
Abstract
Background:
Large cell neuroendocrine carcinoma (LCNEC) of the liver, gallbladder, pancreas, and ampulla is rare and usually arises in case reports, and thus to date, no studies have well described the treatment options and outcomes of those patients.
Methods:
The data of 108 patients diagnosed as hepatopancreatobiliary and ampulla LCNEC between 2004 and 2015 were retrieved from the surveillance, epidemiology, and final results.
Results:
In the entire cohort, the median overall survival (OS) was 10 months. For nonmetastatic patients, the median OS was 32 months for surgery of the primary tumor alone (n = 17), 19 months for surgery of the primary tumor and adjuvant therapy (n = 19), and 1 month for nonsurgical treatment (n = 8). For metastatic patients, the median OS was 14 months for patients who received surgery of the primary tumor with and without adjuvant therapy (n = 16), 9 months for patients undergoing adjuvant treatment alone (n = 30), and 1 month for patients who had no treatment (n = 16). Multivariate analysis revealed that surgery of the primary tumor was an independent factor for improved survival.
Conclusions:
This disease offers a very poor prognosis despite aggressive treatment. Radical resection is the first choice for resectable tumors, whereas surgical resection of the primary tumor plus adjuvant therapy might represent a valid option for metastatic disease. However, further studies are needed to confirm this.
Introduction
Neuroendocrine tumors (NENs) are relatively rare and heterogeneous diseases, accounting for ∼2% of patients with malignancies. 1 According to the 2010 World Health Organization definition, NENs of the digestive system are usually subcategorized into grade-1 NEN, grade-2 NEN, grade-3 neuroendocrine carcinoma (NEC), and mixed adeno NEC. 2 The characteristics of NEC are mitotic activity >20/10 high power field and >20% Ki-67 index. 2 Compared with a small cell type, large cell NEC (LCNEC) is three times larger in size, has richer cytoplasm, prominent nucleolus, and higher mitotic activity.3,4 Besides, the growth pattern of this tumor is frequently diffuse, nested, and trabecula, with a presence of necrotic areas.3,4 The diagnosis depends on histopathological and immunohistochemical findings.
In general, LCNEC may arise in any organ of the individual. 2 The two most common primary lesions are the lung and gastrointestinal tract. 5 LCNEC originated from the gastrointestinal tract is highly aggressive and frequently associated with metastatic disease. 5 Until now, there is limited data regarding the treatment options and outcomes of hepatopancreatobiliary and ampulla LCNEC because previous studies are case reports or small sample retrospective researches.4,6–8 Therefore, this study was to investigate the outcomes of different treatment regimens in patients with hepatopancreatobiliary and ampulla LCNEC and to identify potential prognostic factors for the survival of those patients.
Materials and Methods
Study population
Given the rarity of LCNEC, we conducted this retrospective study by obtaining data from the Surveillance, Epidemiology, and End Results (SEER) database. The inclusion criteria of this study were as follows. (1) Patient: the primary sites from the liver, extrahepatic bile duct, gallbladder, pancreas, and ampulla, with corresponding SEER site codes are C22.0-C22.1, C24.0-C24.9, C23.9, C25.0-C25.9, C24.1; confirmed by pathology as LCNEC; (2) intervene: it provides information on surgical resection of primary and metastatic lesions, as well as chemotherapy and radiotherapy; and (3) outcomes: with known survival time and vital status. Patients <18 years old or without a definite SEER stage were excluded. The research was approved by our Institutional Review Board (IRB). We did not register this study, so we cannot provide the clinical trial registration number.
Data collection
We extracted data according to a predetermined proforma. Data collected on patient included primary site (liver, extrahepatic bile duct, gallbladder, pancreas, or ampulla), age (<65, ≥65), gender, race (white, black, and others), year of diagnosis, tumor size, tumor grade (I-well, II-moderately, III-poorly, and IV-undifferentiated), SEER stage, the metastatic site (liver, lung, bone, and brain), chemotherapy (yes or no), radiotherapy (yes or no), surgery of primary and metastatic lesions (yes or no), survival time, and vital status.
Statistical analysis
The SPSS 18.0 software (IMB, Inc., Chicago, IL) was used to perform all data analysis. The tumor size was expressed in the median (range), whereas the absolute value was applied to describe dichotomous variables. Kruskal–Wallis and Fisher exact testing compared differences between study groups, and the two-tailed P value <.05 was defined as statistically significant. Survival curves were performed using the Kaplan–Meier method and compared using the log-rank test. Cox proportional model was employed to analyze factors potentially influencing the prognosis of patients with LCNEC, and accordingly, hazard ratios with corresponding 95% confidence interval (CI) were produced.
