
Abstract
Indications for pulmonary lobectomy in infants and children include cystic pulmonary adenomatoid malformation, congenital lobar emphysema, chronic infection, and malignancy. These procedures can now all be done thoracoscopically avoiding the short- and long-term morbidity of an open thoracotomy. In this article we describe the technique of thoracoscopic lobectomy as well as the preoperative and postoperative care.
Introduction
There are numerous indications requiring pulmonary lobe resections in infants and children. The majority are for the broad spectrum of bronchopulmonary malformations that present in early infancy and childhood. These include bronchogenic cysts, bronchopulmonary sequestrations (BPSs), congenital pulmonary airway malformation, and congenital lobar emphysema. 1 These lesions may be detected by prenatal ultrasound (US), present as acute respiratory distress in the newborn period, or may remain undiagnosed and asymptomatic until later in life. The other major indications include chronic infection resulting in bronchiectasis and malignancy. Treatment may vary somewhat depending on the time of diagnosis and the presentation, but in most cases complete lobar resection is the desired therapy. Minimally invasive techniques now allow these procedures to be done with much less pain and morbidity and avoid the long-term consequence of a thoracotomy in an infant or small child.
However, thoracoscopic lobectomy can be one of the most technically demanding procedures performed by a pediatric surgeon. To optimize the safety and success of these procedures, we have developed a standardized approach to perform thoracoscopic lobectomy.
Preoperative Workup
Many of these lesions are diagnosed prenatally by fetal US and the infants are born asymptomatic. Chest X-rays may show gross disease but are of limited value beyond that. The best preoperative test remains a computed tomography (CT) scan to help define the location and the extent of the disease, it may also show the presence of a systemic vessel in cases of BPSs. Some groups are advocating the use of magnetic resonance imaging (MRI) to replace CT to avoid radiation, but we currently find the definition of the lung to be suboptimal with this modality. A type and cross for blood should be sent before starting the case.
Positioning
The procedure should be performed with the patient in a lateral decubitus position with the affected side up. In most cases we prefer single lung ventilation achieved by a main stem intubation of the contralateral side. Having a collapsed and “quiet” lung helps with the identification and dissection of vital structures. In larger patients, a double lumen endotracheal tube or bronchial blocker can be used. In cases wherein single lung ventilation cannot be achieved, CO2 insufflation alone can be used. This is generally achieved with a pressure of 4–6 mm Hg and at a flow of 1–2 L/min.
The surgeon and assistant stand at the patient's front. In smaller children the patient should be placed near the edge of the table so that the handles of the instruments are not obstructed by the table (Fig. 1).
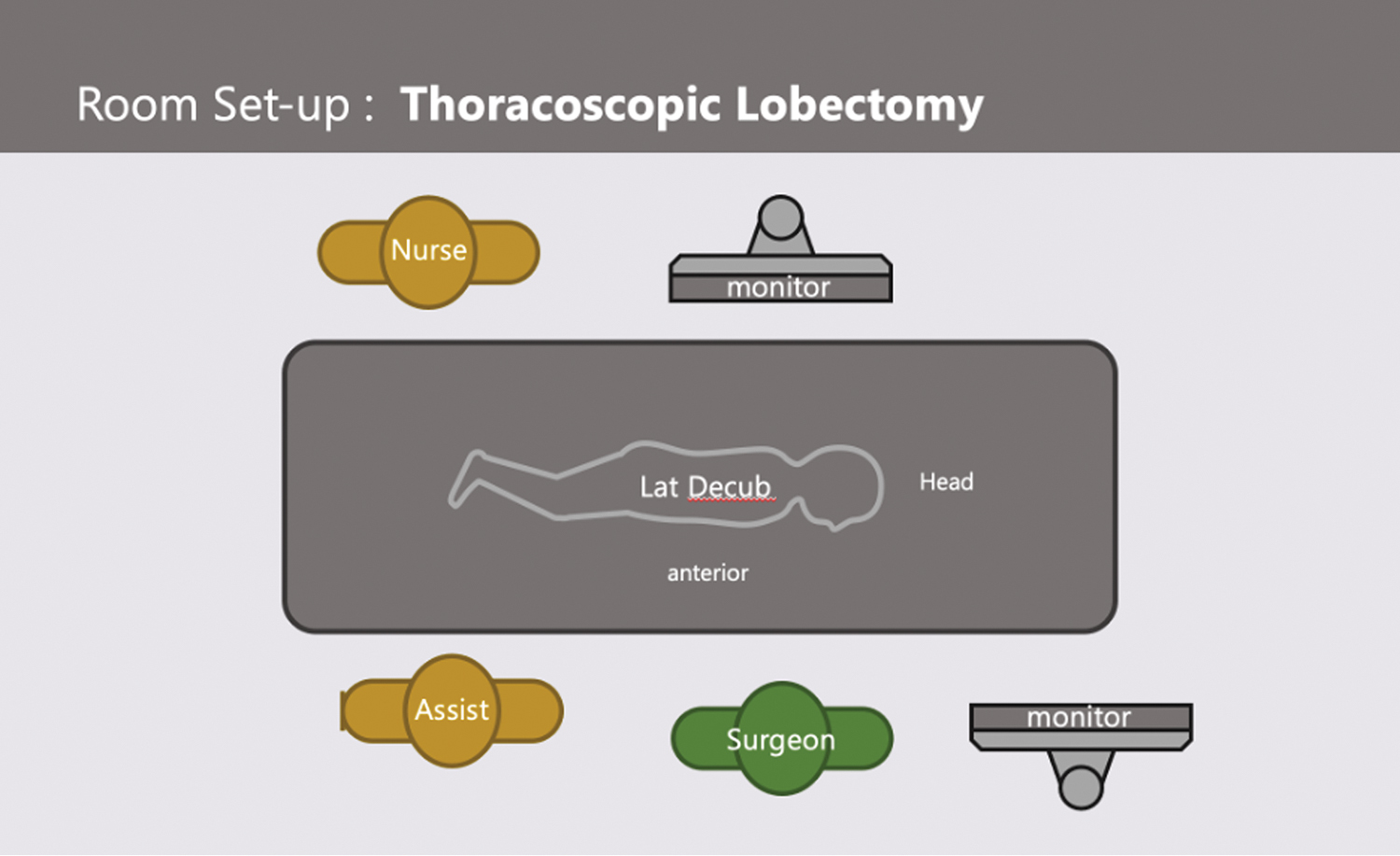
