
Abstract
Aim:
To compare clinical outcomes in infants and children with intestinal malrotation who were treated by laparoscopic or open Ladd's.
Methods:
PubMed, EMBASE, and Cochrane library were searched for studies comparing laparoscopy with open Ladd's for intestinal volvulus through January 5, 2021. Search terms were confined to Title/Abstract: “Intestinal Volvulus” OR “Intestinal malrotation” AND “Laparoscopy” AND “Laparotomy.” Randomized controlled trials (RCTs) and retrospective studies comparing laparoscopy with open Ladd's in neonates, infants, or children were included. Outcomes evaluated included operative time, time to full feeds, length of hospital stay, rate of conversion, reoperation, overall postoperative complications, postoperative adhesive small bowel obstruction, and postoperative volvulus. Pooled odds ratios (OR) were calculated for dichotomous variables; pooled mean differences (MDs) were measured for continuous variables.
Results:
Fourteen studies were included, comprising 444 patients who underwent laparoscopic approach and 1422 patients who underwent open procedure. Laparoscopy group had shorter operative time (MD = −14.44 minutes, 95% confidence interval [CI] = −20.79 to −8.09, P < .00001), hospital stay (MD = −4.57 days, 95% CI = −7.58 to −1.56, P = .003), and time to full feeds (MD = −3.00 days, 95% CI = −3.80 to −2.19, P < .00001). Laparoscopic Ladd's procedure had less overall postoperative complications (OR = 0.35, 95% CI = 0.19–0.65, P = .0009), less postoperative adhesive small bowl obstruction (OR = 0.37, 95% CI = 0.19–0.74, P = .005), and more postoperative volvulus (OR = 2.97, 95% CI = 1.23–7.13, P = .02). There was no difference in incidence of reoperation rate (OR = 2.04, 95% CI = 0.96–4.33, P = .06).
Conclusion:
Laparoscopic procedure is superior to open Ladd's in operative time, hospital stay, time to full feeds, overall postoperative complication, and postoperative adhesive small bowel obstruction. However, more RCTs with adequate follow-up are needed to overcome the limitations of our study.
Introduction
Intestinal malrotation is a congenital disorder that arises from perturbations in the sequence of herniation, rotation, and fixation of the midgut, resulting in a narrowed mesenteric base, which predisposes the child to potentially fatal midgut volvulus. 1
The standard surgical procedure to treat malrotation and prevent midgut volvulus is the Ladd procedure, first described in 1936 by William Ladd, 2 the First Chief of Surgery at Boston Children's Hospital. It is performed by a transverse incision in the upper abdomen, followed by counterclockwise detorsion of midgut volvulus if present, division of the bands between the cecum and the duodenum, widening of the mesenteric root to prevent further volvulus, positioning of intestines into the nonrotation orientation, and often appendectomy to prevent future diagnostic confusion.
The first report of laparoscopic procedure of malrotation was in 1995 in a 3.6 kg, 7-day-old neonate who presented with malrotation and volvulus. 3 Similar reports followed shortly thereafter by Gross et al. 4 and Waldhausen and Sawin, 5 from separate institutions.
Reports comparing the laparoscopic Ladd procedure with the conventional open Ladd procedure have shown that laparoscopic procedure is effective and safe in adults, 6 and although several retrospective studies have indicated that the laparoscopic approach is safe and effective in infants and children,7–10 it is still not performed routinely for malrotation in infants and children.
Since van der Zee and Bax 3 reported the first laparoscopic Ladd procedure in 1995, laparoscopy has been used more frequently in infants and children with intestinal malrotation in the past 26 years. However, it still remains unknown which one of these two methods produces better outcomes. It is also unclear which approach leads to the fewest complications and shorter operation time, all of which can affect outcomes and medical costs. To compare the clinical outcomes of laparoscopic and open Ladd's procedure, we performed a systematic review and meta-analysis.