Results
Baseline characteristics
We initially produced 444,802 results. Figure 1 shows the patient selection procedure. After filtering non-LCNEC, 164 records were left. Then, 56 patients were excluded because of the following reasons: lack of positive histology (n = 12), unclear SEER stage (n = 31), and unknown information on tumor size, surgery, and survival months (n = 13). Finally, a total of 108 patients fulfilled the inclusion criteria for analytical.
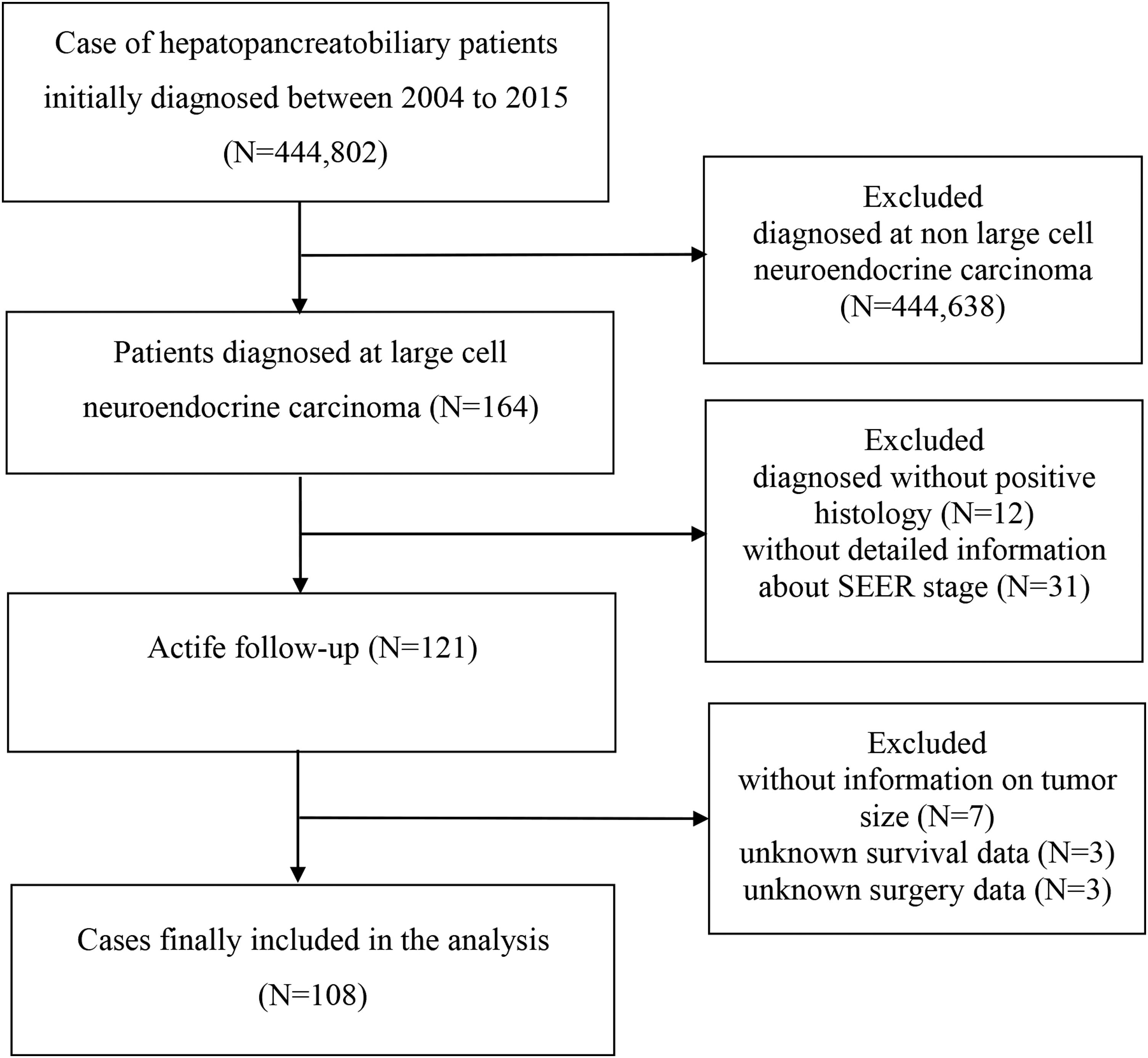
Flowchart of population inclusion of the study. SEER, Surveillance, Epidemiology, and End Result.
