
Abstract
Introduction:
For the past 20 years, robotic surgical systems have been used for the Roux-en-Y gastric bypass (RYGB). The da Vinci Surgical System (Intuitive Surgical, Inc.) has been one of the most used robotic platforms. This study aims to retrospectively compare the performance of two models of surgical robots.
Materials and Methods:
A retrospective comparative study was conducted from a prospective database including all patients who underwent robotic RYGB (RRYGB) from 2011 to 2020.
Results:
Of a total of 277 patients included, 134 were in the RRYGB using the da Vinci S™ (RRYGB-S™) group and 143 were in the RRYGB using the da Vinci Xi™ (RRYGB-Xi™) group. The mean operative time in the RRYGB-S and RRYGB-Xi groups was 154 ± 28 and 151 ± 32 minutes, respectively (P = .510). The was no statistically significant difference in terms of intraoperative complications between the groups with regard to positive blue test, bleeding, and failure of stapler line. The readmission rate was higher in the RRGB-S group (14.1%) than in the RRYGB-Xi group (3.4%) (P = .004), and it was mainly due to major complications (P = .003) including pouch and gastrojejunostomy anastomotic leaks (P = .001). The nonsurgical complications were statistically significantly higher in the RRYGB-S group (7.4%) than in the RRYGB-Xi group (2.1%) (P < .05), as well as the surgical complications were higher in the RRYGB-S group (7.5%) than in the RRYGB-Xi group (0%) (P < .001). The mean percentage of the total weight loss at 1 and 2 years of follow-up did not show any statistically significant difference (P = .547).
Conclusions:
The higher complication rate in the S surgical system might be correlated with the initial learning curve and stressed the need for proper robotic surgical training and accurate strategies when introducing emerging technologies into the surgical practice.
Background
Bariatric surgery is commonly considered a demanding field, the structural anatomy, increased abdominal wall thickness, hepatomegaly, and consistent visceral fat volume lead to a reduced intra-abdominal space. Additionally, in the case of Roux-en-Y gastric bypass (RYGB), complex reconstructions are required, demanding high operators' proficiency during anastomotic suturing as well as advance laparoscopic skills. In this sense, robotic systems were compelling implemented in RYGB with the aim to overcome the limitations of laparoscopy, allowing for precise tissue manipulation and greater dexterity. 1 Horgan and Vanuno were the first to report the seminal work of robotic RYGB (RRYGB) in 2001, and since then, robotic platforms have been rapidly adopted in the western countries and all over the world. 2 Besides some drawbacks of the robotic surgery have been highlighted, such as higher operative times due to docking and a lack of haptic feedback, several studies have proved that this can be minimized once the learning curve has been achieved.3–5 Additionally, some authors have reported that the robotic surgical system can aid surgeons to improve clinical outcomes in critical procedures such as patients with super obesity and revisional surgery. 6 Finally, in terms of cost analysis, the use of robotic systems has proved in clinical trials long-term superiority due to the lower incidence of complications compared with the classical laparoscopic approach.7,8
