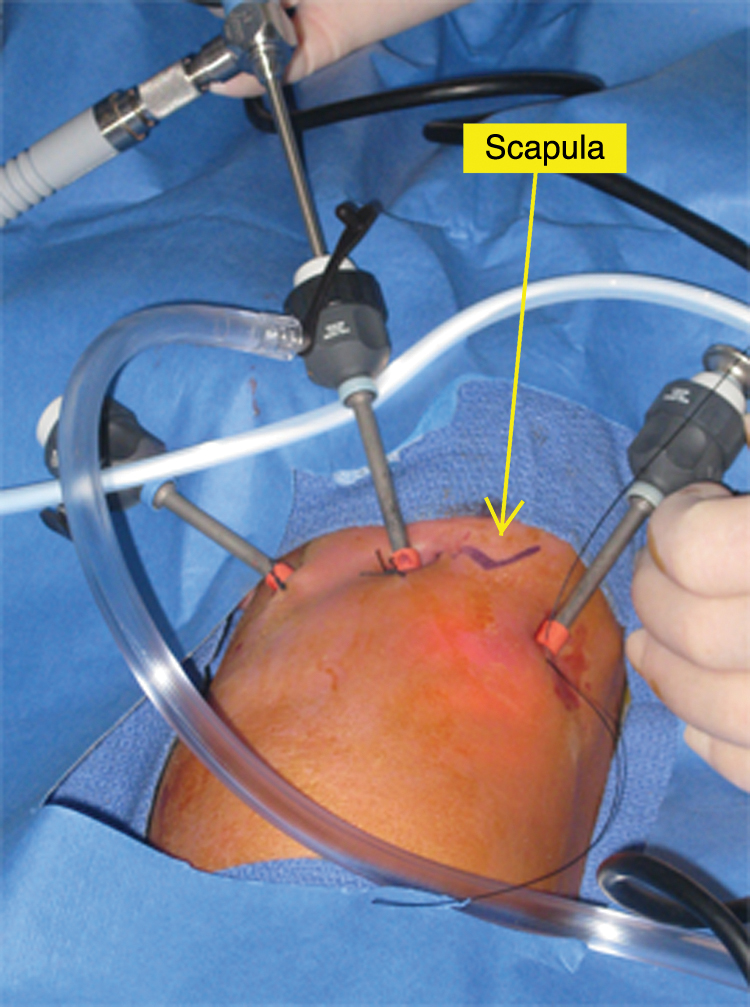
Three trocars are used with the camera in the middle, anterior to the scapula in the mid-axillary line. Two working ports are placed slightly inferiorly on either side of the camera to allow for triangulation. Color images are available online.
It is preferable to use the 18 cm long instruments as this shorter length provides better control in a small operating space. A 30° scope seems to provide better angles of visualization than a 0°. We prefer 2-0 or 3-0 nonabsorbable suture. If the needle is skied (partially flattened), it will pass easily through a 5 mm trocar. Alternatively, 3 mm trocars can be used and the needle passed directly through the chest wall, but retrieval is sometimes challenging and may slow operative time.
A laparoscopic suture passer (or trocar site closure device) is helpful to increase the speed of performing the extracorporeal–intracorporeal lateral pericostal stitches. Mesh should be available in case it is needed. Laparotomy equipment should be available in case conversion to open is warranted.
Technique
Step 1: Reduction of hernia contents
It is important that the baby is completely relaxed during this part of the procedure, as Valsalva or coughing can result in the bowel being thrust back into the chest cavity. The chest is insufflated with CO2 to 3–4 mmHg. Blunt atraumatic graspers are used to gently reduce the bowel and other abdominal contents toward the posterolateral defect (which is toward the upper aspect of the visual field when the baby is in the decubitus position). On the left side, if the left lobe of the liver is in the chest its attachments often have to be divided to mobilize it into the abdomen. Care must be taken to not injure the spleen. The spleen is replaced into the abdomen last and can be used as a “cap” to help hold the rest of the viscera in the abdomen. On the right side, the liver can serve as a “cap.” If there is a hernia sac, it can be used to help reduce the contents into the abdomen, but the hernia sac will need to be partially separated off the leaflets of the diaphragm enough to define the edge of the defect and allow for precise placement of sutures.