Room set-up for thoracoscopic lobectomy. Color images are available online.
Instrumentation
Three valved ports, ranging from 3 to 5 mm, are used. In the majority of cases, a bipolar vessel sealing device is used to manage the pulmonary vessels. In most cases, a 3 mm vessel sealer (Bolder Surgical [previously JustRight], Louisville, CO) is employed. In patients >15 kg, a Maryland style 5 mm Trinity CoolSeal (Bolder Surgical) is used. These devises are also used to seal and divide the lung parenchyma in cases of an incomplete fissure. The vessels are managed by obtaining adequate length of the vessel to create two seals ∼3 to 5 mm apart and then dividing the vessel between them. In larger patients (generally those >15–20 kg), a 5 or 12 mm endoscopic stapler can be used to secure some or all of the major pulmonary vessels. If these are not available, clips for smaller bronchi or division and suture ligature can be used.
Technique
The room is set up to facilitate an anterior approach. The surgeon and assistant are at the patient's front with the monitor at the patient's back (Fig. 1). First the chest is insufflated with CO2 using a Veress needle to help collapse the lung and avoid injury of the parenchyma with a trocar. Three trocars are used in almost all cases. The first port is placed in the mid to anterior axillary line in the fifth or sixth interspace to determine the position of the major fissure and evaluate the lung parenchyma. Position of the fissure should dictate the placement of the other ports. The working ports are placed in the anterior axillary line above and below the camera port (Fig. 2).

Trocar placement for LLL. Four millimeters camera port, left hand 3 mm port, and right hand 5 mm port for endoscopic stapler. LLL, left lower lobe. Color images are available online.
For a lower lobe, the inferior pulmonary ligament is taken first until the inferior pulmonary vein (PV) is exposed. During this portion, care is taken to look for a systemic vessel arising from the thoracic aorta or up through the diaphragm. The major fissure is then examined and, if necessary, completed using the vessel sealing device. This is done in a layer-by-layer technique until the pulmonary artery is seen transversing the fissure. The branches of the pulmonary artery to the lower lobe are then sealed and divided, often at the segmental level (Fig. 3). If necessary, dissection can be carried out into the parenchyma of the lower lobe to obtain adequate length of the segmental branches for safe sealing and division. Alternatively, if the right lower lobe (RLL) artery trunk is large enough and accessible, it can be taken with the 5 mm stapler (Fig. 4). After this the bronchus to the lower lobe can be visualized lying directly under the divide arterial trunk. It is mobilized and divided with the endoscopic stapler (Fig. 5). In many cases, it is beneficial to take the superior segmental bronchus first and then the trunk to the basel segments. This exposes the inferior PV trunk that can be easily divided with the 5 mm stapler (Fig. 6). If not available, the vessel should be followed proximally toward the parenchyma where it branches, and the smaller branches can be sealed and divided as already described.