Methods
Search strategy
This systematic review and meta-analysis were performed following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. On January 5, 2021, PubMed, EMBASE, and Cochrane library were searched for studies comparing laparoscopic Ladd's procedure with open Ladd's procedure for intestinal volvulus. There were no restrictions on type language or publication date. Search terms were confined to Title/Abstract: “Intestinal Volvulus” OR “Intestinal malrotation” AND “Laparoscopy” AND “Laparotomy.” The reference lists of all related articles were manually searched to identify additional eligible studies. Randomized controlled trials (RCTs) and retrospective studies were included if they: (1) assessed the treatment of intestinal malrotation in neonates, infants, or children by laparoscopy in one group and open approaches in another; and (2) reported at least some outcomes of interest. Articles were excluded if they were duplicate reporting, case reports, editorials, conference abstracts, letters, and included adult patients.
Data management
The included studies were evaluated by 2 reviewers independently. If there were any disagreements, they would be resolved by consensus. First author, year of publication, type of study, sample size, patient age, weight and gender, and the outcomes were evaluated. Our study was limited to published research; unpublished data were unavailable to the authors.
Quality assessment
The Newcastle–Ottawa scale 11 was used to assess the quality of the articles included in our study.
Outcome indications
Outcome indications were conversion rate, length of hospital stay, operative time, time to full feeds, rate of reoperation, and overall postoperative complications including postoperative adhesive small bowel obstruction and postoperative volvulus.
Statistics
We summarized the basic study data as n (%) for the sex of patients and mean ± standard deviations (SD), median, or mean for continuous data. The outcomes were summarized as mean ± SD or mean for continuous variables and n or n (%) for dichotomous variables. Odds ratios (OR) with their 95% confidence interval (CI) was calculated to analyze dichotomous variables and mean differences (MDs) with corresponding 95% CI was used for continuous variables.
Statistical heterogeneity of studies was evaluated using the χ 2 test with significance set at P < .1, and heterogeneity was quantified using the I2. A fixed-effects model was used if I2 < 50% and a random-effects model was selected if I2 ≥ 50%. A leave-one-out method was used to conduct sensitivity analysis. Because <10 studies were included in each outcome of the review, publication bias was not assessed. Review Manager 5.4.1 (Cochrane Collaboration) was used to perform the meta-analysis.
Results
Literature screening process
The literature search identified 175 articles, of which 41 were duplications. After the initial review of titles and abstracts, 116 studies were excluded. Seventeen studies had been full text reviewed and three were excluded for not comparing laparoscopy with laparotomy and being a review article (Fig. 1).

Flow chart showing the pathway of article selection. Color images are available online.
Finally, 14 articles were included in our meta-analysis with a total of 1866 patients (n = 444 for laparoscopic approach and n = 1422 for open approach). The characteristics of the included articles are given in Table 1.12–25 The mean age at the time of operation ranged from 13.1 days to 51.9 months for the laparoscopic procedure and from11.5 days to 58.3 months for open Ladd's. For laparoscopic procedure, the mean weight at operation ranged from 3.25 to 25 kg, and for open Ladd's from 3.351 to 10.6 kg. The length of follow-up ranged from 1 to 10 years and most patients were male (range, 44%–80%).
Basic Characteristics of Studies Included in the Meta-Analysis
Median (interquartile range).
Mean (range)
Median.
Median (range).
D, days; M, months; NA, not available; NOS, Newcastle–Ottawa scale; SD, standard deviation; Y, years.
The outcomes of treatment are given in Table 2. Overall conversation rate ranged from 8% to 47%. The operative time of the laparoscopy ranged from 53 to 80 minutes and for the open Ladd's from 61 to 76 minutes. Time to full feeds for the laparoscopy ranged from 1.333 to 4.2 days and for the open Ladd's from 4.6 to 6.9 days. Length of hospital stay ranged from 2.6 to 9 days for the laparoscopic procedure, 5.3–16 days for the laparotomy. A lower rate of the overall postoperative complications and the postoperative adhesive small bowel obstruction was often observed with the laparoscopic procedure, whereas less postoperative volvulus was often associated with the open procedure. As for the reoperation rate, laparoscopy ranged from 10% to 30% and for the open Ladd's from 5% to 20%.
