
Abstract
Minimally invasive surgery (MIS) in pediatric population is becoming more and more popular among pediatric urologists and now it can be considered the best treatment for nephroureterectomy that is one of the most frequent urological procedures. The main indications to MIS ureteronephrectomy in children are congenital or acquired benign conditions such as nonfunctional and/or damaging kidney, renal dysplasia, and destroyed kidneys due to obstructive or refluxing uropathy. Since ever in open urological surgery, the lateral retroperitoneal approach represents the typical way to approach this kind of surgery. Although different surgical approaches can be chosen (i.e., posterior retroperitoneal, lateral retroperitoneal, laparoscopic transperitoneal, and robotic approach), the lateral retroperitoneal approach represents the typical way to perform this kind of surgery, also with minimally invasive techniques. In this article, we illustrate the technique of retroperitoneoscopic nephroureterectomy in infants and children, reporting our experience with this technique in the past 20 years.
Introduction
Minimally invasive surgery (MIS) is becoming increasingly popular in pediatric urology and today it can be considered the gold standard in the majority of urological procedures above all in nephroureterecomy.1–4 This kind of operation in open surgery is usually carried out by the extraperitoneal approach. Retroperitoneal approach was also used in the first MIS pediatric nephrectomy at the beginning of 90s when Chandhoke and Gaur described the first cases in the literature.5–7 In almost the same period, Ehrlich et al. reported the initial experience of laparoscopic nephroureterectomy. 1
Nowadays, the laparoscopic approach to the urological procedures is the most popular among pediatric urologists for the major working space and for the favorable ergonomic. Although the retroperitoneoscopic approach had a gradual decrease due to the difficulty for beginners (less working space, orientation troubles, ergonomic), its use is now rapidly increasing, especially in pediatric urological centers.
This kind of approach has a number of advantages because it is completely safe for the bowel and grants an easy conversion to open traditional surgery in case of complication. Furthermore, for the latter reason, retroperitoneoscopy should be considered as the first choice in urological centers that want to start MIS in urological surgery. In this article, we report our experience of step-by-step nephroureterectomy by the retroperitoneal approach.
Preoperative Phase
Preoperative assessment according to the native pathology includes renal ultrasound, DMSA scan, and eventually cystourethrogram to exclude vesicoureteral reflux; this last investigation can be useful to decide whether ureteral stump must be closed during the operation. In some limited cases, cystoscopy may be helpful to clarify complex anatomy.
Complete blood count, creatinine, electrolytes, coagulation tests, and blood type are usually required and broad-spectrum antibiotic prophylaxis should be administered routinely or according to the child's specific urine testing.
Retroperitoneal approach does not require a full bowel preparation and a simple preoperative enema can be adequate. Patient's parents have to sign a specific informed consent before the procedure.
Patients receive a general anesthesia with orotracheal intubation and muscle relaxation. A Foley catheter into the bladder and a nasogastric tube are placed before surgery.
Positioning
The patient should be placed in a lateral position with the side of interest facing upward, breaking the operating table and/or positioning a soft roll under the declive flank to widen the space between the 11th rib and the iliac crest (especially in infants in whom the working space is limited) (Fig. 1). The back of the patient should stay near the lateral edge of the operating table to allow a wide instrument angulation and to prevent conflict. The surgeon and the assistant stand behind the patient and the scrub nurse stands at the feet of the table (little patients). The monitor is positioned in front and toward the head and the anesthesiologist is in the usual position.

The patient is positioned in lateral decubitus position. The bending of the operating table allows to widen the space between the 11th rib and the iliac crest. Color images are available online.