The da Vinci Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA, USA) is one of the most used platforms worldwide. The robotic platform consists of three components, namely surgeon console, patient's cart, and vision cart. The fourth generation referred as the da Vinci Xi™ system was introduced in 2014. This newer version has been designed to overcome many of the predecessor's shortcomings with a substantial improvement in multiquadrant surgery due to the refine range of motion.9–11 Briefly, in the latest robotic system, the mobile platform with mounted robotic arms accounts with longer instruments' (59.2 cm) offering a higher range of motion, allowing for a better anatomical access serving as advantage for patients with morbid and super morbid obesity.
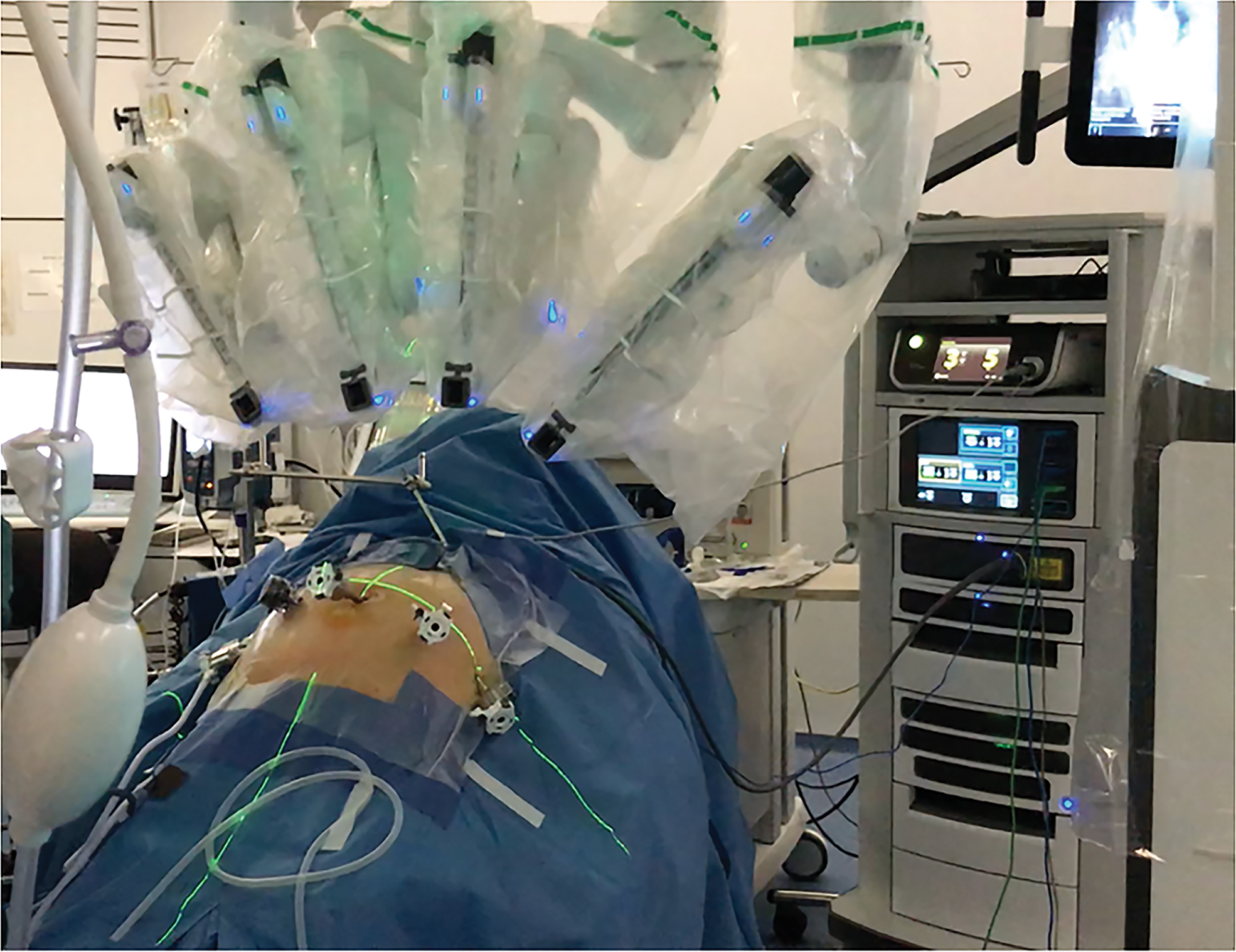
These robotic universal arms allow for the insertion of any robotic instrument including the camera.4,12 The da Vinci Xi system also contains a new architecture style with an adaptive user's interface offering easier robotic setup enhancing substantially the surgical workflow. By instance, the patient's cart can be placed aside from the patients' lateral position (right/left) (Fig. 1), which is more convenient compared with the previous S™ platform that required the placement in the patient's cephalic end creating spatial constraints for the anesthetic team (Fig. 2).
da Vinci Xi™ system setup during simulation. Please note the side entrance of the motor-driven patient cart. Color images are available online.

da Vinci S™ system setup after docking during an RYGB. Please note the entrance of the motor-driven patient cart at the patient's head. RYGB, Roux-en-Y gastric bypass. Color images are available online.
The da Vinci Xi system accounts with integrated energy sources with a single device for monopolar, bipolar energy, and vessel sealer. Additionally, it has a standard integration of near-infrared (NIR) technology (Firefly™ Fluorescence Imaging) as well as stapling EndoWrist™ instrumentation with intuitive motion. 13
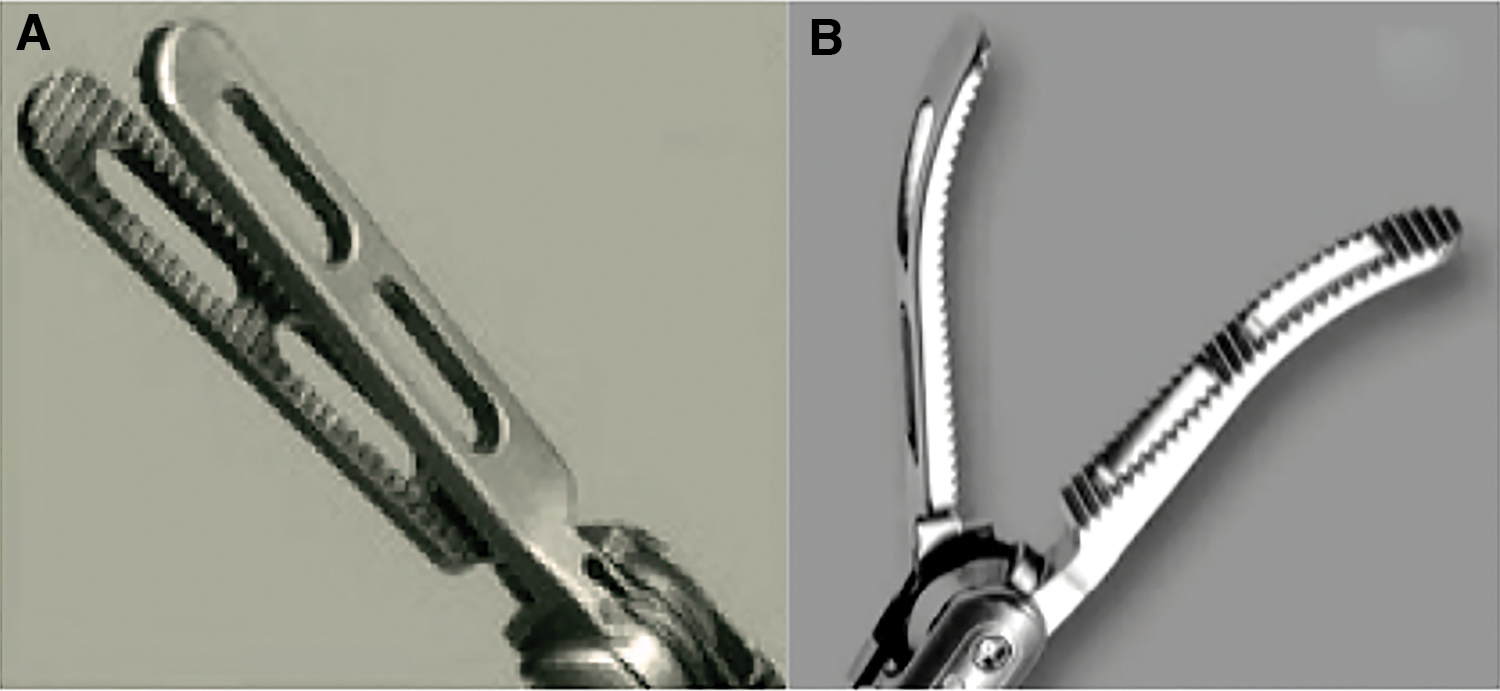
As for the stapler devices, differences in the features of robotic graspers used to manipulate the small bowel have also been adjusted. In the S generation, the system had a very strong grip, which could easily cause damage to the small bowel (Fig. 3A). The double-fenestrated graspers used in the first platforms were replaced by Tip-Up fenestrated graspers in the Xi generation allowing for a softer tissue's grip, thereby preventing from inadvertent complications (Fig. 3B). These improved factors in the latest robotic technology might positively impact the outcomes in RRYGB. Literature lack studies that compare the performance of surgical robots in bariatric surgery. This study aims to compare the clinical outcomes in two models of the da Vinci robotic surgical system.
Materials and Methods
Since 2009, our Bariatric and Metabolic Unit started to use the robotic surgical systems with the second generation of the da Vinci S system, which was replaced by the da Vinci Xi system in 2016. To evaluate the repercussion of the innovation and evolution of these two robotic platforms in our practice, we decided to conduct a retrospective comparative study of a prospective database including all our RRYGB cases.
Patients' selection