Summary of Outcomes and Complications
Excluding laparoscopy converted to laparotomy.
Including laparoscopy converted to laparotomy.
Including six postoperative volvulus.
Median (interquartile range).
Mean (range).
Median (range).
Median.
Outcomes for propensity score-matched patients.
NA, not available; SD, standard deviation.
Conversion rate
The overall conversion rate was reported in 11 studies, of 444 patients, who had undergone laparoscopic treatment; conversion to an open procedure was necessary for 21% of them.
Operative time
Operative time was reported in two studies. A fixed-effects model of analysis was used as a low level of heterogeneity was observed (χ 2 = 0.08; I2 = 0%, P = .78). The overall pooled analysis indicated that the laparoscopy had a shorter operative time (MD = −14.44 minutes, 95% CI = −20.79 to −8.09, P < .00001; Fig. 2A).
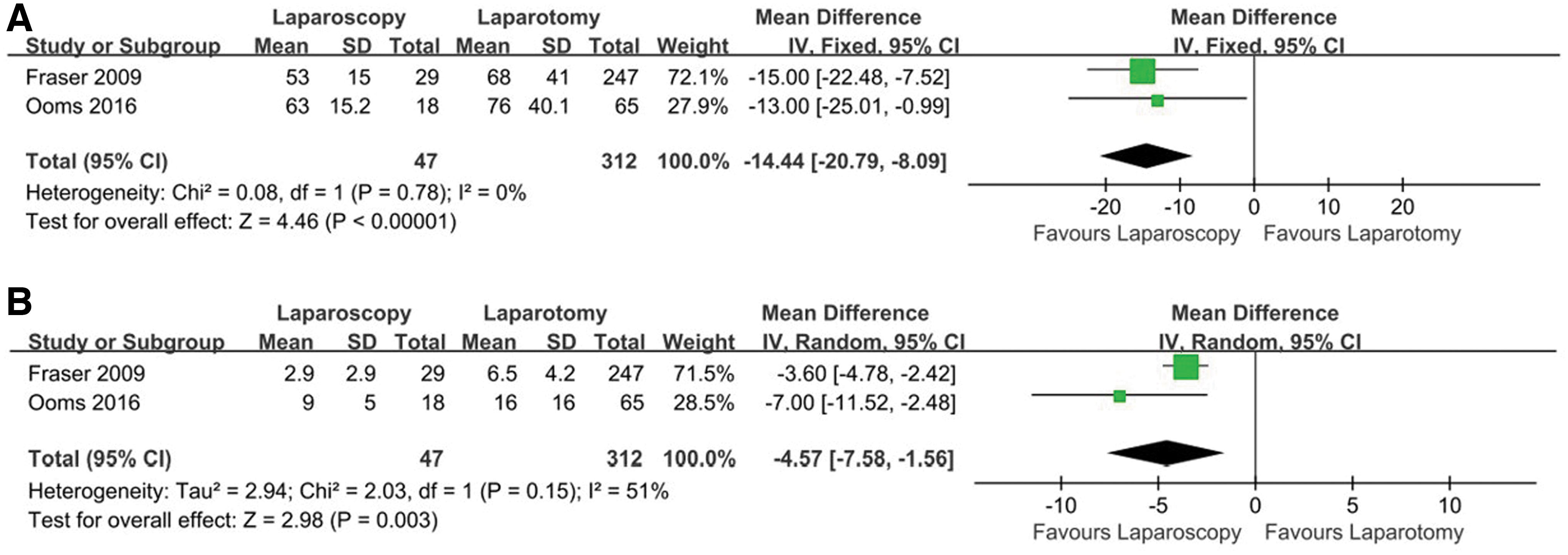
Laparoscopic versus open Ladd's: forest plot for operative time
Length of hospital stay
Two studies reported length of hospital stay. A random-effects model of analysis was selected as a significant heterogeneity degree was observed (χ 2 = 2.03, I2 = 51%, P = .15). The overall pooled analysis showed that patients with laparoscopic approach had shorter hospital stay (MD = −4.57 days, 95% CI = −7.58 to −1.56, P = .003; Fig. 2B).
