
Abstract
Background:
Patients with esophageal squamous cell cancer (ESCC) have a high frequency to coincide with head and neck cancer (HNC). This study aims to analyze the treatment results and prognosis of patients with synchronous ESCC and HNC.
Methods:
From January 2016 to December 2019, 5 patients underwent concurrent surgical resection of synchronous ESCC and HNC in our institution. We retrospectively reviewed the surgical outcomes and prognosis of these patients with synchronous ESCC and HNC (HNEC group) and compared the results with those of 20 patients who underwent esophagectomy with three regional lymph node dissections for ESCC during the same period (EC group).
Results:
The locations of HNCs were pharynx/tongue (4/1) and the clinical stages were Stage IV in all patients. Meanwhile, the clinical stages of ESCCs were Stages 0/I/II/III (1/1/2/1). All patients underwent thoracoscopic esophagectomy. The surgical procedures concurrently performed for HNC were pharyngolaryngectomy with free jejunum transfer in 3 patients, wide tongue and mandibular segment resection with mandibular reconstruction in 1 patient, and mandibular transection with radial forearm flap reconstruction in 1 patient. There was no significant difference in the frequency of postoperative complication between these two groups. The HNEC group had a significantly shorter recurrence-free survival than the EC group (P = .046).
Conclusion:
Head and neck surgery with thoracoscopic esophagectomy can be safely performed concurrently with local control. The risk of recurrence is higher in ESCC patients with HNC; therefore, it is important to move on to adjuvant therapy without delay.
Background
Esophageal cancer is the sixth most leading cause of death from malignant disease in Japan. 1 The prognosis of esophageal squamous cell carcinoma (ESCC) has dramatically improved with the advent of multimodal treatment approaches such as neoadjuvant chemotherapy followed by radical esophagectomy with extensive lymphadenectomy, or chemoradiotherapy (CRT). 2 It is not uncommon to see the synchronous presentation of head and neck (H&N) cancer (HNC) in patients with ESCC.3–5 Both smoking and alcohol intake are reported to increase the prevalence of ESCC and HNC. 5
Complete removal of cancer is the mainstay of treatment for both ESCC and HNC; however, it is complicated to treat synchronous ESCC and HNC simultaneously.6–9 Esophagectomy is a highly invasive procedure associated with several serious postoperative complications, such as pneumonia, anastomotic leakage, and recurrent laryngeal nerve paralysis, which may possibly result in multiorgan failure. 10 If we perform surgery for HNC concurrent with esophagectomy, it may become considerably more invasive for these patients. Nowadays, technical advances and developments in endoscopic equipment and thoracoscopic surgery have increased the popularity of minimally invasive esophagectomy (MIE). 11
From the nationwide Japanese database, MIE is associated with a lower rate of pulmonary complications such as pneumonia than open esophagectomy. 12 MIE may possibly lower the invasiveness for patients with synchronous ESCC and HNC. Pharyngolaryngectomy with total esophagectomy (PLTE) is an effective treatment for patients with synchronous hypopharyngeal or laryngeal and thoracic esophageal cancers; however, fatal complications, such as tracheal and gastric tube necrosis, may happen. 7 Regardless of the invasiveness, the survival of patients with synchronous ESCC and HNC was similar to that of patients with solitary ESCC. 13
Another treatment strategy for synchronous ESCC and HNC may be the use of concurrent CRT. However, few therapeutic options remain for post-CRT patients with residual or recurrent disease, and salvage treatment is associated with higher postoperative mortality or morbidity.14,15 Considering these difficulties, surgical resection with reconstruction may be preferable for these patients with synchronous cancers.