The primary site from the pancreas, the gallbladder, the ampulla, and the liver was 61.1% (66/108), 20.3% (22/108), 9.3% (10/108), and 9.3% (10/108), respectively. Among these, most patients were white (75.9%) and older than 65 years (56.5%), and males were slightly more than females (Table 1). About 59.3% of the patients were poorly differentiated and undifferentiated, whereas 5.6% were moderately and well differentiated. The median tumor size was 4.5 (0–22.5) cm. According to the SEER stage, 59.3% of the patients (n = 64) had distant metastatic lesions. Table 1 describes the main patient characteristics. Besides, the SEER database recorded the available information of distant metastatic lesions after 2010, 35 patients developed liver metastases, accounting for 72.9% (35/48) of the metastatic patients in the same period (between 2010 and 2015). Of the 35 patients with liver metastases, 32 originated from the pancreas.
Characteristics of 108 Patients with Large Cell Neuroendocrine Carcinoma
American Indian/AK Native, Asian/Pacific Islander.
I-well, II-moderately, III-poorly, IV-undifferentiated.
SEER, Surveillance, Epidemiology, and End Result.
Patients were divided into four groups according to the different primary sites. The intergroup analysis showed that there were no significant differences between the groups in terms of age, gender, race, year of diagnosis, chemotherapy, and radiotherapy. The four groups differed significantly regarding median tumor size (P = .000), tumor grade (P = .000), SEER stage (P = .000), and surgery of the primary tumor (P = .000).
Treatment options
Figure 2 lists detailed treatment options for all patients. In nonmetastatic patients, 17 (38.6%) were treated with surgery of the primary tumor alone (SURG 1), 19 (43.2%) were managed by surgery of the primary tumor and adjuvant therapy (SURG 2), 2 underwent adjuvant therapy (AT) alone, and the remaining 6 received no treatment (NT).
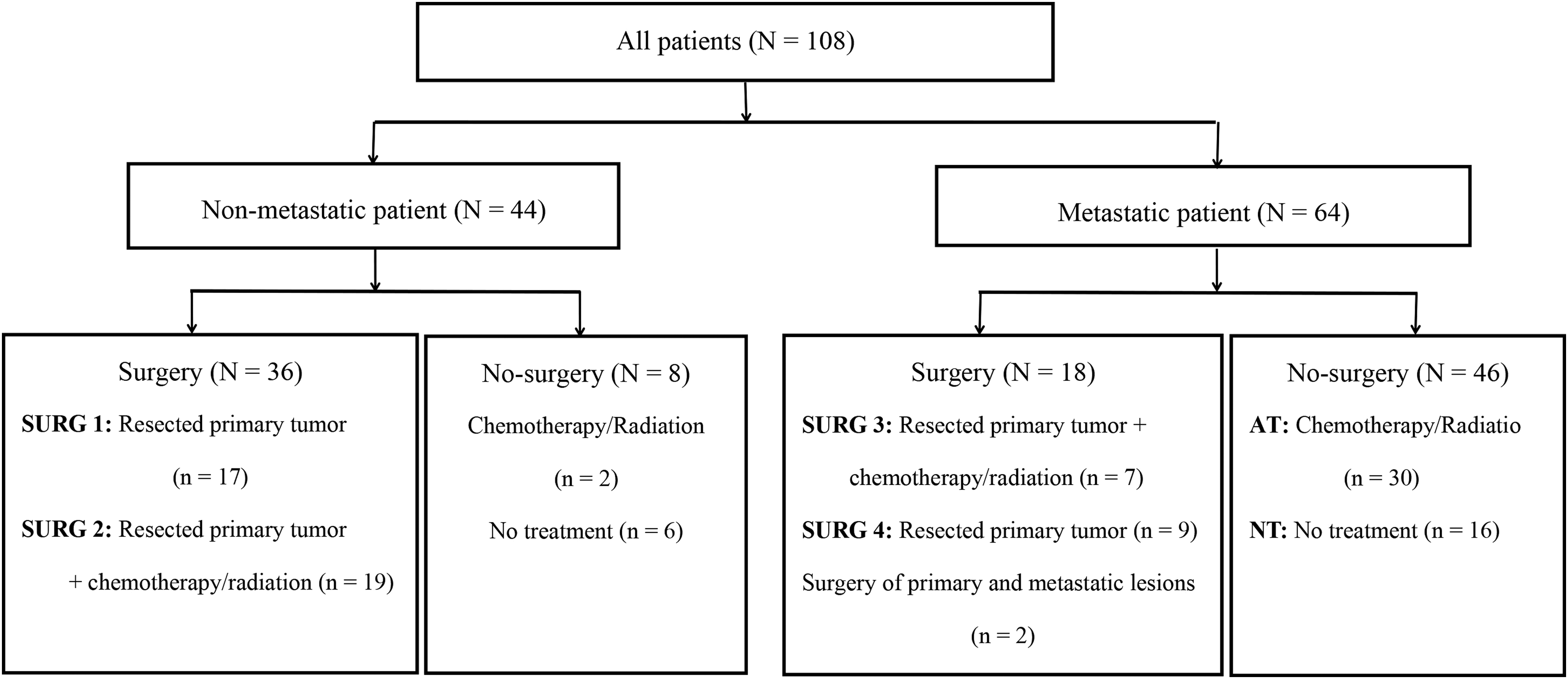
Flowchart of the patients who received different treatment options in the study. AT, adjuvant therapy; NT, no treatment.