Surgical accesses
The landmarks for the access are the XI or XII rib (depending on the patient's size, age), the iliac crest, and the paraspinal muscles; it can be useful to mark them with a demographic pencil. The first access is usually done at the tip of the XI rib through an open incision no longer than 1 cm (depending on the size of the first trocar [5 or 10 mm]) and then the muscular layers are gradually split until the retroperitoneal space. In order to confirm the correct access and to facilitate the introduction of the smooth forceps (Fig. 2), the identification of the retroperitoneal fat is a useful trick. At this point, if possible, the opening of Gerota's fascia under direct vision can be useful and the retroperitoneal space (virtual) can be gradually created by smooth dissection with wet gauzes, finger, and optical device (depending on patient and trocar's size (Fig. 3). Positioning a proper balloon trocar is now advisable because it is more stable and it allows to keep the position when the surgeon pulls it up to widen the retroperitoneal space (Fig. 4). Once the balloon trocar is inserted, the CO2 insufflation (7–10 mmHg) and the oscillating movements of the optical device along the paravertebral and psoas muscles are useful to complete the creation of the retroperitoneal operative space. We prefer to use 30° optical device to have more angle of vision according to its rotation.
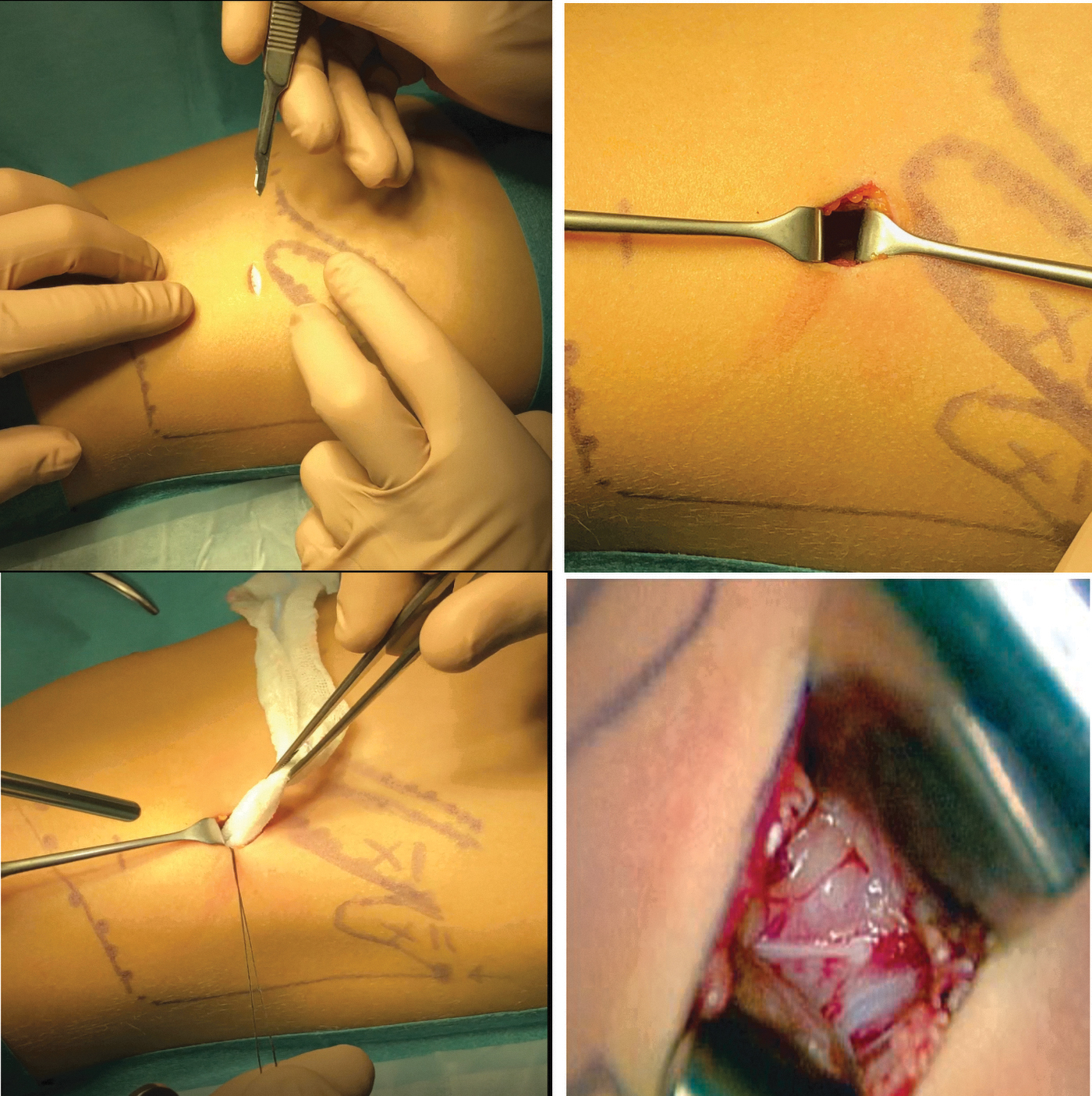
Incision and access to retroperitoneal space. Color images are available online.