All patients were managed in a tertiary care and teaching center. A multidisciplinary team evaluation was performed according to the Bariatric and Metabolic Unit protocol. Surgical indication of bariatric surgery was based on the criteria of the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Patients who were eligible candidates for RYGB signed the informed consent. After ethical board approval, a retrospective comparative study was conducted by accessing our prospective database comprising a total of 277 patients from January 2011 to March 2020. We divided them into two groups according to the robotic surgical model, namely RRYGB using the da Vinci S™ (RRYGB-S™) accounted for 134 patients and RRYGB using the da Vinci Xi™ (RRYGB-Xi™) accounted for 143 patients. Variables for demographics such as gender, preoperative body mass index (BMI), and main obesity-related comorbidities (diabetes mellitus, hypertension, hypercholesterolemia, and obstructive sleep apnea) were evaluated.
Technical aspects
Robotic surgery technique
The patients were positioned in a supine 30° Fowler's position with closed legs. We used six ports in all cases: four 8-mm trocars, one 12-mm trocar, and one 5-mm trocar. A liver retractor was introduced via an epigastric incision. Four robotic arms were used for the procedure. A retrogastric window was created in the lesser omentum to construct a 30–50 mL gastric pouch by means of a 60 mm Echelon Flex™ linear stapler (Ethicon, USA), and a calibrating device was used during the creation of the pouch. The gastrojejunostomy (G-J) was performed in a hand-sewn double-layer manner in an antecolic antegastric position with polyglactin and polydioxanone 3/0. The jejunojejunostomy was created with an Echelon Flex linear stapler and sutures. The biliopancreatic limb was measured at a 100 cm length. The Roux limb (alimentary limb) was created in an antegastric and antecolic position, with a 130 cm length. Since nowadays there is no consensus regarding the best alimentary limb length, our protocol adapted the classical proximal gastric bypass described by Wittgrove and Clark, which referred an alimentary limb of 150 cm. 14
The mesenteric defect was closed in both robotic groups. However, Petersen's space was closed only in the RRYGB-Xi group. Finally, to rule out any potential leakage, an intraoperative double endoluminal methylene blue (MB) leak test was performed. In the latest cases, an indocyanine green test (ICG test) using Firefly Fluorescence Imaging was performed at the end of the surgical procedure (Fig. 4A, B). ICG was infused intravenously (IV) to evaluate the perfusion of the anastomosis and intraluminal through an orogastric tube to rule out fluorophore leakage. The ICG test has been recently implemented in the RYGB to evaluate intraoperative leakages that could be missed using the standard MB test. 15
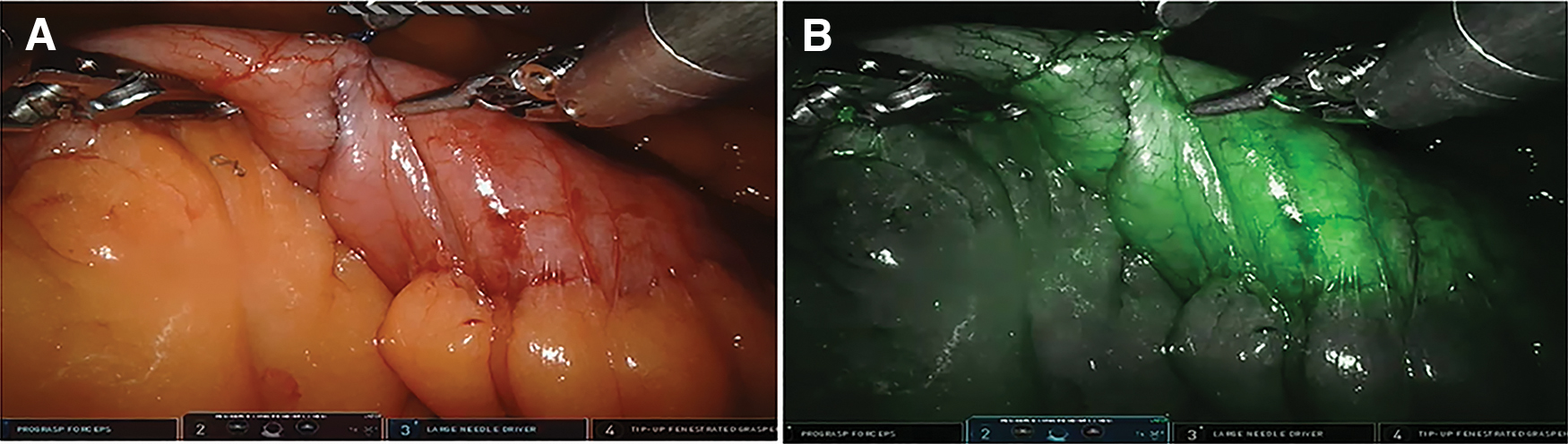
Gastrojejunostomy double test during the RRYGB procedure with the Xi™ system.
Robotic bariatric postoperative care
Due to the outcomes improvement reported with the enhance recovery after surgery (ERAS), 16 our institution started the use of the ERAS pathway in the Bariatric Unit since 2017. The protocol includes the reduction of drains and catheters as much as possible, restrictive fluid therapy, and oral resumption with clear fluid intake after surgery. IV infusions are discontinued on postoperative day 1, and incentive spirometry was provided as well. The formal ERAS was mostly used in the RRYGB-Xi group. All our patients used intermittent compression socks during surgery as well as 8 hours postoperatively to prevent thromboembolic events during their hospital stay. After discharge, all patients received a subcutaneous low-molecular-weight heparin for 4 weeks.
Thirty-day outcomes