Step 2: Assess the size of the defect
The initial amount of bowel in the chest cavity is not reflective of the size of the defect in the diaphragm, as a lot of bowel can protrude through a very small defect. Once the contents are reduced into the abdomen, the size of the defect is assessed. To fully evaluate this, a hernia sac (if there is one) may need to be separated off the leaflets of the diaphragm. The leaflets of the diaphragm may also need to be unrolled with the assistance of hook electrocautery.
At this point, the decision is made of whether the defect is small enough to perform a primary repair or whether permanent mesh will be needed to complete a tension-free repair. If there is agenesis of the diaphragm or a mesh is required and the surgeon does not have experience suturing a larger mesh intracorporeally, consideration should be made to convert to open.
Step 3: Cauterize edges of the diaphragm
Probably the two most important aspects of minimizing recurrences in a CDH repair are creating inflammation on the edges of the diaphragm to enhance the healing process and suture placement to achieve a tension-free repair. If either aspect is missing, recurrence rates are likely to rise.
The process of creating inflammation on the edges of the diaphragm is similar to removing the hernia sac for an umbilical hernia repair or cauterizing the internal ring (lateral to vas and vessels) in a laparoscopic inguinal hernia repair. The concept is that sticky edges heal well together, whereas peritonealized smooth surfaces do not stick or heal to each other, thus relying more heavily on the sutures rather than the body's healing ability.
To achieve this, the hook electrocautery is simply moved along the entire circumference of the CDH defect, creating a little burn to cause inflammation (Fig. 3). Care is taken to not injure adjacent structures.
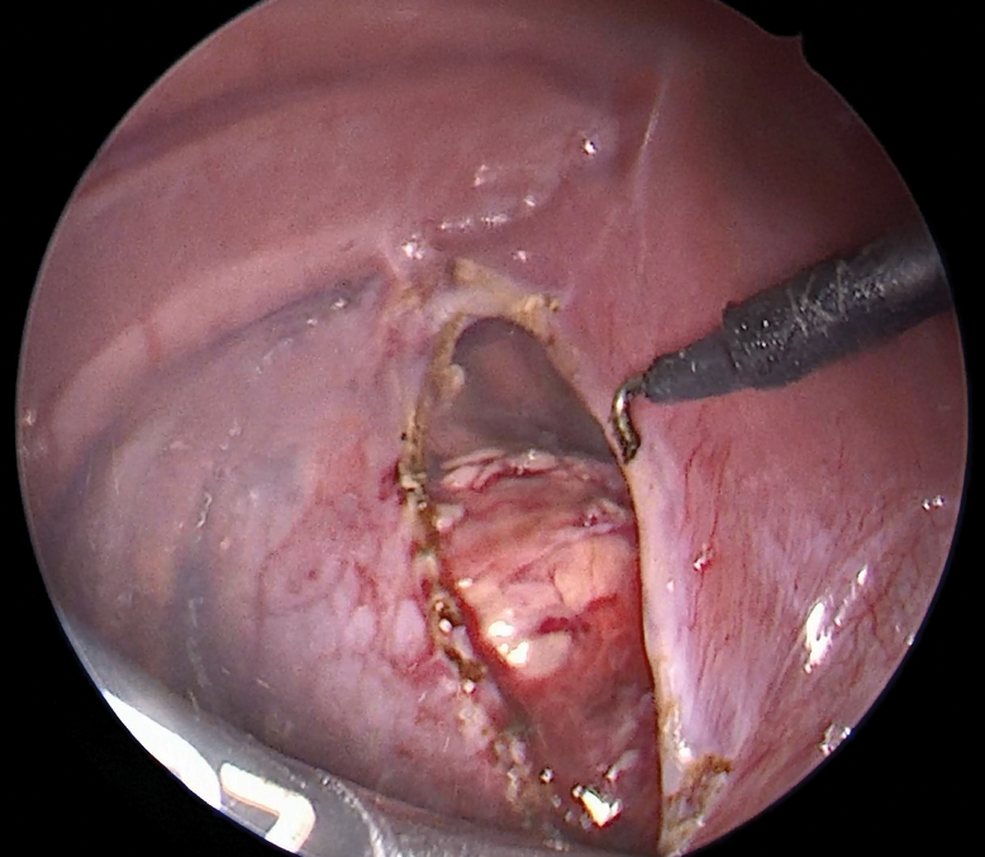
Electrocautery is used to create inflammation along the edges of the diaphragm to enhance the healing process. Color images are available online.