Creation of retroperitoneal space with smooth dissection can be performed in different ways (i.e., wet gauzes, finger, and optical device). Color images are available online.
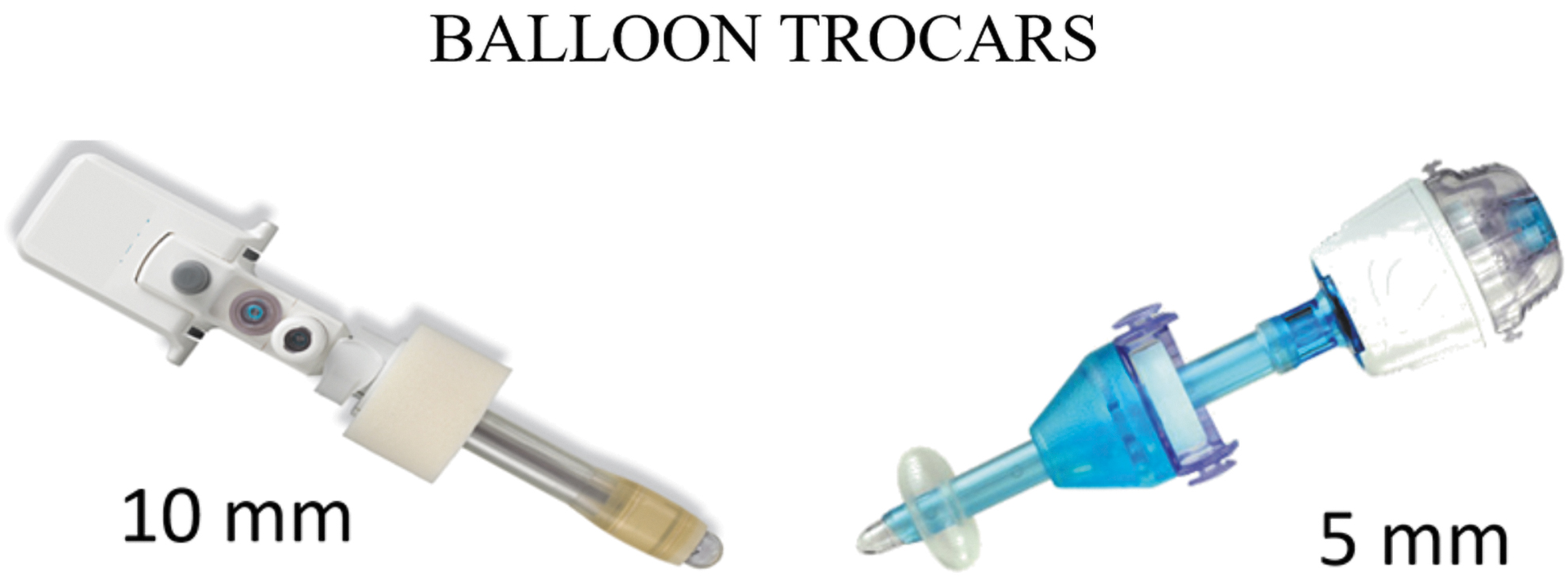
Different types and sizes of balloon trocars allowing stability during the procedure. Color images are available online.