The analyzed variables included operative time, intraoperative complications (MB leakage test, bleeding, and perforation), length of hospital stay, postoperative 30-day morbidity, which was graded according to the Clavien–Dindo classification. 17 Surgical complications (reoperation) and nonsurgical complications (deep venous thrombosis, pulmonary embolism, pneumonia, wound infection/seroma, urinary tract infection, and gastrointestinal bleeding), and mortality rate were recorded as well.
Follow-up
The main variables analyzed during the follow-up (FU) regarding weight loss are expressed as a percentage of the total weight loss [%TWL = 100 × (BMI current–BMI baseline/BMI baseline)] and the BMI delta between the first and second year (ΔBMI). The complications associated with the procedure were also described during FU.
Statistical analysis
Parametric and nonparametric data are expressed as mean and standard deviation and median (interquartile range), respectively. Statistical analysis was performed using the IBM® SPSS® Statistics Software version 24.0 (Chicago, USA). Confidence intervals were set at 95%. A two-sided P value ≤.05 was considered statistically significant. Two-sided t-tests were performed for continuous variables. Comparisons for categorical variables were performed using χ 2 test (chi-squared test) and Fisher's exact test when an observed value was <5.
Results
During the study period, a total of 277 patients underwent RRYGB: 134 in the RRYGB-S group and 143 in the RRYGB-Xi group. The mean patient’ age was 45.4 ± 9.4 years in the RRYGB-S group and 47 ± 7.6 years in the RRYGB-Xi group. Most of them were women in both groups, with a preoperative BMI of 43.32 and 43.94 kg/m2 for the RRYGB-S and RRYGB-Xi groups, respectively (P = .806). The robotic surgical groups were statistically comparable in terms of demographic data (Table 1).
Patients' Demographic Data of Robotic Roux-en-Y Gastric Bypass (S and Xi)
BMI, body mass index; OSAS, obstructive sleep apnea syndrome; RRYGB, robotic Roux-en-Y gastric bypass.
Thirty-day outcomes
The mean operative time in the RRYGB-S and RRYGB-Xi groups was 154.7 ± 28 and 151.2 ± 32 minutes, respectively. The length of hospital stay was longer in the RRYGB-S group with 4.9 ± 11 days without reaching statistically significant difference (P = .492). The intraoperative complications were similar in both groups (7.4 versus 7.0) (P = .535). The ICG test was only performed in some of patients of the da Vinci RRYGB-Xi group, and all the positive tests were detected with MB in standard white light. In case of G-J leak detected with MB, the management consisted of interrupted sutures. There was no G-J ischemic area detected in the serosal side after ICG IV near-infrared test. The perfusion was evaluated always after the anastomosis creation in a static manner without quantification of ICG diffusion or time to peak. Our RRYGB results regarding NIR fluorescence-guided surgery have published recently as part of the IHU-IRCAD-EAES EURO-FIGS registry. 18
The 30-day postoperative complication rate was higher in the RRYGB-S group (11.9%), accounting for pouch and G-J leakage rate (7.46%; P = .001), jejunojejunostomy leakage rate (1.49%; P = .236), intra-abdominal bleeding rate (0.75%; P = .50), and other origins (2.1%; P = .360). For the RRYGB-Xi group, the incidence of complications was 2.1%; the majority of them were intra-abdominal bleeding (1.4%). Overall mortality was 0%. There were no cases of deep venous thrombosis or thromboembolism during the study (Fig. 5 and Table 2).