Step 4 (optional): Biologic mesh underlay reinforcement (routinely used by authors given data suggesting reduced recurrences)
We recently published data demonstrating a decreased recurrence rate in both open and minimally invasive CDH repairs when a biologic mesh is placed on the abdominal side as reinforcement of a primary repair. 4 Given these data, the authors routinely use biologic mesh underlay reinforcement in both primary and mesh repairs.
To place a biologic mesh underlay from the thoracic cavity, the distance between the tips of a laparoscopic grasper is used to measure the size of the defect (Fig. 4). The biologic mesh is cut 1–2 cm larger than the shape of the defect in each direction to allow for overlap of the repair. (Consider adding an extra couple centimeters of length to the mesh in the medial to lateral direction as it is easy to bunch up the mesh and end up with too little laterally.) An absorbable suture is placed on the intended medial corner of the mesh to orient it. The mesh is rolled lengthwise to make it as thin as possible. It is always easier to pull a mesh into the chest, rather than push it in. To facilitate this, we insert a grasper through one working port and out the working port directly opposite it (Fig. 4). We then remove the second working port, leaving the grasper protruding out of the chest cavity. The corner of the rolled mesh is grasped and pulled into the chest. The second working port is replaced. The mesh is unrolled in the thoracic cavity and oriented correctly.

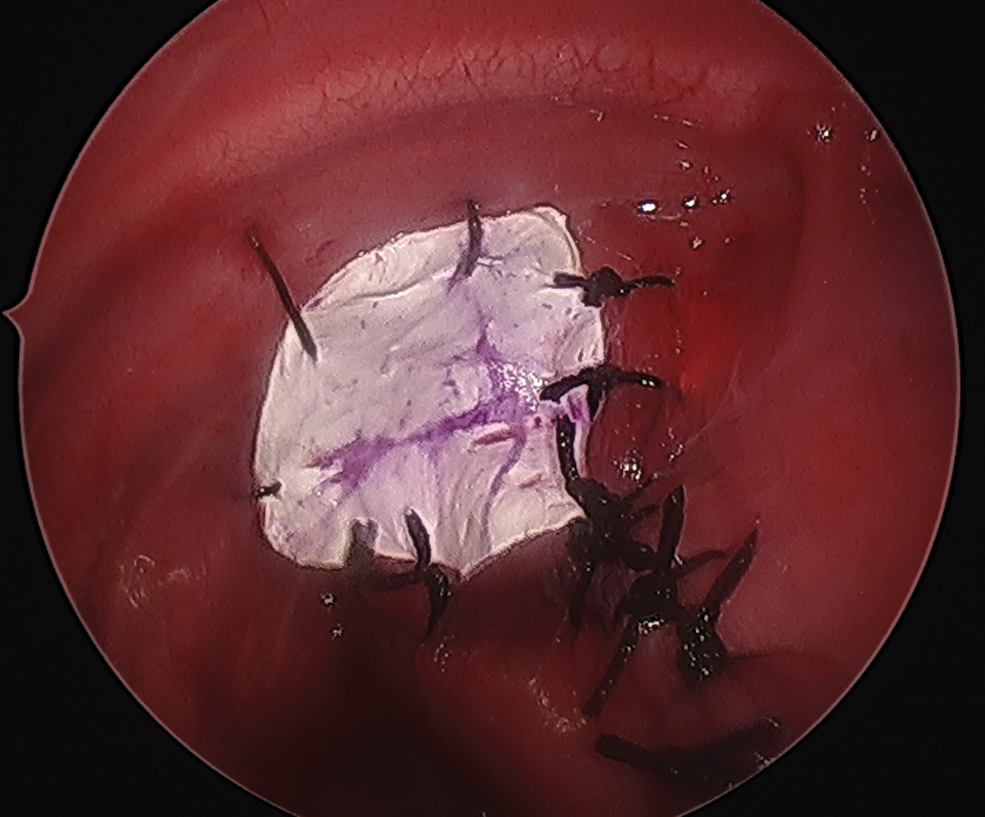
The first suture is placed to repair the CDH about 1 cm from the medial edge. A laparoscopic needle drive is inserted through the medial corner under this suture, grasping the medial suture on the mesh, and pulling the mesh through under the defect. The mesh is secured at this corner with a suture closing the medial corner. The mesh is splayed out under the defect on the abdominal side. Sutures closing the defect are placed through the anterior leaflet, through the middle of the mesh, through the posterior leaflet, and then tied down. Care is taken to not advance too much on the biologic mesh to leave plenty of overlap on the lateral wall. The end result is that the biologic mesh underlay cannot be visualized in the chest but is spread out on the abdominal side secured in the middle of the mesh and overlapping the suture line by a couple centimeters on each side (Fig. 5).

