
Abstract
Introduction:
Roux-en-Y gastric bypass (RYGB) remains among the most widely performed bariatric procedures. A significant decline in its indication has been observed due to weight regain and reappearance of comorbidities. Moreover, the lack of effective therapeutic alternatives after failure justifies why other techniques are more frequently chosen. We present a novel technique to convert a failed RYGB into a one anastomosis gastric bypass (OAGB).
Case Presentation:
A 43-year-old male patient with a body mass index (BMI) of 47 kg/m2 and several comorbidities was submitted to RYGB. Initially his surgery was successful, but after 7 years he visited the bariatric and metabolic surgery clinic with reappearance of all comorbidities, and the same BMI as before having bariatric surgery. After proper evaluation and preparation, conversion to OAGB was decided.
After anatomy identification, the alimentary limb was transected 20 cm distal to the gastrojejunal anastomosis, and a new anastomosis with the common channel (CC) was created, to form a new long afferent biliopancreatic limb and a new short efferent CC.
Results:
The surgical procedure and postoperative course were uneventful. One year after the procedure the patient's BMI was 36 kg/m2. He has been able to stop all medications and therapies related to previous comorbidities. To date, the patient has good dietary and supplementation adherence resulting in no nutritional deficiencies, or gastrointestinal symptoms.
Conclusion:
This new surgical technique is safe and feasible. Short-term results have shown reasonable weight loss (WL), and especially remission of comorbidities with an improved quality of life.
Introduction
Roux-en-Y gastric bypass (RYGB) is considered the gold standard in bariatric surgery, but paradoxically its indication suffered a considerable decline. The emergence of simpler surgical techniques such as sleeve gastrectomy or one anastomosis gastric bypass (OAGB) partially justify this tendency. Long-term weight regain (WR) and reappearance of comorbidities can occur in ∼30% of patients.1–4 Once this happens, effective therapeutic alternatives are seldom found5–11 and it could be RYGB most significant shortcoming.
Endoscopic and surgical modifications of a primary RYGB have been described with varying results. We present a novel technique to convert a RYGB failure into a OAGB.
Case Presentation
A 43-year-old male patient with a body mass index (BMI) of 47 kg/m2, a history of smoking and comorbidities, including type 2 diabetes, hypertension, obstructive sleep apnea syndrome, and nonalcoholic fatty liver disease, was submitted to RYGB in 2010 at another institution. During that time he had to be hospitalized on three occasions, one of which was secondary to marginal ulceration (MU). Patient's lowest BMI was 28 kg/m2 and remission or improvement of comorbidities was acceptable during the first two postoperative years, but with a clear tendency toward progressive WR thereafter. The trend was such that after 7 years his BMI was the same as before having bariatric surgery, and there was also complete reappearance of all comorbidities.
Possible causes of failure and MU such as gastro-gastric fistula, and pouch, or anastomotic enlargement were discarded before deciding surgical conversion by means of endoscopic and radiographic studies. After proper evaluation and preparation by our multidisciplinary team, the patient was scheduled for surgery. Our goal was to convert a mainly restrictive procedure such as standard RYGB 12 into a hypoabsorptive OAGB avoiding the modification of prior anastomosis or stapled tissues. Informed consent was obtained from all individual participants included in the study.
Surgical Procedure
The key steps of our procedure included (1) precise identification of RYGB anatomy with measurement and marking of each limb, (2) measurement of new common channel (CC) from ileocecal valve proximally, (3) creation of a new “pouch” with a jejunal segment, by transecting the alimentary limb 20 cm distal to the original gastrojejunal anastomosis, (4) communication (latero-lateral anastomosis) between new “pouch” and predesignated small bowel (SB) loop to form a new long afferent biliopancreatic (BP) limb and a new short efferent CC (Supplementary Video SV1).
The simplicity of the technique is that after RYGB anatomy has been properly identified, it only requires the creation of a new anastomosis. Transection of the Roux limb creates distance from previously dissected tissues reducing complications related to working in an operated area. It also reduces the chance of esophageal reflux, frequently found when a short pouch and a loop configuration are combined. Besides the fact that this is conversion and not primary surgery, the parameters considered to decide CC length include patient's BMI, age, presence of comorbidities, and SB hypertrophic changes (which are characteristic years after bariatric procedures). The CC length is shorter than the minimum used for primary OAGB.