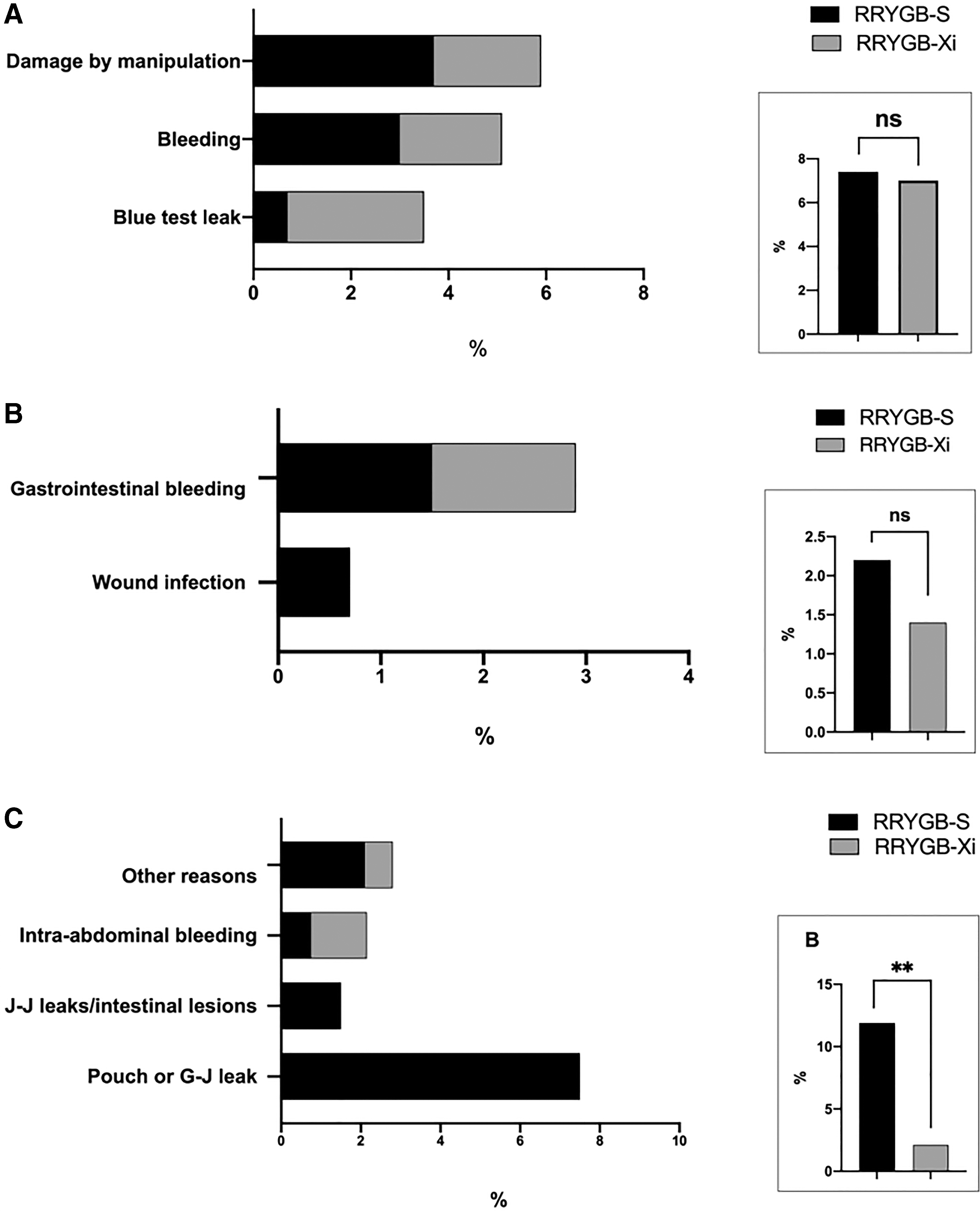
Thirty-day complications between groups.
Thirty Days OF Outcomes of Robotic Roux-en-Y Gastric Bypass (S and Xi da Vinci system)
Bold values denote statistical significance at the P < 0.05 level.
Injuries caused with robotic graspers, that is, perforation, serosal injury, or incomplete laceration.
Clavien–Dindo classification for surgical complications.
Other reasons: suspicions of perforation, small bowel obstruction.
G-J, gastrojejunostomy leakage; J-J, jejunojejunostomy leakage; RRYGB, robotic Roux-en-Y gastric bypass.
Follow-up
During the FU, complications were higher in the RRYGB-S group (14.2%; P < .001) and included G-J stricture, hypoglycemia, marginal ulcer, small bowel obstruction, chronic abdominal pain, and ventral/internal hernia. The RRYGB-Xi group had a complication rate of 2.1%; 1 patient had a marginal ulcer and 2 patients presented with a G-J stricture. Although there were five anastomotic strictures in the da Vinci RRYGB-S group, the difference did not reach any statistically significant difference (Fig. 6C and Table 3).