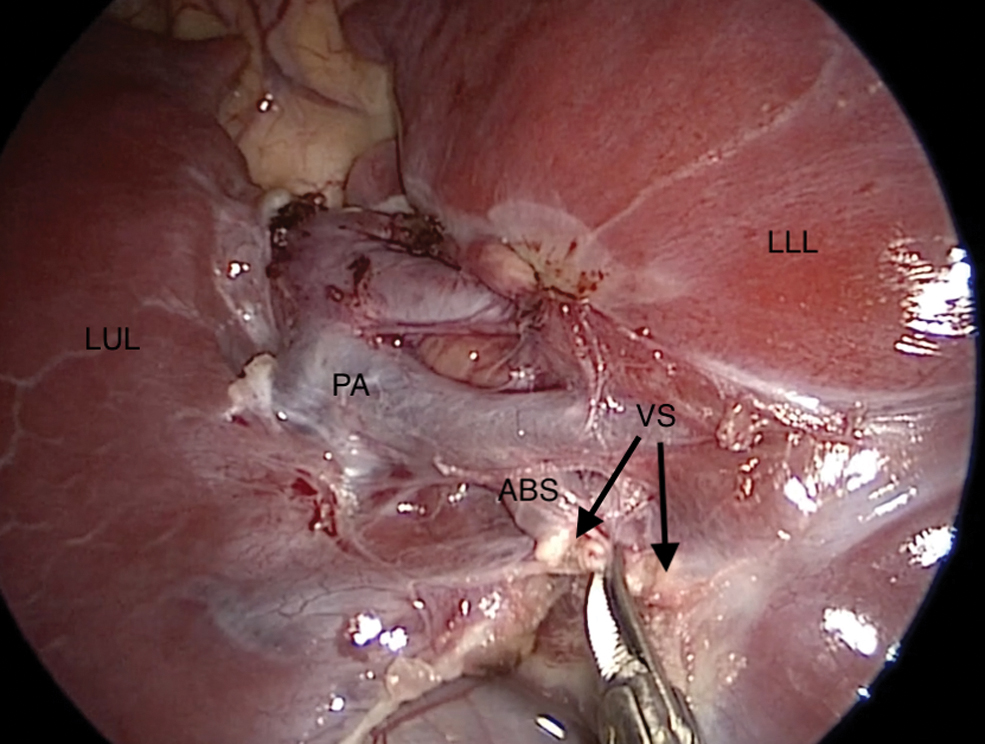
Proximal and distal seals (VS) on ABS of pulmonary artery with scissors dividing vessel between the two seals. ABS, anterior basel branch; LLL, left lower lobe; LUL, left upper lobe; PA, pulmonary artery; VS, vessel seal. Color images are available online.

Dividing main PA to LLL with 5 mm stapler. The 3 mm Maryland keeps proximal vascular control until it is clear that the staple line is secure. LLL, left lower lobe; PA, pulmonary artery. Color images are available online.

Taking bronchus to RUL with 5 mm stapler. RUL, right upper lobe. Color images are available online.