Results
Final CC limb length was 160 cm (down from an original 290 cm). Original BP limb was 30 cm, and increased to a total of 300 cm (original BP limb [30 cm]+original Roux [alimentary] limb [160 cm]–new GJ “pouch” [20 cm]+aggregated bypassed limb [130 cm]) (Fig. 1). Operative time was 93 minutes and there were no complications. The postoperative course was uneventful. Indications regarding diet, supplementation, activities, and follow-up visits were the same as for primary OAGB. One year after the procedure, the patient's BMI was 36 kg/m2. This weight loss (WL) is in contrast to the results we obtain after primary OAGB and reflects difficulties in finding therapeutic alternatives after RYGB failure. In contrast, the patient has been able to stop all medications and therapies related to previous comorbidities. To date, the patient has good dietary and supplementation adherence resulting in no nutritional deficiencies, or gastrointestinal symptoms.
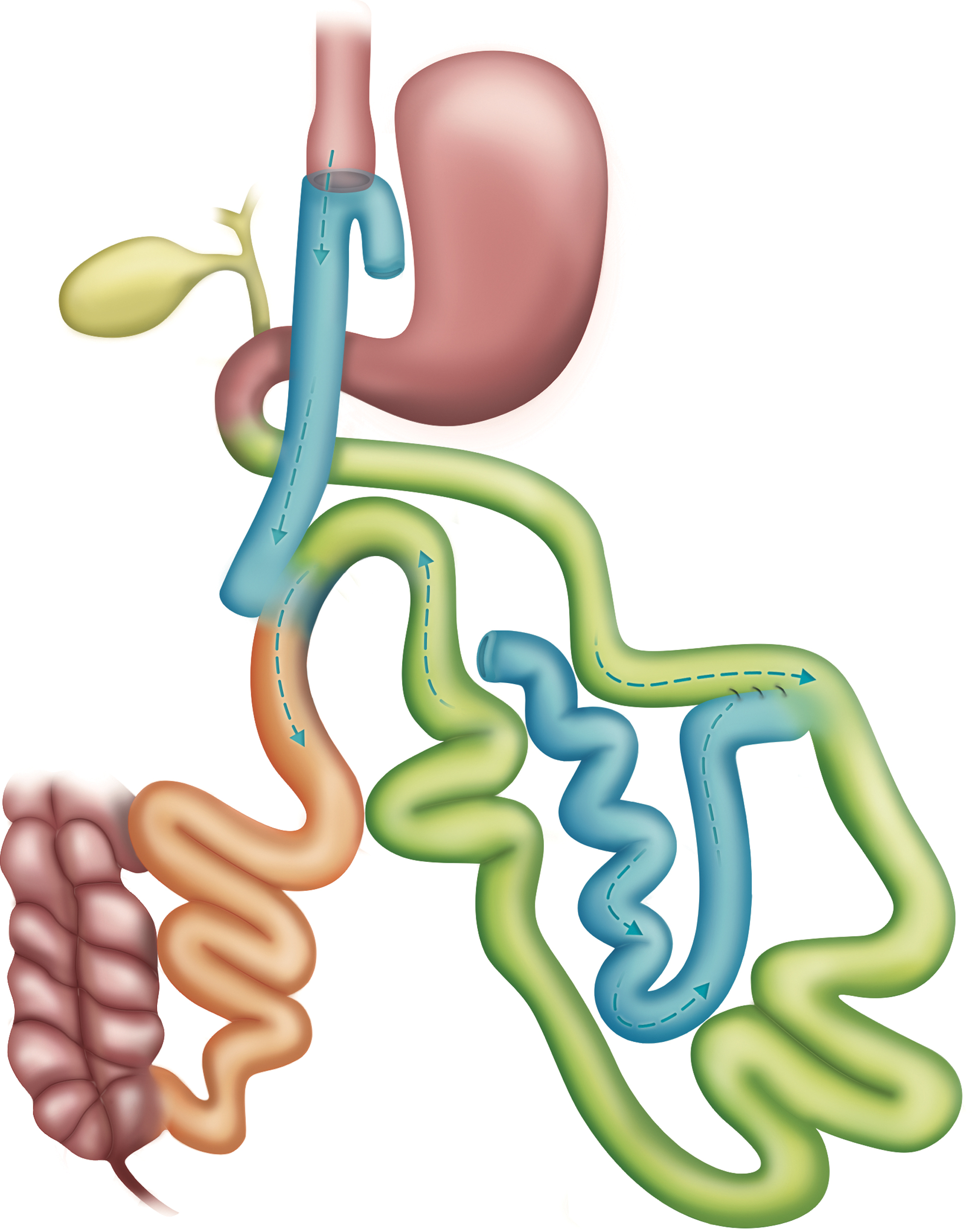
Surgical technique scheme. Color images are available online.