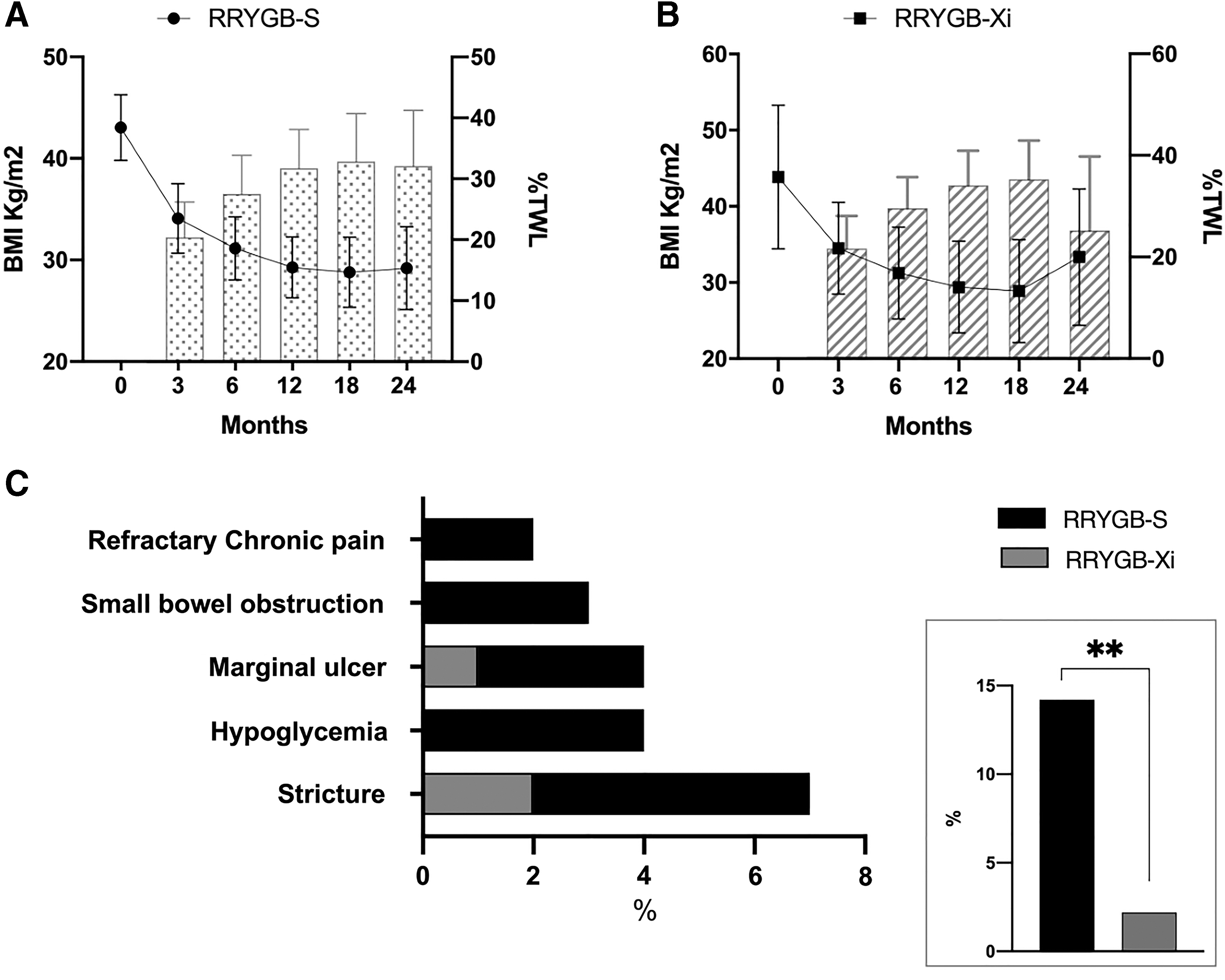
Follow-up outcomes in the RRYGB da Vinci system S™ and Xi™.
Follow-up Outcomes at 1 and 2 Years After Robotic Roux-en-Y Gastric Bypass (S and Xi da Vinci system)
Bold values denote statistical significance at the P < 0.05 level.
Adhesions and port site hernia.
%TWL, percentage of total weight lost; BMI, body mass index; G-J, gastrojejunostomy; RRYGB, robotic Roux-en-Y gastric bypass.
The median FU in the RRYGB-S group was 66.61 ± 15 months and 23.75 ± 8 months in the RRYGB-Xi group (P ≤ .001). The RRYGB-Xi group had a lower FU period because these patients underwent surgery more recently (2018) compared with the RRYGB-S group. At 1 and 2 years, there was no statistical difference in terms of %TWL. At 1 year, the %TWL was 32.9 ± 7.9 and 35.3 ± 7.5 for the RRYGB-S and RRYGB-Xi groups, respectively (P = .573). At 2 years, the %TWL was 32.1 ± 9.1 and 34.2 ± 10.23 for the RRYGB-S and RRYGB-Xi groups, respectively (P = .547) (Fig. 6A, B and Table 3).