In metastatic patients, 7 (11%) underwent surgery of the primary tumor and adjuvant therapy (SURG 3), 9 (14%) received surgery of the primary tumor alone (SURG 4), 2 (3.1%) underwent surgery of the primary and metastatic lesions, 30 (46.9%) received AT alone, and 16 (25%) patients had NT.
Survival outcomes
In the entire cohort, 91 (84.3%) patients died of this disease during the follow-up period. Of the 17 patients who survived, 10 were from nonmetastatic patients and 7 from metastatic patients. The median overall survival (OS) for all individuals was 10 months (95% CI: 8.455–11.545; Fig. 3).

Kaplan–Meier analysis of entire population. Color images are available online.
We compared the effect of whether or not the presence of a metastatic lesion on survival for patients and thus we found that nonmetastatic patients had significantly better survival time than the metastatic patients (19 [95% CI: 12.560–25.440] months versus 8 [95% CI: 6.575–9.425] months, P = .006; Fig. 4).
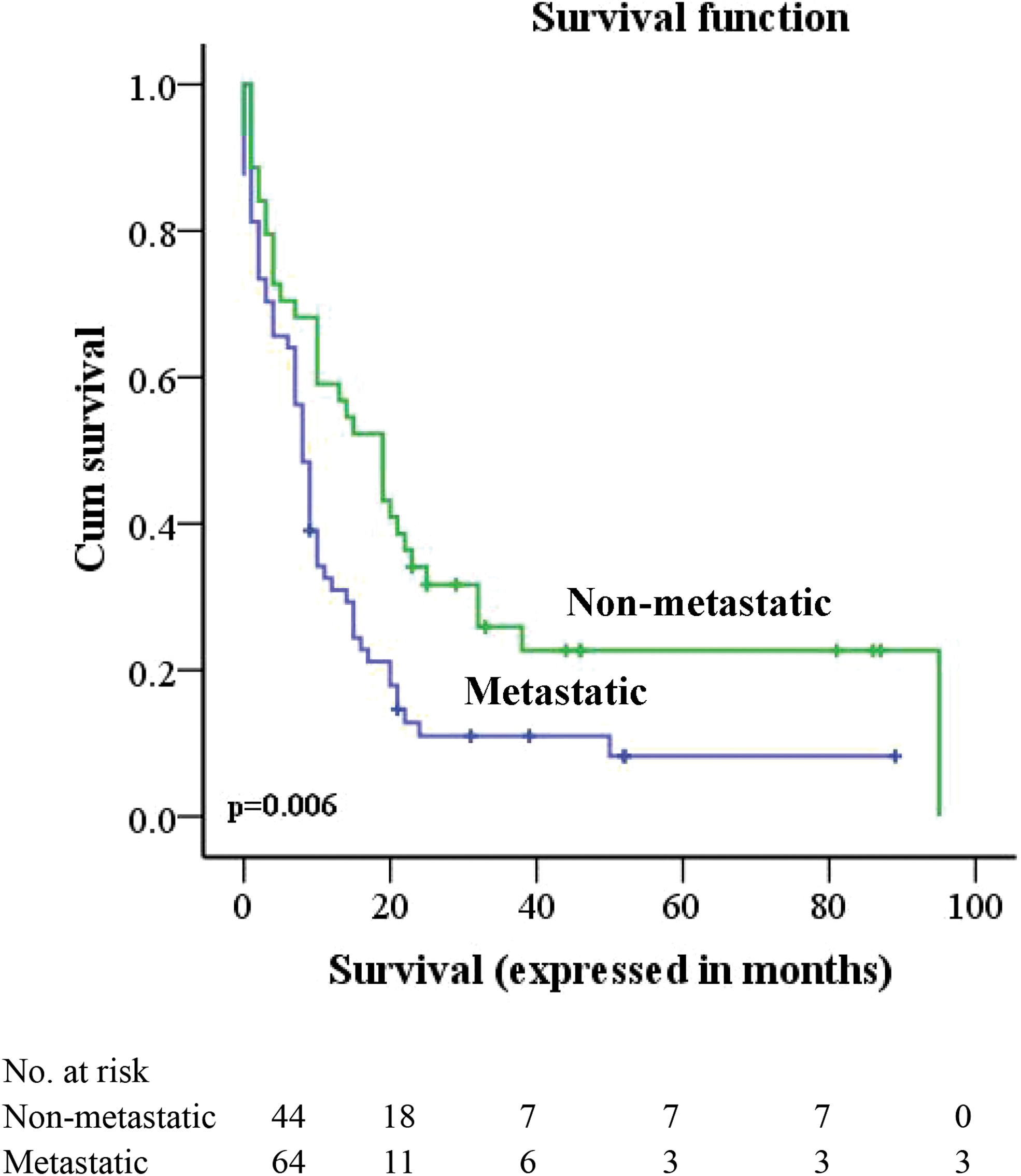
Kaplan–Meier analysis of metastatic and nonmetastatic patients. Color images are available online.
After straying nonmetastatic patients according to the treatment option, the median OS was 32 (7.142–56.858) months for SURG 1, 19 (11.970–26.030) months for SURG 2, and 1 (0–2.342) month for No-surgery (SURG 1 versus No-surgery, P = .001; SURG 2 versus No-surgery, P = .017; Fig. 5). However, the use of adjuvant therapy did not offer any survival benefit in comparison with patients undergoing only surgical resection (SURG 1 versus SURG 2, P = .234).
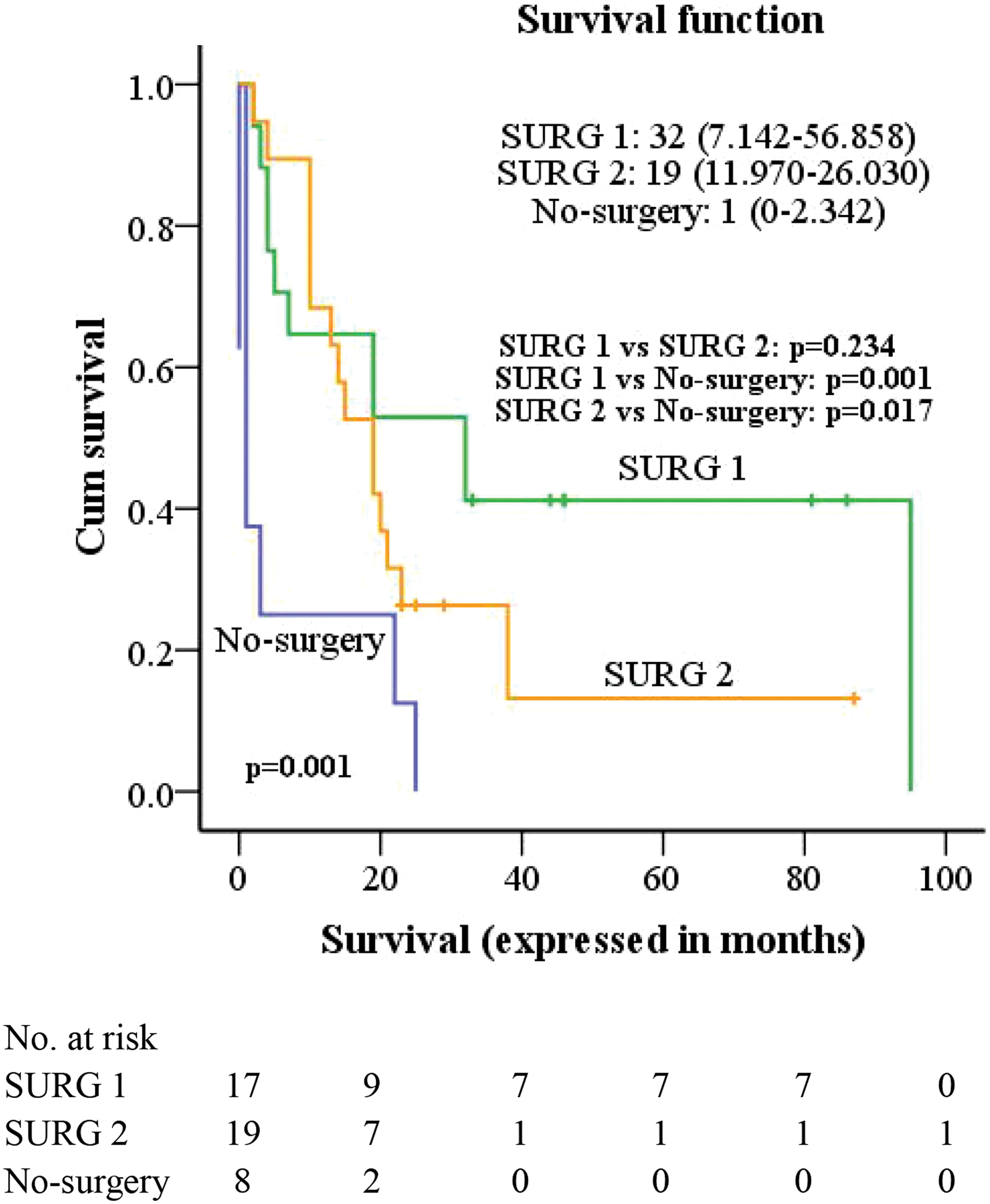
Kaplan–Meier analysis of nonmetastatic patients according to different treatment options. SURG 1: surgery of the primary tumor alone; SURG 2: surgery of the primary tumor and adjuvant therapy; No-surgery: AT alone and NT. AT, adjuvant therapy; NT, no treatment. Color images are available online.
For metastatic patients, the median OS was 14 (4.974–23.026) months for SURG 3+SURG 4, 9 (7.482–10.518) months for AT, and 1 (0–4.920) month for NT (SURG 3+SURG 4 versus AT: P = .010, SURG 3+SURG 4 versus NT: P = .002; Fig. 6). In addition, 2 patients who underwent surgery of the primary and metastatic lesions survived for 31 and 89 months, respectively. We also compared the subgroups of the surgery group, showing that the median OS was 17 months for SURG 3, whereas the median OS was 8 months for SURG 4. However, this difference did not reach statistical significance (P = .405).