Discussion
There is currently a significant lack of Grade A recommendations about conversion techniques after RYGB. Before proceeding to revise or convert an RYGB, an MDT should evaluate nutritional, behavioral, and anatomical pitfalls that could justify failure of the primary operation. A commonly performed RYGB has standard measures with a 50 cm BPL and 150 cm Roux limb. The Roux limb has absorption capacity except for fat, making RYGB a mainly restrictive procedure. 12 So far, lengthening of BPL appears as the most efficient option after WR, but nutritional complications may arise.
The main goal of the technique described is to add a powerful hypoabsorptive effect while avoiding prior anastomosis or stapled tissues, to prevent unnecessary complications. The ratio between total bowel length/common limb is the most accurate parameter to predict a long-term postoperative BMI under 25 kg/m2. 13 This result is mostly secondary to a hypoabsorptive effect and the reason why a modification from RYGB restriction to OAGB hypoabsorption can be successful.
A loop configuration with a short pouch has been associated with GERD; therefore, it is reasonable to lengthen the pouch at the expense of jejunum. This conforms a low-pressure system with a large anastomosis such as primary OAGB, without the presence of exocrine secretions close to the esophagus.
The remaining Roux limb of 160 cm no longer serves a purpose, but it is not necessary to resect or reattach the SB. Any anastomosis performed in a patient can leak, even in very experienced hands. Besides, the removal of SB in obese patients can be a difficult and aggressive step that may lead to complications with higher morbidity, mortality, and prolongation of the surgical time. After sleeve gastrectomy with jejunal bypass (SGJB) in which the jejunum is abandoned and a jejunoileal anastomosis is performed, there is an absence of symptoms or histological alterations that would suggest that patients develop small intestinal bacterial overgrowth. 14
It is necessary to know the total bowel length when any hypoabsorptive technique is performed, especially in revisional surgery. At the time of choosing CC length, we take into account the patient characteristics, comorbidities, age, and intraoperative findings. In this young patient with such intestinal diameter, we selected 160 cm, which is the shortest CC we have used in revisional surgery. Besides limb length, the surface added by a larger intestinal circumference should be considered. It required more than one 60-mm cartridge to transect the SB. The most feared complications regarding hypoabsorptive procedures are nutritional deficiencies. During our initial experience we used fixed limb measures, but then changed to TBL/CC ratio. Two hundred twenty centimeters is the shortest CC we would recommend for primary surgery, and only in patients with BMI >50 kg/m2. 15 After 3600 primary OAGB we only had to convert 2 patients. 16 The intestinal adaptation and metabolic changes after failed primary bariatric surgery turn WL into something harder to achieve. After gastric bypass hyperplasia occurs, resulting in an increased SB diameter, higher villi, and deeper crypts.
By eliminating the Roux limb, lengthening the BPL, and shortening the CC in proportions that ensure an adequate nutritional status, we could obtain the best possible results. After 1 year of follow-up there was less weight loss than we expected, but full comorbidities resolution. With the patient under strict supplementation, there are no significant deficiencies or gastrointestinal symptoms worth mentioning.
It is clear that anatomic, nutritional, and behavioral causes of WL failure or WR after gastric bypass need to be corrected before conversion. In contrast, controversy exists in the area of choice of revisional intervention. We propose the conversion from RYGB to OAGB based on the advantage of adding a powerful hypoabsorptive effect while avoiding the modification of prior anastomosis or stapled tissues.
Conclusion
Long-term failure of RYGB is not infrequent. Adaptation makes successful therapeutic options difficult to find. Conversion of a standard RYGB to OAGB using previously “untouched” tissues proved to be simple and safe. Short-term results have shown reasonable WL, and especially remission of comorbidities and an improved quality of life.
Footnotes
Authors' Contributions
Writing, original draft by L.A. Conceptualization, review, and editing by J.A.P.-S. and M.Á.C. Review and editing by H.A.Q. and E.L.-d.-L.
Disclosure Statement
No competing financial interests exist. The authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.