At 1 year of FU, ΔBMI was 14.2 ± 3.68 in the RRYGB-S group and 15.3 ± 3.6 in the RRYGB-Xi group (P = .132). After 2 years, the mean ΔBMI was 13.89 ± 3 and 15.1 ± 4.9 (P = .573) in the RRYGB-S and RRYGB-Xi groups, respectively. The reoperation rate during the FU was significantly lower in the RRYGB-Xi group (0%) (P < .001) (Fig. 7 and Table 3).
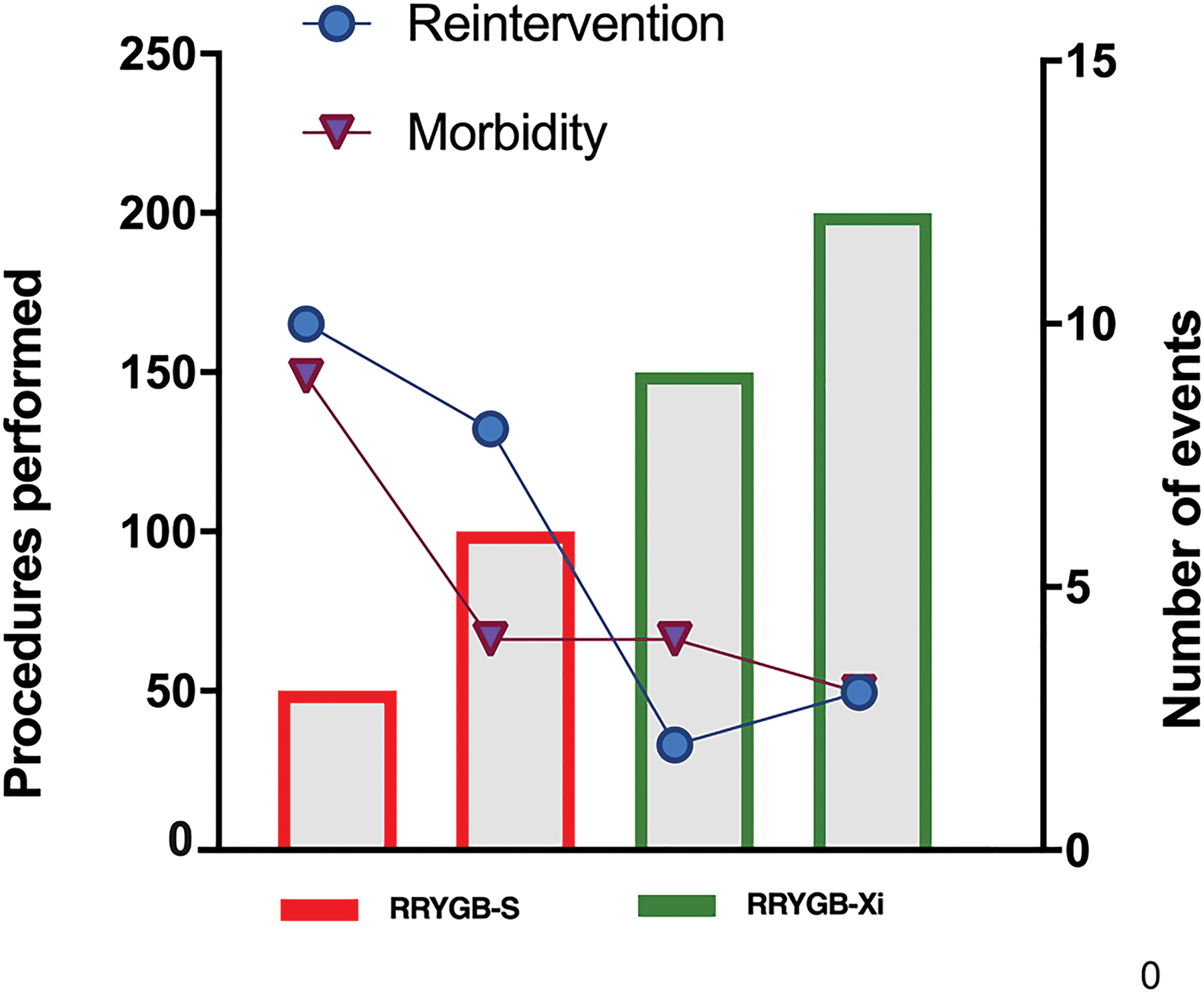
Bar graphic of the procedures performed ranging from 50 to 200 cases (left side) and complications associated with the sequential group of procedures (right side). Color images are available online.
Discussion
Undoubtedly, robotic surgery has proved to be feasible and safe; it is a promising technology that might enhance surgical proficiency in complex procedures such as patients with obesity and revisional surgery. The incremental use of robotic systems in bariatric surgery highlights the relevance in understanding its current role and the implementation of emerging technologies into the surgical practice. This study is one of the few articles that compared two robotic platforms in bariatric surgery.
The results in terms of operative time show comparable times in the two robotic surgical systems (227 ± 61 and 219 ± 59 minutes for S and Xi, respectively; P = .22). A recent article published by Niclauss et al. comparing RRYGB-Si™ versus RRYGB-Xi found an operative time of 153.7 ± 28 minutes in the da Vinci for Si and 151.2 ± 32 minutes for Xi (P = .510), which assembles the results of our study. Nevertheless, in their study, G-J and jejunojejunostomy times were significantly longer with the Si system; the G-J took 37 ± 15 minutes versus 26 ± 10 minutes for Si versus Xi (P < .0001), and the jejunojejunostomy took 31 ± 11 minutes versus 22 ± 7 minutes for Si versus Xi (P < .0001). These results suggested higher proficiency while using the latest platform, decreased conflicts between arms could also account for the differences in time.