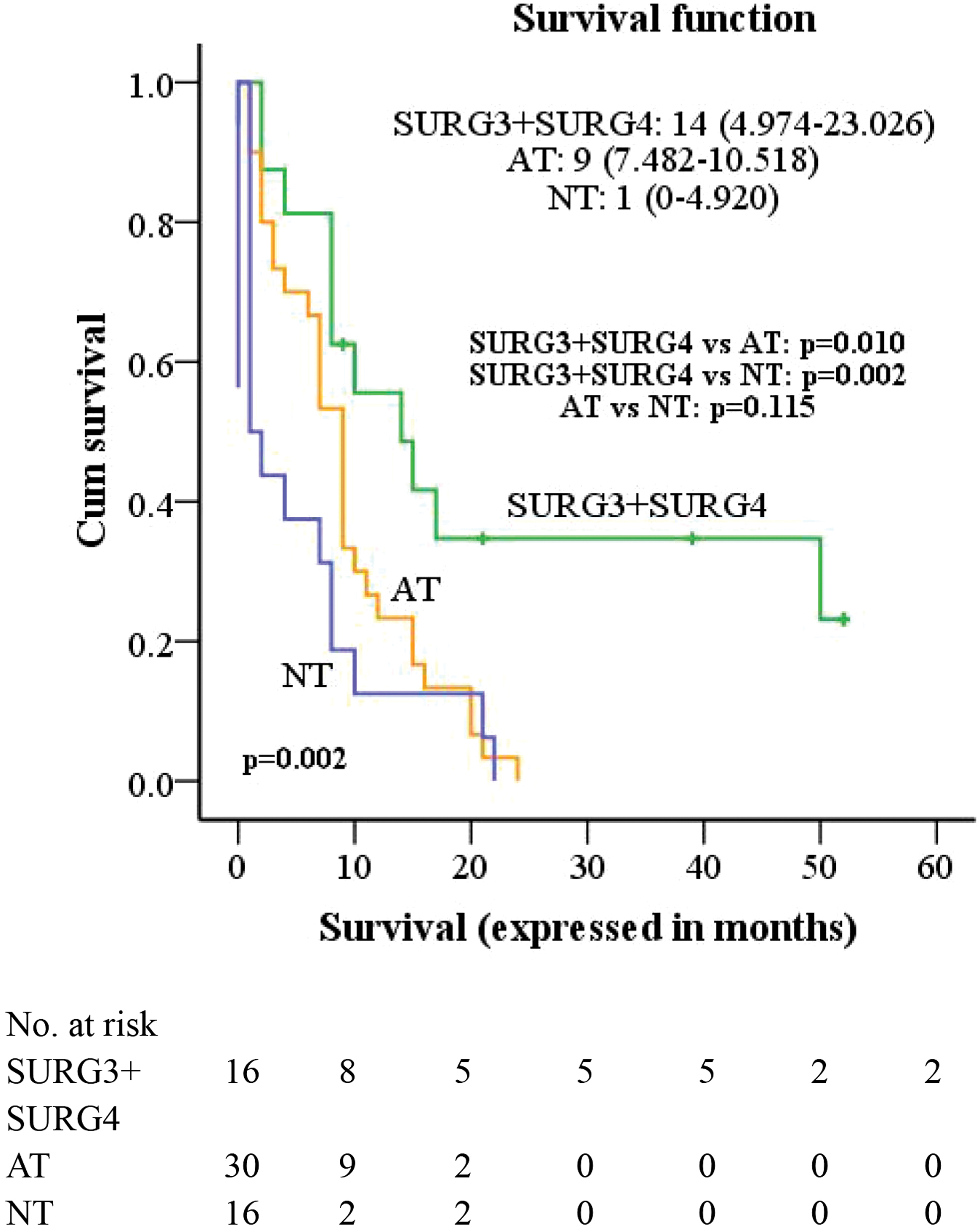
Kaplan–Meier analysis of metastatic patients according to different treatment options. SURG 3: surgery of the primary tumor and adjuvant therapy; SURG 4: surgery of the primary tumor alone. AT, adjuvant therapy; NT, no treatment. Color images are available online.
Multivariable Cox regression models
As presented in Table 2, the surgery of the primary tumor was an independent factor for improved survival.
Significant Predictors of Overall Survival by Cox Proportional Hazards Model
Note: Two patients who underwent primary and metastatic surgery were excluded from the analysis.
SEER, Surveillance, Epidemiology, and End Result.
Discussion
To the best of our knowledge, this is the largest study currently reported on the curative options and outcomes of hepatopancreatobiliary and ampulla LCNEC. Based on the SEER database, and finally, we included 108 patients for analysis. One finding is that the most common primary site was the pancreas, followed by the gallbladder, ampulla, and liver. The prevalence of LCNEC primary sites remained concordant with that reported in previous literature.9,10 Furthermore, patients with a primary pancreatic tumor are more likely to develop into metastatic disease, and may thus have fewer opportunities to undergo radical surgical resection. In the year of diagnosis from 2010 to 2015, 48 patients presented with distant metastases, and the liver (35/48) was the most common metastatic lesion. This finding is consistent with the already reported data.4,6,7 At the initial diagnosis, the liver tumor was significantly larger than other primary lesions. This discrepancy may be because liver LCNEC can grow to a larger size asymptomatically, whereas pancreatobiliary LCNEC may cause obstructive symptoms when the tumor is small.4,6