Two or more operative 3–5 mm trocars are then inserted under direct vision: the first trocar is usually placed at the anterosuperior edge of the iliac crest (along the middle axillary line) and the second trocar at the costovertebral angle of the XII rib; a third accessory trocar can be placed along paravertebral muscle line inferiorly if needed (Fig. 5). The posterior peritoneum is gently dislocated anteriorly and superiorly from the lumbar musculature, paying attention not to detach the kidney from it; blunt instruments and hook coagulation may facilitate the dissection. Care must be taken to avoid peritoneum damage; a small hole would cause the passage of CO2 in the abdomen losing the retroperitoneal space, making the procedure very difficult. Orientation in the retroperitoneal space is not easy, so the surgeons, especially the beginners, should know to have the kidney above the operating field and the lumbar and psoas muscle on the ground to be sure of the correct dissection.
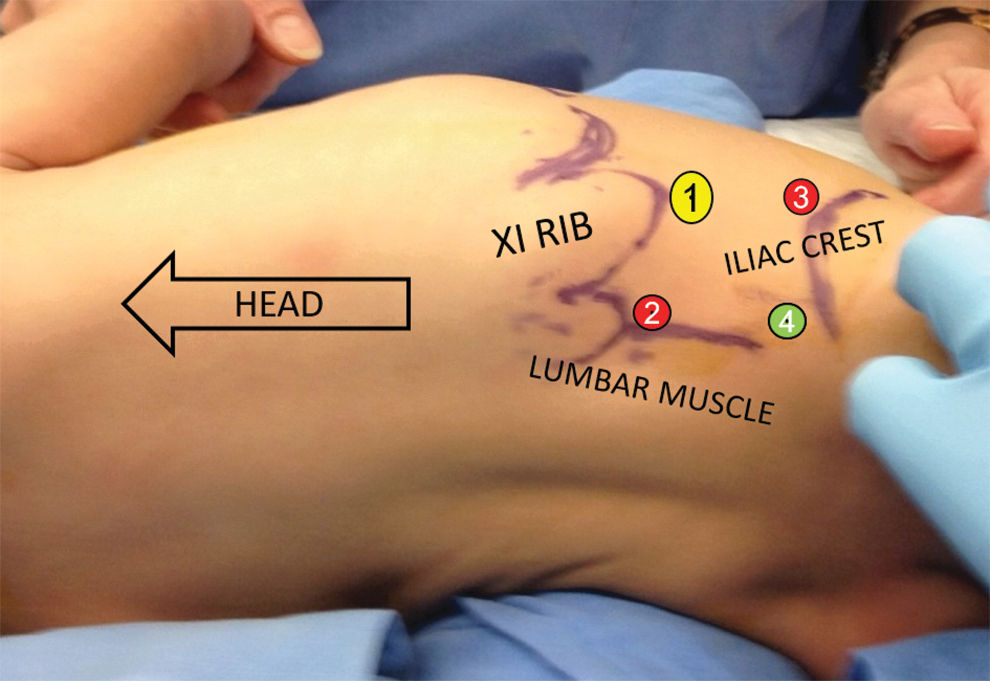
Trocar's position. We prefer to use two or three operative trocars (3 or 5 mm): one at the anterosuperior edge of the iliac crest, one at the costovertebral angle of the XII rib, and one along the paravertebral muscle line. Color images are available online.