In our institution, we cooperated with otorhinolaryngologists, H&N surgeons, and plastic surgeons for the treatment of patients with synchronous ESCC and HNC. Considering that plastic surgery techniques such as microvascular anastomosis and musculocutaneous flap application are frequently required, close cooperation among these departments is indispensable.6,13
We hypothesized that surgical procedures for synchronous ESCC and HNC may be safely performed, and have a good prognosis. The aim of this study was to evaluate the surgical outcomes of concurrent thoracoscopic esophagectomy and H&N surgery for patients with synchronous ESCC and HNC in our institution.
Methods
Patients
We retrospectively analyzed patients who were diagnosed with ESCC of the thoracic esophagus and HNC synchronously and who had concurrent esophagectomy with surgical resection of the HNC between April 2016 and December 2019 in Ageo Central General Hospital, Japan. We only included patients who required reconstructive surgery performed by plastic surgeons. Clinical staging was made by preoperative endoscopy and computed tomography, according to the Japanese Classification of Esophageal Cancer and HNC proposed by the Japanese treatment guidelines for Esophageal Cancer and HNC, and according to the TNM classification.16–18
Methods
Neoadjuvant therapy was performed according to the guidelines of a more advanced cancer of either ESCC or HNC.19–21 Esophageal surgeons performed thoracoscopic esophagectomy with standard mediastinal lymph node dissection in all patients. Otorhinolaryngologists and H&N surgeons performed the surgery for HNC. Plastic surgeons performed the reconstruction and pharyngogastric anastomosis. We further compared patients' backgrounds and surgical outcomes with those who underwent standard esophagectomy for isolated ESCC of the thoracic esophagus within the same study period. We excluded patients who had undergone salvage esophagectomy. This study was approved by the Institutional Review Board of Ageo Central General Hospital.
Statistical analysis
We performed statistical analyses using SPSS Statistics, version 25 (IBM Corporation, Armonk, NY). We analyzed the clinical and pathological variables using the Student's t-test for continuous variables and χ 2 test, Fisher's exact tests, and Kruskal–Wallis method for categorical variables. Survival analysis was performed using the Kaplan–Meier method, and the parameters were compared using the log-rank test. We considered differences to be statistically significant at P < .05.
Results
From January 2016 to December 2019, a total of 25 patients underwent thoracoscopic esophagectomy for ESCC of the thoracic esophagus, and 5 of them underwent concurrent surgical resection of synchronous ESCC of the thoracic esophagus and HNC in our institution.
Of these 5 patients, neoadjuvant chemotherapy was performed in 3 patients; 2 had three courses of DCF therapy (70 mg/m2 of cisplatin and 70 mg/m2 of docetaxel on day 1 and 700 mg/m2 of fluorouracil on day 1–5), and 1 had a single course of FP therapy (80 mg/m2 of cisplatin on day 1 and 800 mg/m2 of fluorouracil on day 1–5). All patients underwent thoracoscopic esophagectomy with standard mediastinal lymph node dissection for ESCC. Among these patients, the locations of HNC were pharynx/tongue (4/1) and the clinical stages were all Stage IV. The clinical stages of ESCC were Stages 0/I/II/III (1/1/2/1). The details of these patients' backgrounds are shown in Table 1.
The Characteristics of 5 Patients with Synchronous Esophageal Squamous Cell Cancer and Head and Neck Cancer
DCF, chemotherapy of docetaxel, cisplatin, and fluorouracil; ESCC, esophageal squamous cell carcinoma; FP, chemotherapy of fluorouracil and cisplatin; HNC, head and neck cancer.
The surgical procedures concurrently performed for the HNC were wide tongue and mandibular segment resection with mandibular reconstruction in Patient 1, mandibular transection with radial forearm flap reconstruction in Patient 2, and PLTE with free jejunum transfer in Patients 3–5. Patient 3 suffered anastomotic leakage of gastric tube that caused tracheoesophageal fistula. Fistula was closed with the redo-surgery performed on postoperative day (POD) 49 and seemed to be controllable; however, this patient could not move on to adjuvant therapy and died of recurrence on POD 99. Three of 5 patients moved on to postoperative concurrent CRT. The details of surgical outcomes are shown in Table 2.