The management strategy and prognosis of patients are closely related to the tumor stage. As expected, the median OS of nonmetastatic patients was better than that of metastatic patients in our study. Theoretically, radical surgical resection is the most effective treatment for the localized solid tumors and contributes to the long-term survival of patients, which may also be the case in LCNEC. Beggs et al. reviewed 20 patients with ampulla LCNEC who underwent pancreaticoduodenectomy, and the mean survival was 11.8 months. 6 Raiker and his colleagues performed a review of published literature on biliary tract LCNECs in 2019, including 12 patients, 7 of whom underwent surgical resection with a median survival of 12 months (21 days–69 months). 4 Similarly, several small sample studies support radical resection as the preferred treatment for primary hepatic or pancreatic LCNEC and provide the most favorable outcomes like long-term survival.8,11,12 In this study, nonmetastatic patients who received surgery of primary tumor alone or surgery of primary tumor plus adjuvant therapy had better survival outcomes than nonsurgical patients. Interestingly, the use of adjuvant therapy did not offer any survival benefit in comparison with patients undergoing only surgical resection. Previous articles have shown that tumor morphology and the Ki-67 index play a crucial role in chemotherapy response and patient survival.13,14 Poorly differentiated NENs respond to cisplatin in >50% of patients against <15% for well-differentiated individuals, but the former has a worse survival outcome than the latter. 13 In this study, most of the nonmetastatic patients who received surgical treatment were poorly differentiated tumors, and the proportion of SURG 1 and SURG 2 was comparable, so we consider that tumor morphology has little impact on survival. In contrast, patients with Ki-67 ≥ 55% had a higher response rate to platinum-based treatment (42% versus 15%) but worse survival than patients with Ki-67 < 55% (10 versus 14 months). 15 This is a significant disadvantage of our study because there was no report on the Ki-67 index in SEER, which may lead to the selection bias that we cannot control. Data on pancreas and gallbladder NEC have suggested that most patients have a Ki-67 index ≥55%,16–18 and these patients were more likely to receive adjuvant chemotherapy in the setting of better chemotherapy response rates. 