Technique
As already described, the main anatomical landmark in the retroperitoneal space are lumbar and psoas muscles lying horizontally and inferiorly to the operating field. In this way the kidney is approached posteriorly and its the anterior surface stays attached to the peritoneum that suspended it upward; to understand that in this way the kidney is approached posteriorly is very important. Once the ureter and the hilum are identified, the aim of the surgeon is to dissect the hilar vessels. During the first phase, it is important not to detach the anterior surface of kidney from peritoneum to maintain a good operative space; the dissection of the vessels is obtained with blunt instruments and gentle CO2 insufflation pressure that progressively pushes the kidney forward and upward together with the peritoneum. Sometimes the kidney can be too heavy and the surgeon might constantly lift it up with one of the two instruments, performing the dissection of the hilum with only one instrument (not advisable); in this case it might be more comfortable to place a third 3-mm service trocar to keep the kidney lifted. The posterior approach to the kidney allows an easier identification and ligation of the renal vesssels (Fig. 6). In some cases accessory polar renal vessels are present and they should be sealed if needed. The ligation and dissection of the vessels can be performed according to the preference of the surgeon and the size of the trocars (i.e., simple ligature, clips, bipolar forceps, and advanced sealing devices). According to our experience, the electrothermal bipolar vessel sealing system guarantees a safe and fast control of the hilum. After that, the ureter should be dissected as much lower as possible (lower than the iliac vessels when possible) and finally sectioned and left open. Large refluxing ureter (RU) should be closed distally (ligature, clips, etc.) to prevent leakage of urine from the bladder (Fig. 7); in case of doubt of leakage (RU), injection of methylene blue through the ureteral catheter can be helpful. At this point, the devascularized kidney can be gradually freed from peritoneal adhesions, obtaining a complete mobilization. The surgical specimen is extracted through the optical trocar access, widening the incision if necessary. Before removing the trocars, it is very important to check the operative field and especially the sealing of the renal pedicle to prevent bleeding. Depending on the surgeon's preference, retroperitoneal drainage can be placed to control any postoperative bleeding.

Retroperitoneal access to the renal hilum identifying the ilar vessels. Color images are available online.
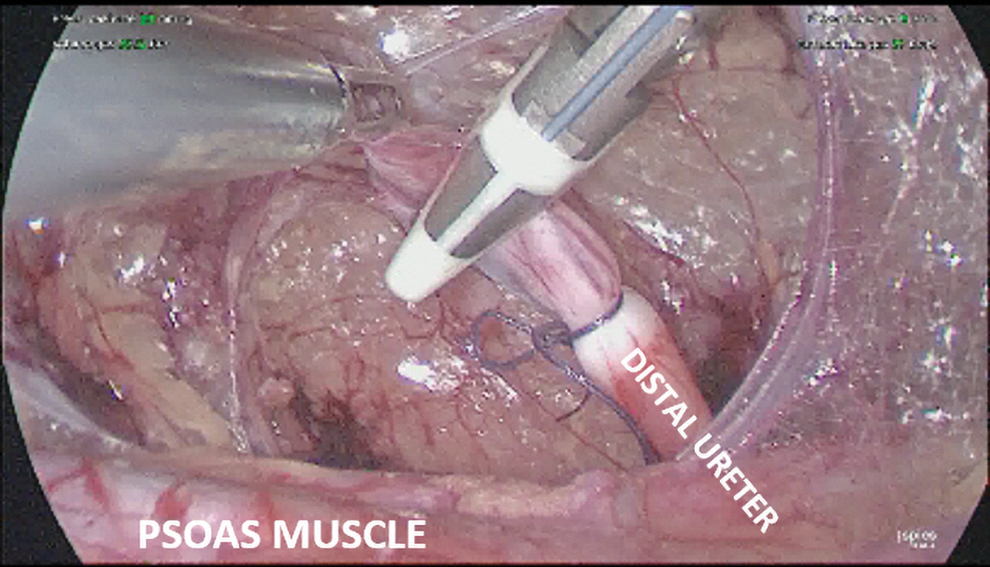
Ligation and section of the distal ureter. Color images are available online.
Postoperative Care
In case of retroperitoneal approach, bowel movements start very fast, whereby the patients can start oral feeding few hours postoperatively. Analgesic therapy with paracetamol (dose 15 mg/kg 8-hour interval) and antibiotic prophylaxis can be administered for 12–24 hours postoperatively. Perirenal drainage is advisable above all in postpyelonephritis kidneys and it can be removed 24 hours postoperatively. The patient is usually discharged in 2 p.o. days.