The medial edge of the defect is partially closed. The underlay biomesh is unrolled, pulled underneath the defect, and secured at the medial corner. The remaining mesh is secured with sutures through the middle of the mesh during CDH closure, resulting in the biologic mesh spread out on the abdominal side overlapping the suture line by a couple centimeters in each direction. CDH, congenital diaphragmatic hernia. Color images are available online.
The authors also consider biologic mesh underlay for a larger patch repairs, resulting in a biologic mesh underlay reinforcement and a permanent patch inlay repair (Step 7).
Step 5: Primary defect closure (only if no tension)
The defect is closed using interrupted 2-0 or 3-0 nonabsorbable sutures to approximate the anterior and posterior diaphragm leaflets. The authors prefer to close the diaphragmatic defect from medial to lateral. The medial corner of the defect has the least tension, making placement of the first few sutures easier. Each medial suture then progressively takes the tension off the next more lateral edge, making placing the subsequent sutures easier. We also like this approach because it allows us to really assess as we approach the lateral aspect of the repair whether there will be any tension on it at the lateral wall. If there is no lateral diaphragmatic muscle or there appears to be increasing tension laterally, the decision needs to be made to place a pericostal suture (Step 6) or place a small piece of mesh laterally to maintain a tension-free repair (Step 7).
There are others who prefer to place a lateral pericostal suture at the very beginning to take the tension off of the lateral edge. This is a lateral to medial approach to the repair. 5 Either approach is reasonable as long as a tension-free repair can be achieved.
Step 6: Lateral pericostal suture placement
A pericostal suture is an extracorporeal–intracorporeal stitch that secures the lateral leaflets of the diaphragm (or mesh) around a rib instead of just to the weak inner chest wall muscle fibers. 6 In our approach, both tails of the suture must start and end through the same skin incision to be tied extracorporeally with the knot buried in the subcutaneous tissue.
It is common for the majority of CDH babies to be missing a segment of the diaphragm against the most posterolateral rib surface. If this is the case, then a pericostal stitch will provide a stronger primary repair. If a primary repair would generate tension laterally, then a mesh is necessary and a few pericostal stitches will be required to secure the mesh against the lateral costal margin (Step 7).
To place a pericostal stitch, first determine the optimal location on the chest wall between the two leaflets of the diaphragm by observing with the thoracoscopic camera while gently pushing on the outside of the chest wall or using a small finder needle. Make a 3-mm skin incision at this location. Choose a 2-0 or 3-0 nonabsorbable suture on a medium-sized taper needle. Using a combination of extracorporeal and intracorporeal needle drivers, the needle is passed extracorporeally through the 3 mm skin incision, inferior to a rib, thoracoscopically through the leaflets of the diaphragm (or mesh) and then superior to the rib ending extracorporeally. The needle is then manipulated out of the same skin incision so it can be tied extracorporeally.
If it is challenging to pass the needle back out of the chest wall, a laparoscopic suture passer (or trocar site closure device) can be passed through the incision, over the rib, grasp the suture in the thoracic cavity and withdraw it through the incision. This is an especially valuable technique if multiple pericostal sutures are required to secure a mesh to the lateral chest wall, as it can greatly increase the speed of placing pericostal sutures.
Step 7: Patch placement (if necessary to avoid tension on the repair)
The goal of the CDH repair is to have a tension-free repair to decrease the chance of a recurrence. If the defect is too large and diaphragmatic leaflets too small, this will not be possible without placement of a patch. We prefer to use a composite patch with a biologic overlapping underlay on the abdominal side and polytetrafluroethylene (PTFE) inlay on the thoracic side. If there is agenesis of the diaphragm, it is probably good judgment to convert to an open subcostal incision for the repair. If reasonable anterior and posterior leaflets can be identified, it is frequently possible to start closing the medial aspect of the defect for several stitches before encountering any tension on the repair. Once the tensionless medial aspect of the repair is complete, measure the remaining defect size (see Step 4).