The Surgical Outcomes of 5 Patients with Synchronous Esophageal Squamous Cell Cancer and Head and Neck Cancer
CCRT, concurrent chemoradiotherapy; FJT, free jejunum transfer; PLTE, pharyngolaryngectomy with total esophagectomy; VATS, video-assisted thoracic surgery.
We also compared these 5 patients who underwent concurrent surgery for synchronous ESCC and HNC (HNEC group) with those who only had esophagectomy for ESCC of the thoracic esophagus (EC group). The backgrounds of all patients are shown in Table 3. There were no significant differences in patients' backgrounds between these two groups. The surgical outcomes of all patients are shown in Table 4. The patients in the HNEC group had significantly longer operation time and significantly higher amount of blood loss than the EC group. There were no significant differences in the frequency of postoperative complication between two groups.
Patients' Backgrounds
ESCC, esophageal squamous cell cancer.
Patients' Surgical Outcomes
P < 0.05.
ESCC, esophageal squamous cell cancer.
Overall survival (OS) and recurrence-free survival (RFS) between these two groups are shown in Figure 1. At the median follow-up duration of 486 days, there were no significant differences in OS between two groups; however, patients in the HNEC group had significantly shorter RFS than the EC group (P = .046). Among the 5 patients in the HNEC group, recurrence was revealed in 3 patients (the location of recurrences: lymph node/lung/pleural dissemination; 1/1/1).
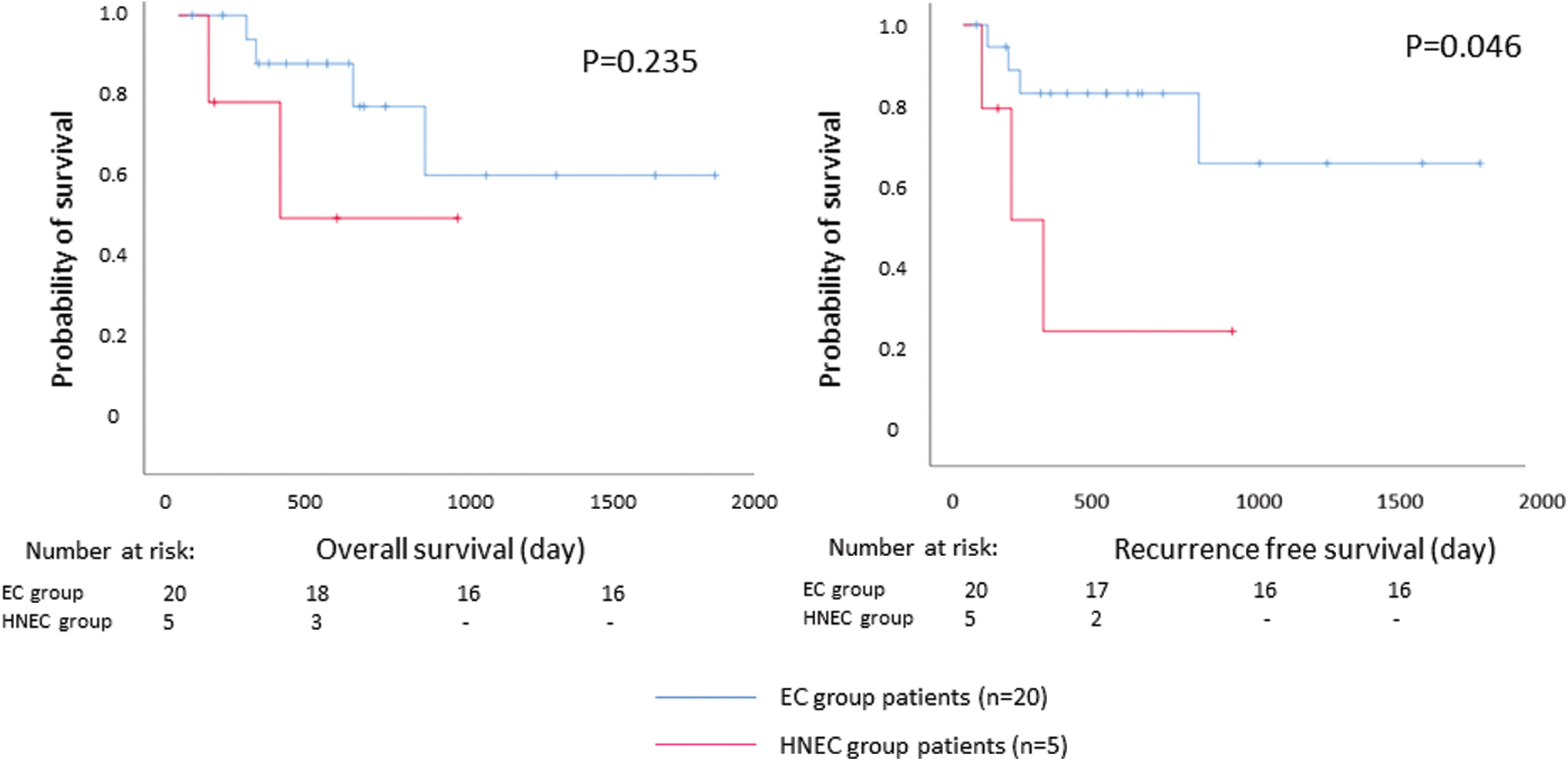
Figure 1 shows the Kaplan–Meier curves of overall survival and recurrence-free survival in the EC group and HNEC group. EC group, ESCC of the thoracic esophagus; ESCC, esophageal squamous cell cancer; HNC, head and neck cancer; HNEC group, synchronous ESCC and HNC. Color images are available online.
We performed jejunostomy for all patients who underwent esophagectomy and enteral nutrition was required until the day of discharge for 3 of 5 patients in the HNEC group.
Discussion