18 This may explain why the additional chemotherapy after surgery in our study did not bring survival benefits. Similarly, in a multicenter study conducted by Merola et al., the authors included 60 resectable high-grade gastroenteropancreatic NEN and NEC patients and found that median OS after radical surgery with and without adjuvant chemotherapy was comparable. 19 However, patients receiving radical surgery and adjuvant treatment had a higher Ki-67 value. Therefore, further researches are needed to identify the highly selected subset of nonmetastatic patients who may benefit from additional adjuvant chemotherapy after radical surgical resection.
At present, international guidelines indicate that chemotherapy is the standard treatment for metastatic NEC patients, and the first-line therapy regimen is cisplatin/carboplatin plus etoposide.20,21 In this study, nearly half of the metastatic patients received AT alone, and the median OS was 9 months. On the contrary, the median survival time of metastatic patients without any treatment was only 1 month. This finding was following the study from Sorbye et al., 15 authors compared patients after palliative chemotherapy (n = 252) with patients treated with best supportive care only (n = 53) and found that their respective median survival was 11 and 1 month.
Considering the previous literature and this study, the liver is the most common metastatic site of LCNEC.4,6,7 Simultaneous resection of the primary tumor and the metastatic liver lesions is still the most effective way for patients to obtain long-term survival benefits. Galleberg et al. reported the outcomes of curatively intended resection/radiofrequency ablation in 32 patients with metastatic gastroenteropancreatic NECs (nonsmall cell: 78.1%), and the results showed that the median OS was 35.9 months with a 43% 5-year OS. 22 The benefits of survival are inspiring, but in clinical practice, only a small number of patients have an opportunity to undergo radical surgery because liver metastases are usually bilobar, numerous, and synchronous. 23 Once liver metastases are considered unresectable, patients may receive radiofrequency ablation, transcatheter arterial chemoembolization, or peptide receptor radionuclide therapy. 