For the biologic underlay, the mesh is cut 1–2 cm larger than the shape of the defect in each direction to allow for overlap of the repair. As described in Step 4, it is inserted and spread out on the abdominal side under the defect. It can be tacked in place with a few sutures to the underneath side of the diaphragm leaflets (or lateral wall) leaving about 1 cm overlap. It is not a strength layer but is simply secured so that it does not move and allows tissue ingrowth from the periphery.
For the permanent inlay, the PTFE patch is cut to the size of the defect and marked with a pen to orient it. It is inserted into the thoracic cavity as described (Step 4), unrolled, and oriented correctly. Interrupted sutures are then placed working from medial to lateral along both diaphragm leaflets, securing the edge of the mesh to the edge of the diaphragm as an inlay mesh. At the lateral edge when there are no longer diaphragm leaflets, several pericostal sutures will have to be placed securing the mesh directly to the chest wall with sutures going around the ribs (Step 5). The final result is a primary repair medially and a permanent mesh inlay repair laterally (Fig. 6).
For a moderate-sized defect, a primary repair is performed medially and a permanent mesh inlay repair laterally. The authors typically place a biomesh underlay on the abdominal side as well for reinforcement. Color images are available online.
Step 8: Chest tube placement versus evacuation
There is typically an obligate pneumothorax, given the hypoplastic lung. This will frequently be replaced by a hydrothorax over time if the lung cannot expand to fill the space. The goal is not to evacuate the pneumothorax or hydrothorax, but to maintain the mediastinum in a neutral position. A chest tube can be placed at the end of the procedure through a trocar site. Alternatively, the chest can be evacuated with a suction device when closing the trocar sites and aspirate air out of the chest with a needle postoperatively if necessary. Given data that there is no evidence that chest tube placement increases risk of patch infections, it is a reasonable option. 7
Postoperative care
Critical care management is essential for CDH babies with severe hypoplastic lungs and pulmonary hypertension. This management will include strategies to address possible ECMO, anticoagulation, diuresis, blood pressure support, pulmonary vasodilators, ventilation weaning, feeding protocols, gastroesophageal reflux, among other considerations1,3
If a chest tube was placed intraoperatively, it should be put on water seal (not suction) and removed when the mediastinum is neutral and there is no ongoing air leak. If a chest tube was not placed intraoperatively, chest radiographs should be monitored for need to aspirate air from the ipsilateral chest cavity if there is a hemodynamically significant mediastinal shift.
Enteric feeds are initiated (either orally or via nasogastric tube) when there is evidence of bowel function. Analgesic therapy is administered as needed during the immediate postoperative period. Perioperative antibiotics are typically stopped within 24 hours. It is ideal to remove the chest tube as soon as there is no air leak, no chyle leak, and the position of the mediastinum has stabilized.
The limiting factor on patient discharged from the hospital is likely the extent of the severity of hypoplastic lungs and pulmonary hypertension. Postoperative chest X-rays are followed at 1 month and every 3 months the first year and then transitioned to 6 months and annually. This is to evaluate for asymptomatic recurrent diaphragmatic hernias, which are greatest in the first year and at times of significant patient growth.
Results
Overall survival of CDH appears predominantly linked to underlying severity of hypoplastic lungs and pulmonary hypertension, not technique of repair. 1
Intraoperative concerns for elevated CO2 levels or acidosis during a minimally invasive CDH repair have been raised. 8 However, we have demonstrated that even in sicker patients after ECMO decannulation, average end-tidal CO2 at 15 operative minutes was 36.9 mmHg in the thoracoscopic group versus 50.7 mmHg in the open group and at 60 minutes was 34.25 mmHg versus 45.6 mmHg, respectively. 9 The thoracoscopic group never experienced significantly increased end-tidal CO2 during the operation. This may be attributed to the fact that insufflation can be decreased or turned off once the first suture is placed in the diaphragmatic repair.