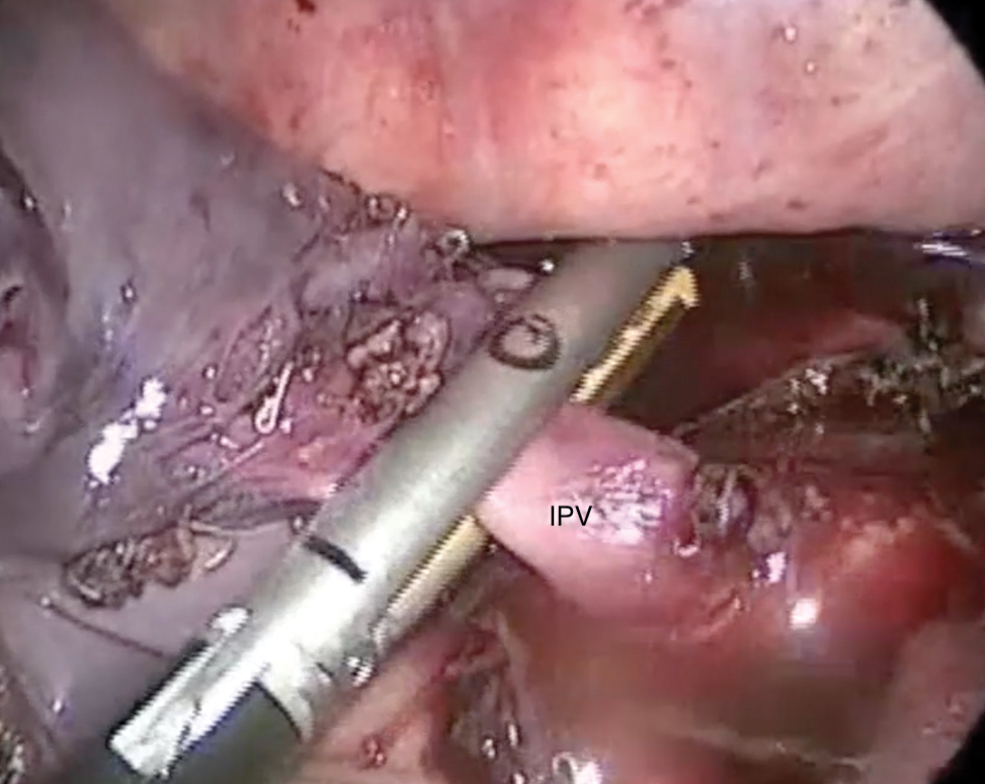
Taking the IPV to the RLL with the 5 mm stapler. Care is taken to ensure there is an adequate stump length in case there are any issues. IPV, inferior pulmonary vein; RLL, right lower lobe. Color images are available online.
In cases of upper lobe disease, the operation can be performed starting from the apex down or from the fissure up. I prefer to go from the apex down. The lung is retracted inferiorly and the anterior and apical segmental branches are taken. Dissection is then continued anteriorly where the superior PV branches are taken. The lingular vein is more inferior and taken and then the lingular artery that lies in the anterior portion of the fissure. The fissure is then completed going from anterior to posterior, and there is usually a posterior branch or the artery to the upper lobe located in the posterior aspect of the fissure. This leaves only the lingular bronchus and the bronchus to the remaining portion of the upper lobe. In most cases, these two structures are usually taken separately. Care must be taken to preserve all arterial and bronchial branches to the lower lobe as they pass through the fissure.
The right middle lobe can be fairly straight forward if the minor fissure is complete. However, it is often necessary to identify the bifurcation of the right middle lobe (RML) and right upper lobe vein to help demarcate the fissure. The surgeon needs to understand that the RML artery and bronchus enter at the posterior aspect of the fissure and may actually come off low, looking like they arise from the RLL artery and bronchus.
If there are large space-occupying cysts, these are “collapsed or popped” first using the vessel sealer. The cystic areas of the lung are grasped and energy applied. This causes the cyst to decompress and collapse, creating more intrathoracic space and improving the surgeon's ability to manipulate the lung and identify important structures. The specimen is then removed in a piecemeal manner through a slightly dilated 5 mm trocar site. A chest tube is left in all cases of lobar resection.
Postoperative Care
The patient is managed on the ward with IV narcotics for the first night. The CT is kept to 10–15 mmH2O suction. If there is no air leak, it is placed to H2O seal and an X-ray is obtained in 2 hours. If there is no pneumothorax, the CT is removed. Most patients are discharged on the first or second postoperative day.
Results
Over the past 30 years, 558 of 561 procedures were completed thoracoscopically. Operative times ranged from 35 to 240 minutes (average 115 minutes). Average operative time when a trainee was the primary surgeon was 160 minutes (N = 83), and 95 minutes when the senior surgeon was performing the procedure. There were 142 upper, 46 middle, and 373 lower lobe resections. There were four intraoperative complications (1.1%), requiring conversion to an open thoracotomy. Three of these were secondary to bleeding and one was to repair a compromised bronchus to an upper lobe after a lower lobectomy. Only one of these, a bleeding vessel to a pulmonary sequestration, occurred in the past 15 years of the study period. The postoperative complication rate was 3.3%, and 3 patients (0.8%) required re-exploration for a prolonged air leak. In 2 cases, a small accessory bronchus was found and sutured closed. In the third, no leak was identified, and the patient had no air leak postoperatively. Hospital stay (length of stay [LOS]) ranged from 1 to 16 days with a mean of 3.2 days. In patients <5 kg and <3 months of age, the average operative time was 78 minutes and LOS was 1.8 days. The postoperative complication rate was 2.6% and LOS was 2.1 days.