24 In addition, Frilling et al. also suggested that the primary tumor should be resected if possible. 24 In our study, the median OS of the metastatic patients with resection of the primary tumor was better than that of metastatic patients with AT alone or metastatic patients without any treatment. Furthermore, metastatic patients undergoing surgery of the primary tumor and adjuvant therapy had a trend of survival benefit over metastatic patients undergoing surgery of the primary tumor alone, but it did not reach statistical significance. Consistent with our results, Feng et al. collected data from metastatic pancreatic NEC patients registered in the SEER database from 1988 to 2014 and concluded that surgical resection of the primary lesion could significantly prolong the survival of those patients. 25
Several limitations exist in this study. First, the number of patients included in our cohort was less than the actual number due to the missing information in the database. Despite that, this is the largest series to exhibit the treatment options and outcomes of LCNEC at present. Second, this is a retrospective study in design, which may lead to inherent selection bias regarding who received certain modalities (resection, systemic therapy, etc…). Third, it is an inability to gain information on chemotherapy regimens (agents, doses, or timing), surgery type, and to obtain some related to the prognosis factors such as Ki-67 index and surgical margin status, making it impossible for further analysis. Nevertheless, we had shown the survival trend of a rare disease in different treatments. Also we found that a considerable number of patients after surgical resection survived for a long time despite this disease with a poor OS.
In summary, the prognosis of patients with hepatopancreatobiliary and ampulla LCNEC is dismal, with a median OS of 10 months. Radical resection is the first choice for resectable tumors, whereas surgical resection of the primary tumor plus adjuvant therapy might represent a valid option for metastatic disease. However, further studies are needed to confirm this.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.