Operative times trended longer in the thoracoscopic group. While this was not statistically significant (P = .11), it is consistent with the literature.8,9 Operative times likely decrease with experience and a systematic approach.10,11
Many studies have demonstrated decreased time to extubation, decreased time to feeds, decreased length of stay, and even decreased costs in the thoracoscopic group.9,11–14 Gastroesophageal reflux are common in both groups, and chyle leaks are rare in both groups.
The most clinically significant differences in outcomes between the MIS and open CDH repairs seem to hinge around recurrent diaphragmatic hernias, postoperative bowel obstructions, and ventral hernias.10,11,14 Historically, recurrence rates have been higher with MIS CDH repair. Based on CDH Study Group data, recurrence rates do seem to be decreasing in the MIS group in recent years, which may reflect adoption of better techniques. 14 In the CDH Study Group, early recurrences in the MIS group were 7.9% from 1995 to 2010. 15 More recently, their data showed that from 2007 to 2010 the MIS recurrence rate was about 6%, and in the 2010–2014 groups, the MIS and open recurrence rates were equivalent to each other. 14 We demonstrated a decrease in recurrences with biomesh underlay reinforcement. 4 Others have noted no recurrences with select techniques or when a buttress approach is used in MIS repairs.11,16 While the recurrence rate for MIS CDH still appears to be slightly higher than with open, as individuals improve their techniques, the gap seems to be closing.
More recently, the significant increased risk of postoperative bowel obstructions and ventral hernias in the open CDH repair group has come to the forefront. We demonstrated that in 144 patients over a 10-year span, there was a statistically significant increase in the incidence of bowel obstruction in patients undergoing open repair of CDH (14.3% in patients repaired open, 0% in patients repaired thoracoscopically). 17 This included patch repairs in both groups. The CDH Study Group concurred with these findings, showing an increased risk of bowel obstruction in the open repair group. 14 Bowel obstruction seems to be a clear disadvantage of the open repair, independent of mesh utilization, as this finding is consistent with the literature.11,13 Ventral hernias have also been noted to be a problem unique to the open repair group, with reports of up to 14% versus 0% in the MIS group. 11
Discussion
In care for a neonate with a CDH, attention first needs to be focused on the often challenging and life-threatening problems due to physiological changes related to hypoplastic lung and pulmonary hypertension. As the neonate stabilizes, attention turns to repair of the diaphragmatic hernia. A minimally invasive CDH repair has become a more common approach but not without concerns for higher recurrence rates. The thoracoscopic approach appears to be safe, even in select patients after ECMO decannulation. Touted benefits of the MIS CDH repair include decreased time to extubation, decreased time to feeds, decreased length of stay, and even decreased costs in the thoracoscopic group. Confounding factors may make the significance of these benefits difficult to tease out. What does appear to be clear is an increased risk of bowel obstruction with the open approach, independent of whether a patch was utilized. If a systematic approach with key technical components could be applied to the thoracoscopic neonatal CDH repair, lowering recurrence rates and decreasing operative times, then the appeal of minimizing postoperative bowel obstructions would weigh heavily in the favor of the MIS approach.
We have presented some technical tips that we believe have the potential to improve success in approaching a thoracoscopic neonatal CDH repair:
Select the right patient: select stable patients and smaller defects (reasonable in most cases to take a quick thoracoscopic look and convert to open for agenesis of the diaphragm or large defects) Position for success: cross-table lateral with body elevated will reduce interference and provide the most ergonomic position for the surgeon Cauterize edges of the diaphragm: creating inflammation on the edges of the diaphragm will enhance the healing process Primary defect closure only if no tension: with any tension, consider closing the defect from medial to lateral and add an in-lay permanent patch on the lateral aspect of the repair to avoid tension Placement of pericostal stitches when diaphragm missing laterally: extracorporeal–intracorporeal sutures are placed around a rib to better secure the repair laterally Consider routine use of underlay biomesh reinforcement: from a thoracic approach, biologic mesh is placed on the abdominal side as reinforcement with significant overlap on the underside of a primary or patch closure
Published data seem to point to a clear disadvantage of the open CDH repair approach in terms of postoperative bowel obstructions and incidence of ventral hernias. Recurrent diaphragmatic hernias after MIS CDH repair have been decreasing over the past two decades, likely due to growing experience and modification of techniques. We have proposed here a thoracoscopic neonatal CDH repair approach that may assist surgeons in achieving an expeditious and technically sound result with minimal recurrences.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors declare that they have received no financial support for this study.