Time to full feeds
Time to full feeds were reported in two studies. A fixed-effects model was selected, because no heterogeneity was seen in the data (χ 2 = 0.17, I2 = 0%, P = .68). The overall pooled analysis showed that the laparoscopy had a shorter time to full feeds (MD = −3.00 days, 95%CI = −3.80 to −2.19, P < .00001; Fig. 3).

Laparoscopic versus open Ladd's: forest plot for time to full feeds. Color images are available online.
Overall postoperative complication
Five studied reported data for the overall postoperative complication rate. Because low level of heterogeneity was seen, a fixed-effects model of analysis was selected (χ 2 = 0.54, I2 = 0%, P = .97). The overall pooled analysis showed that patients who underwent the laparoscopic approach had a lower overall postoperative complication rate than those treated by open Ladd's (OR = 0.35, 95%CI = 0.19–0.65, P = .0009; Fig. 4A).
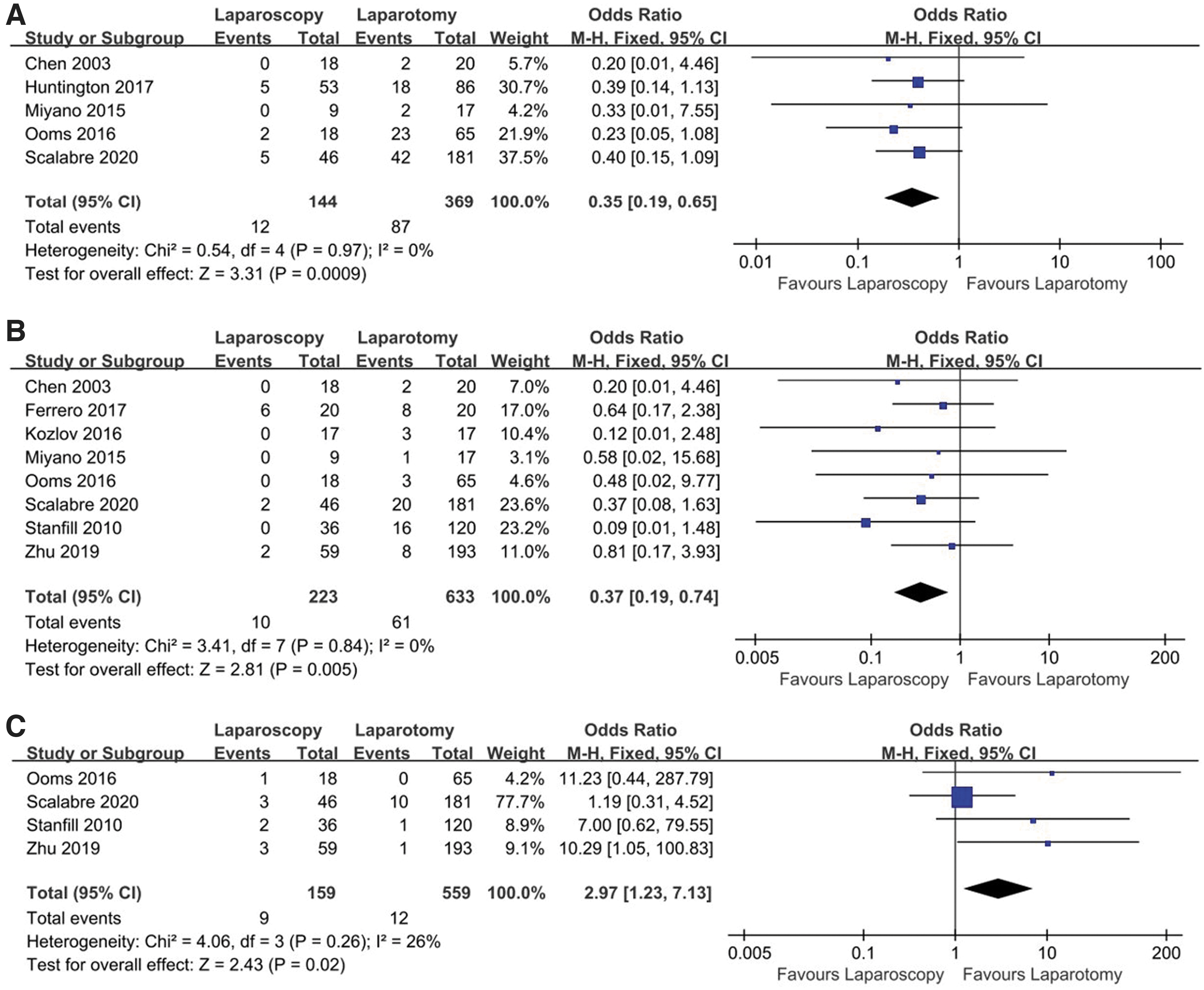
Laparoscopic versus open Ladd's: forest plot for overall postoperative complications
Postoperative adhesive small bowel obstruction