ESCC and HNC coincide in high frequency. The frequency of concurrent or metachronous development of these diseases is reported to be 25%–33%. 22 The correlation between genetic polymorphisms for alcohol dehydrogenase and aldehyde dehydrogenase, and alcohol carcinogenicity in the upper gastrointestinal tract is well established. 22 If we encounter patients with either ESCC or HNC, we should thoroughly examine the upper gastrointestinal tract to avoid overlooking other synchronous diseases.
Nowadays, owing to the progress of multidisciplinary treatment, ESCC and HNC can be treated by CRT. Definitive CRT tends to be the initial treatment for these synchronous double cancers. 6 However, salvage surgery may be needed in cases with residual or recurrent disease, which is generally associated with high morbidity and mortality. 23 Thus, surgical treatment may be the mainstay of treatment to achieve complete resection of the tumor.
Concurrent surgery may achieve complete resection of tumor at once. However, concurrent surgery is more invasive than either esophagectomy or HNC surgery with reconstruction, and indications must be decided carefully. In our institution, we deliberate the indication carefully in each case, with consideration of all the factors such as patients' backgrounds or comorbidities that may impair the postoperative life of the patients. We corporate with otorhinolaryngologists, H&N surgeons, and plastic surgeons for the whole treatment process of these patients. There were no significant differences in postoperative complications between those who underwent concurrent surgical resection and those who only had esophagectomy in our study. Our study suggested that one-stage concurrent surgical resection for synchronous ESCC and HNC may be a feasible and safe treatment option.
In our study, all patients underwent thoracoscopic esophagectomy. Recently, this MIE procedure has been increasingly performed worldwide. 11 According to the previous studies, MIE was associated with a longer operation time and smaller amount of blood loss than open esophagectomy. Moreover, it was associated with lower frequency of pulmonary complications, with similar mortality rate to those who underwent open esophagectomy. 12 This MIE approach can be applied for patients with synchronous ESCC and HNC.