Discussion
Thoracoscopic lobectomy in children for congenital cystic lung disease is now an accepted and well-described technique.2–6 Most authors agree on the relative merits of a thoracoscopic approach, including less pain, shorter hospital stay, and decreased long-term morbidity, including a decreased risk of chest wall deformity, shoulder girdle weakness, and scoliosis. 7 Despite this general consensus, the adoption of this technique and surgeon comfort with the approach remains relatively low primarily because of the procedure is technically demanding and because most surgeons see a low volume of cases that results in a decreased familiarity with pulmonary anatomy. Using a thoracoscopic approach further compounds this, as the surgeons can no longer put their hand in the chest cavity to palpate the structures and identify the anatomy. Therefore, standardization of technique and approach is critical.
One of the most difficult aspects of these cases is when the fissure is incomplete and the pulmonary vessels are not readily visible. We have found that using the vessel sealing technology to dissect and divide the parenchyma of an incomplete fissure is the safest way to approach this. The fissure is approached layer by layer until the pulmonary artery is visualized. In our experience using the vessel sealer results in limited bleeding and air leak as compared with other methods.
The second issue has been standardizing an anterior approach. During an open thoracotomy, the surgeon is generally positioned at the patients back. For thoracoscopic lobectomies, the surgeon and assistant are positioned at the patient's front. This is especially important in smaller patients, as there is more room from the chest wall to the mediastinum, where the pulmonary vessels arise.
The anatomic relationships for each lobe using this anterior approach are critical. The three dimensional relationships of the vessels and bronchi to each lobe, which cannot always be seen in the two dimensional view of the scope, are critical in understanding and safely dissecting the anatomy.
The third major issue is standardizing the management of the pulmonary vessels. Early in our experience, we learned that thoracoscopic suture ligation of each individual vessel was difficult and time consuming. The small working space, difficulty in achieving traction and countertraction to obtain adequate vessel length while suturing, and the technical demands of tying a secure knot made this process laborious. We have not favored endoscopic clips for most vessels because of the risk of dislodging them during the extensive tissue manipulation necessary during a lobectomy. Therefore, we adopted vessel sealing as a way to safely mange the pulmonary vessels. 8 The 3 mm sealing device now available can seal vessels up to 5 mm and works well as a dissector especially in the smaller chest cavities of infants. It is more than adequate for most pulmonary vessels in children <10 kg, and for segmental branches in larger children. A key to using vessel-sealing technology effectively is to make proximal and distal seals on the vessel ∼3–5 mm apart. Using scissors, a partial cut is made to determine that the seals are secure and that there is no bleeding once the lumen is entered. Once the vessel is partially divided and no bleeding is seen, the vessel can be completely divided. If there appears to be some bleeding, there is an opportunity to reseal the vessel before the vessel retracts and control is lost. Because of the relatively large nature of the pulmonary vessels, and the limited space in the chest cavity, it takes very little blood to obscure the operative field and force conversion to an open thoracotomy. For this reason, we have avoided any energy devises that seal and divide the vessel in one step, because if the seal fails, the ability to salvage the situation is minimal.
For bronchus management, we initially cut and then suture the bronchus using PDS suture in smaller patients. This can be time consuming and technically demanding. We now favor the 5 mm endoscopic stapler for this task. 9 If the lobar bronchus is too large, then the bronchi can be taken at the segmental level. For example, the superior segment bronchus in a lower lobectomy can be divided separately, and then the trunk to the basal segments can be taken with a second application of the stapler. In larger patients, we used the 12 mm endoscopic linear staplers. However, because of the variations in anatomy and the proximity of the bronchus to the other lobes, extreme care must be taken to avoid compromising the other bronchi.
The timing of surgery remains somewhat controversial, but there is little evidence to suggest that delayed resection improves outcome. We favor earlier resection of prenatally diagnosed lesions before they become infected or the patients become symptomatic. We have previously documented our experience with infants <10 kg and showed that these procedures had shorter operative times, lower complication rates, and shorter hospital stays. 10 In older infants, there can be significant adenopathy and inflammation in the fissures and around the pulmonary artery, making identification and safe division of these vessels much more difficult. These procedures are technically easier in infants at or near 5 kg despite the smaller working space as evidenced by the shorter operative times in this group than older patients. The LOS in this group is also shorter. Lastly for those who argue for conservative nonoperative management of these lesions in asymptomatic patients, despite the high incidence of infection, we had 2 cases of unsuspected pulmonary blastoma. 11 We feel the risk of recurrent infection and possible malignancy outweigh the risks of intervention if a thoracoscopic approach is used in an institution with a large experience in these procedures.
Footnotes
Disclosure Statement
Dr. Rothenberg has an ownership interest in Bolder Surgical.
Funding Information
No funding was received for this article.