Eight studies analyzed postoperative adhesive small bowel obstruction rate. A fixed-effects model was selected, because no heterogeneity was seen (χ 2 = 3.41, I2 = 0%, P = .84). The overall pooled analysis showed that the laparoscopy had a lower incidence of postoperative adhesive small bowel obstruction (OR = 0.37, 95%CI = 0.19–0.74, P = .005; Fig. 4B).
Postoperative volvulus
Four studies reported the full data for postoperative volvulus. A fixed-effects model was selected, as low level of heterogeneity was observed (χ 2 = 4.06, I2 = 26%, P = .26). The overall pooled analysis found that patients who underwent the laparoscopy had higher postoperative volvulus rate than those treated by open Ladd's (OR = 2.97, 95% CI = 1.23–7.13, P = .02; Fig. 4C).
Reoperation
Three studies analyzed reoperation rate. A fixed-effects model was selected, because no heterogeneity was seen (χ 2 = 0.11, I2 = 0%, P = .95). The overall pooled analysis suggested that there is no significant difference between the two approaches. (OR = 2.04, 95% CI = 0.96–4.33, P = .06; Fig. 5).
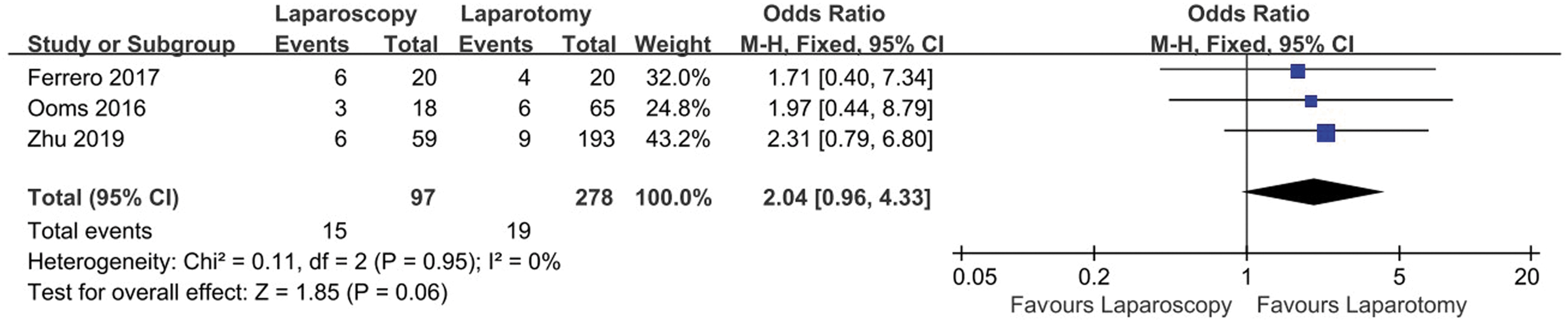
Laparoscopic versus open Ladd's: forest plot for reoperation. Color images are availableonline.