The prognoses of patients with synchronous ESCC and HNC depend on the stage of the more advanced cancer, and the delay of the treatment for the advanced cancer may negatively influence survival. 24 Generally, HNC is difficult to detect until the symptoms appear, and is usually detected in the advanced stage. In our study, all the patients with synchronous ESCC and HNC had Stage IV HNC, which was more advanced than ESCC.
We found that RFS was significantly shorter in patients who underwent concurrent surgery. Since all patients who underwent concurrent surgery had Stage IV HNC, they may have a high risk of recurrence. Adjuvant therapy is recommended for these patients to reduce the risk of recurrence according to the guideline. 17 The delay in the adjuvant therapy may be related to the recurrence risk. In our cases, 1 patient had a complication of anastomotic leakage, which might be related to the delay of adjuvant therapy, and died of recurrent disease.
For concurrent surgery, tracheal necrosis is considered to be one of a severe complication. 7 It is commonly caused by insufficient tracheal blood flow. Thoracoscopic esophagostomy may enable us to preserve tracheal blood flow as much as possible by giving us precise view. Although we had no patients with tracheal necrosis, staged surgical resection for ESCC and HNC, respectively, may be effective to prevent tracheal necrosis by forming tracheal blood flow bypass.7,8 According to some reports, staged surgery for these patients can be effective to lessen the complications.7,8 However, if the surgery for either cancer is preceded, the growth of the other one is a concern before the next surgery. In addition, a previous study indicated that adhesions from the first surgery may increase the difficulty of the second surgery. 6
From this point of view, we consider that the concurrent surgery may be a feasible choice for patients with synchronous ESCC and HNC.
In all patients we performed jejunostomy for the postoperative nutritional management. Patients with HNC surgery may have more difficulty in oral ingestion because of phlegm congestion or difficulty in swallowing. In addition, adjuvant CRT had a possibility of adverse effect of pharyngitis. The administration of arginine-enriched enteral nutrition is reported to significantly decrease in fistulas and hospital stay in patients undergoing surgery for HNC. 25 Enteral nutrition may be effective for the management for these patients until they finished adjuvant therapy.
There are some limitations for this study. First, our study is a retrospective study with limited number of patients based on the experience of a single institution. To confirm the safety of concurrent surgical resection of ESCC and HNC, we need more accumulation of cases. Although synchronous concurrence of ESCC and HNC is frequently observed, cases in which both cancers can be curatively treated with surgery are relatively rare even in high volume centers. 24 Our study is unique in the point that included not only PLTE as a surgical method but also HNC surgery that incorporated mandibular reconstruction.
In addition, we focused on the feasibility of MIE in patients with synchronous ESCC and HNC. Second, the observation period is extremely short to conclude oncological safety, and we need more long-term outcomes to evaluate the oncological safety of concurrent surgical resection. We found a significant difference in RFS, which may possibly suggest the high risk of recurrence in patients with ESCC who synchronously have HNC. Further study must be followed to evaluate efficacy of concurrent surgery for synchronous ESCC and HNC.
In conclusion, concurrent surgical resection of ESCC and HNC by thoracoscopic esophagectomy can be safely performed and is a feasible treatment strategy for patients with synchronous ESCC and HNC. It may be important to move on to the adjuvant therapy without delay to lessen the risk of recurrence.
Conclusions
H&N surgery with thoracoscopic esophagectomy can be safely performed concurrently with local control. The risk of recurrence is higher in ESCC patients with HNC; therefore, it is important to move on to adjuvant therapy without delay.
Authors' Contributions
A.S. collected and analyzed the data and drafted the article. A.S., M.T., S.I., Y.Y., M.O., W.N., and K.O. participated in the treatment of these patients. M.T., S.I., N.O., Y.Y., M.O., W.N., K.O., and G.W. participated in revising the article critically. All authors declare that they contributed to this article and that they read and approved the final article.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.