It is important to stress that we performed a totally robotic approach with hand-sewn G-J on both platforms contrarily to the technique described by Niclauss et al. in which the hand-sewn G-J was performed only in the Si group. 19 In our standard RRYGB, the G-J is performed in the left upper quadrant and has no real technical challenge during the placement of the robotic arms. However, during the jejunojejunostomy, the overall system requires a particularly high range of motion and reach of instruments as the anastomosis is performed near the left abdominal wall.
Although our study did not express G-J and jejunojejunostomy times independently, we subjectively consider that in our practice anastomotic times in the da Vinci RRYGB-Xi group were shorter. The reason might originate from an improvement in our skills and from the standardization of our anastomotic suturing technique, which includes monofilament sutures allowing to perform two to three rows without pulling, thereby saving time.
Anastomotic leak as a complication is a major contributor of the morbidity and mortality associated with bariatric surgery. 20 Since G-J requires advanced laparoscopic skills, 4 the robotic systems could improve surgeon's performance. Additionally, they have the advantage of minimizing surgeon's fatigue facilitating completely hand-sewn anastomoses. The use of surgical robots requires a proper training to reach an optimal proficiency level; in RRYGB, the reported learning curve is considered around 50 cases. 21 The clear advantage of complete hand-sewn anastomoses has been extensively studied. 22 Recently, a meta-analysis from Kostakis et al. plotted five studies to compare the leak rate and four studies to compare stricture rate, both meta-analyses favored the robotic groups. 23
Although our study did not find any statistically significant difference in terms of minor complications (2.2% and 1.4% in the S and RRYGB-Xi groups, respectively, P = .676), there was a statistically significant higher incidence of major complications in the RRYGB-S group. The 11.9% of major complication in the da Vinci S mostly accounted for G-J leak in 7.46%, jejunostomy leak in 1.49%, and intra-abdominal bleeding in 0.75% contrarily to the da Vinci Xi in which the 2.1% of major complication mostly accounted for intra-abdominal bleeding in 1.4%. Compared with our results, Niclauss et al. found similar minor complications (10.3% and 13.9% in the Si and RRYGB-Xi groups, respectively, P = .31) and major complications (5.1% and 5.6% in the Si and RRYGB-Xi groups, respectively, P = 1) between the robotic groups. 19
Our incidence of major complication in the da Vinci RRYGB-S group overpasses the laparoscopic benchmark in the cutoff for bariatric procedures (>IIIa), which is estimated at 5.5%. In 2019, Gero et al. reported this value during a multicentric trial analysis (39,424 cases). 24 This significant higher incidence in the da Vinci S can be alarming, and we should not accept this increased complication rate without a concerted effort to improve surgical care. Nevertheless, we must stress that literature reports of complications during robotic initial experience tent to be more prevalent. Fourman and Saber found similar rates during the analysis of six studies, which showed their “initial experience” in RRYGB from 2006 to 2011. The authors found a complication rate of 10.2% (range: 0%–24.1%). 25 In our study, the da Vinci S system was the first robotic platform adopted at our institution, and the higher complication rate in this group could be correlated with our learning curve during the initial implementation of the robotic technology.
Multiple factors likely contributed to the increased perioperative complications, as matter of fact the atypical leaks in the upper part of the pouch presented in the RRYGB-S group could be explained by technical particularities. The stapler model used during the first RRYGB in 2011 was the EC60A (Echelon Flex Articulating Endoscopic Linear Cutter), which had a length of 34 cm (from the end of the rotating knob to the tip of the cartridge). To create the gastric pouch, the assistant surgeon fired the stapler from the right side of the patient. Due to the short stapler length, difficulties arose especially during the last two firings at the level of the angle of His. Afterward, longer lengths of staplers were introduced in the marketplace, and since 2016, we used the LONG60A (Echelon Flex Articulating Endoscopic Linear Cutter) system, which has a total length of 44 cm. Consequently, after the implementations of longer stapler devices, our leak rate dropped drastically to 2.1%, compared with the existing literature. More recently, we have enforced the use of the robotic EndoWrist Stapler (Intuitive Surgical, Inc.) in the da Vinci Xi system.
RRYGB as the treatment of obesity has an increasing prevalence, 26 and nowadays, the da Vinci system is the most widely used robotic platform. Although some robotic emerging platforms that have been introduced recently into the clinical practice 27 and more are awaited to be disseminated in the near future,28,29 some institutes still account with the previous version such as the da Vinci S system. To the best of our knowledge, this is one of the very few studies that compare the two robotic surgical systems in bariatric surgery, and we expect that our data will positively impact the existing literature. Additionally, our results also represent in some way the challenges while introducing new technologies as part of the surgical practice and must stress the need for precise training and interim analysis minimizing as much as possible potential risks.
A significant drawback of our study lies in the fact that the cohorts originated from two different time spans with different evolving surgeons, learning curves, and technologies.
In conclusion, our study gathered meaningful insight into these versatile machines identifying fewer postoperative complications with the latest platform once our learning curve had been consolidated.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.