Study quality
The Newcastle–Ottawa scale was used to assess the quality of the included studies. Thirteen of them had score ≥6, with another scoring 5. The included studies had the quality to be accepted.
Sensitivity analysis
The leave-one-out method was used to analyze the sensitivity of each outcome. In terms of the outcomes, there were no significant differences with the omission of any one study, suggesting that our review was not unduly impacted by any study.
Discussion
Our research aimed to compare surgical method outcomes in children with intestinal malrotation who were treated using the laparoscopy or open approach. Fourteen studies were included. Our study suggests that the laparoscopy procedure was associated with shorter operative time, hospital stay, and time to full feeds, and in addition, lower overall postoperative complication rate, postoperative adhesive small bowel obstruction rate, and higher postoperative volvulus rate compared with the open procedure. The reoperation rate was similar for open Ladd's.
Compared with the previous study performed by Catania et al., 26 our study included 14 studies and we paid attention to more outcomes of the 2 approaches, such as operative time and reoperation rate. Catania et al. found that laparoscopy was associated with shorter hospital stay and faster time to full feeds, lower overall postoperative complication rate and higher incidence of postoperative volvulus compared with the open approach, which were similar to our study. However, they found no difference between treatments in postoperative adhesive small bowel obstruction in the laparoscopy group, which is different from our study.
In our study, we found that the laparoscopic Ladd's spend less operative time than open Ladd's. However, this result must be explained prudently because the operative time is influenced by plenty of factors, such as surgeon experience and whether the patient was with complex complications (like volvulus, bowel necrosis, and other malformation). Moreover, only two studies were included in this result, and the laparotomy group in Ooms's study had more “other surgery,” 21 which may increase the bias of the result; more RCT studies should be carried out in the future to make this result more convincible.
In this study, the overall conversion rate was 21%. The conversion may be because of the lack of surgical experience. As far as we know, there is a surgical learning curve for laparoscopic techniques; with the accumulation of experience, conversion rates may be reduced.15,21 In addition, the high conversion rate may also be influenced by the number of neonate patients included in our study, because Hsiao and Langer found that in neonates the conversion rate was as high as 50%. 16
In our study, the postoperative volvulus rate was higher in the laparoscopic group, whereas the postoperative small bowl obstruction rate of these two approaches was exactly the opposite. Some surgeons believe this may be because the open approach could facilitate adhesion development, which could keep the small bowel in the nonrotation configuration to decrease the risk for volvulus.15,21,23 As for the reoperation rate, we did not find a significant difference between these two procedures. On the one hand, the laparoscopic approach may have a higher reoperation rate for volvulus, because laparoscopy leads to fewer adhesions. On the other hand, laparotomy may result in more reoperation because of a higher risk of postoperative small bowel obstructions.15,23
Our results seem to favor laparoscopy for most of the outcomes. However, owing to the limitations of our research, the result must be interpreted with caution. The lack of randomized trials is a key problem. Most of the studies were small retrospective studies, which may lead to selection bias and may generate uneven distribution of confounding factors, such as age of patient, the year when surgery was performed, duration of follow-up, and the clinical indications. In addition, the conversion ratio is extremely high in the laparoscopic treatment groups, indicating that the patients in the laparoscopic group seem to be different from the patients in the open group, which may have led to potential bias and possibly confounded the findings. Considering these factors, more prospective randomized controlled studies compare these two surgical approaches for treating intestinal malrotation are needed in the future.
Conclusion
In summary, compared with open Ladd's, laparoscopic procedure is associated with shorter operative time, hospital stay, time to full feeds, less overall postoperative complication, less postoperative adhesive small bowel obstruction, and more postoperative volvulus. These two surgical approaches were similar with respect to the reoperation rate. However, the lack of large prospective studies cannot be ignored. More RCTs with adequate follow-up are needed to overcome limitations in the current literature.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.