Results
In 20 years of experience, we performed 138 nephrectomies for nonmalignant disease with MIS. Of these, 112 were carried out by the retroperitoneoscopic approach. The main indications to surgery were nonfunctioning kidney (secondary to obstruction, reflux, or ectopic ureter), multicystic dysplastic kidney, post-traumatic renal failure, and renal hypertension: 6 patients had a horseshoe kidney, 4 were misdiagnosed. None required conversion to open surgery and no major intra- or postoperative complications were reported. Eight patients had a residual ureteral stump (7 in the first 60 patients and 1 in the remaining); 2 out of 8 patients underwent successfull laparoscopic surgical removal for recurrent urinary tract infections. The duration of the procedure ranged from 40 to 120 minutes (median 95 minutes) depending on the surgeon's experience and the complexity of the pathology (recurrent pyelonephritis, horseshoe kidney). The median hospital stay was 3 days (range 1 to 5 days), very short in case of multicystic kidney.
Even though the retroperitoneoscopic approach allows an easy access to the renal vessels at the hilum, the space creation and the correct understanding of the anatomy require high skills and specific training. To maintain the orientation, the psoas muscle must always be identified to the base of the operating field, whereas the kidney has to be located in the anterosuperior part. The great vessels (inferior vena cava on the right and aorta on the left) are relatively close and they need to be carefully preserved to avoid harmful lesions during the maneuvers. Compared with the transperitoneal access, the cardiac and respiratory effects of the retropneumoperitoneum are unremarkable; further the risk of lesions to the intra-abdominal organs and the postoperative adhesions are reduced to the minimum. Finally the retroperitoneal access does not jeopardize the conversion to open surgery with lateral access (normally preferred by the pediatric urology specialists).
Discussion
Since the first descriptions of laparoscopic nephrectomy in children 8 and retroperitoneal operative laparoscopy,5,6 the technological improvements have expanded their indications and now MIS is considered the gold standard for almost all nephrectomies, especially for simple nephrectomy and ureter–heminephrectomy for nonmalignant diseases. Even though the first reports of retroperitoneal laparoscopic nephrectomy in children have been reported in the same years,9–12 the choice between transperitoneal and retroperitoneal MIS approaches is still debated. In fact, the retroperitoneal approach in children still requires a high level of experience by the surgeon and his team, and excellent imaging of the retroperitoneal space as more recently reported by Al-Hazmi and Farraj. 13 The retroperitoneal approach can be obtained through lateral or posterior approach 14 ; according to the literature 15 and our experience, the lateral approach seems to be easier, giving a better visualization and removal of the distal ureter. 16 Although the first reports did not recommend retroperitoneal laparoscopy in infants, 14 the increased use of minimally invasive techniques permits to consider retroperitoneoscopy also in these patients and more and more urological centers are adopting this approach.15,17,18 Our series, which is one of the largest in the pediatric population, supports this concept and suggests retroperitoneal nephrectomy as an effective procedure with a low rate of complications. In fact the cardiac and respiratory effects of the retropneumoscopy are unremarkable compared with the transperitoneal approach, and the risk of lesions to the intra-abdominal organs or the risks to develop adhesions are reduced to a minimum with this kind of access. Furthermore, the retroperitoneal access can be easily converted to an open retroperitoneal approach that is usually preferred by the pediatric urologist. Moreover, as already described by El-Ghoneimi et al., it has a reasonable learning curve also in infants 19 and in our series, this was demonstrated by the reduction of operative time with the standardization of the technique. Despite the literature reporting a higher rate of conversion, a higher number of major complications, and higher length of surgery after partial retroperitoneal nephrectomy than transperitoneal approach, 20 in our series these variables were not different between laparoscopic and retroperitoneal approaches for nephrectomy in children. Moreover, the retroperitoneoscopic approach allowed less mobilization of colon, reducing the risk of injury to hollow viscera, and peritoneal adhesions as recently described by Taghavi for heminephrectomy. 21 In conclusion, although retroperitoneoscopy still presents some limitations (i.e., difficulties of orientation, limited working space), we believe that it can be considered the treatment of choice for nephrectomy in infants and children if performed by expert surgeons. According to our experience, retroperitoneoscopic nephrectomy is a safe procedure with a very low rate of intra- or postoperative complications and it guarantees a faster postoperative course and less discomfort for the patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.