
Abstract
Background:
The planning of revisional bariatric surgery is a complex process. The availability of accurate anatomical information is especially important for the planning of such challenging surgical procedures, we present our initial experience using three-dimensional-computed tomography (3D-CT) images to preoperatively assess the anatomy of patients before bariatric revisional surgery.
Methods:
We used 3D reconstructed images of CT scans to assess the anatomy and plan revisional surgery in 144 patients 98 of them had a previous sleeve gastrectomy 41 had a previous gastric by-pass and 4 Vertical banded gastroplasties. An effervescent preparation was used to distend the stomach and the proximal bowel allowing volume estimation.
Results:
Eleven sleeve patients underwent a re-sleeve gastrectomy and 44 were revised to a “Roux-en-Y” gastric bypass (RYGBP). Forty-two patients with a previous gastric by-pass were revised due to weight regain or other issues and 4 patients with previous vertical banded gastroplasty (VBGP) were revised to RYGBP. 3D-CT scans provided valuable information for the planning of all revisional procedures by offering accurate information about the existing anatomy and measures of the volume of the gastric pouch, the size of the gastro-jejunal anastomosis in gastric by-pass cases, or the volume and shape of the gastric tube in gastric sleeve cases.
Conclusion:
3D-CT is a fast, widely available, reliable, and accurate tool to assess the anatomy after bariatric procedures. This noninvasive method can be particularly useful for the evaluation of postbariatric patients with failures, suboptimal results, and complications, and for the planning of revisional surgery.
Background
The planning of revisional bariatric surgery is a complex process, and the decision-making process, in general, is based in scarce anatomical information, mainly provided by endoscopic and/or conventional radiological studies with biplanar images that provide limited, and often inaccurate, definition of the anatomy. The use of high-quality three-dimensional (3D) reconstruction images of computed axial tomography (CAT) scans may provide valuable information for the planning of revisional bariatric surgery by offering accurate information about the existing anatomy and measures of the volume of the gastric pouch, the size of the gastro-jejunal (G-J) anastomosis in gastric by-pass cases, or the volume and shape of the gastric tube (rotations, strictures dilations, or fundus presence) in gastric sleeve cases.
Materials and Methods
From January 2009 to May 2021, we performed CAT scans with 3D reconstruction to 144 patients with history of bariatric procedures. Ninety-eight patients had a previous sleeve gastrectomy (55 with weight regain or <50% of excess weight loss, and 47 with severe gastroesophageal reflux disease (GERD), obstructive symptoms, poor tolerance to oral food intake or paraesophageal herniation of the sleeve).
Out of the 55 people with weight regain, 11 (20%) underwent a re-sleeve gastrectomy and 44 were revised to a “Roux-en-Y” gastric bypass (RYGB) (80%). Thirty-eight patients with a previous gastric by-pass had weight regain, two had acid gastroesophageal reflux, one had a gastro-gastric fistula and weight regain as well, and another had a big hiatal hernia (part of the gastric pouch herniated into the chest) and a stricture of the G-J anastomosis. Four patients had a previous vertical-banded gastroplasty (two with weight regain and two with severe GERD).
Before the CAT scan, all patients had, at least, 4 hours of fasting period. They were given a dose (1 packet—4 g) of E-Z Gas II (effervescent sodium bicarbonate granule packets E-Z-EM Canada Inc. (a Canadian Company dedicated to the GI Tract imaging) diluted in 5 mL of water. The patients were sitting during the liquid intake and, after swallowing the liquid, they were instructed not to bloat and were immediately asked to lie flat on the table. The helical CAT scan images were acquired using a PHILIPS TOMOSCAN 64, a CT GE REVOLUTION MAXIMA LITE, or a PET-CT GE DISCOVERY scanner and reconstructed in the workstation of each system.
In all gastric by-pass patients, the gastric pouch was partially resected in block with the G-J anastomosis, calibrating and reshaping the pouch by trimming it over a 36 Fr bougie, and a new G-J anastomosis was done. In 6 patients, the length of the biliary limb was also increased and in 1 patient with gastro-gastric fistula, the fistula itself and part of the distal stomach was also resected.
The protocol was reviewed and approved, by the Instituto Medico La Floresta (Caracas Venezuela) “Institutional Review Board” (IRB), ethics commitee and review Commitees of both institutions.
This research complies with World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects (2013). The article has been prepared in accordance with the Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals (ICMJE Recommendations).
Results
Sleeve patients with weight regain, or failure, had an average body mass index (BMI) of 39.7 kg/m2 (36–44), and those with severe GERD, or other conditions, had an average BMI of 29 kg/m2 (26–32).
Surgical time for re-sleeve procedures was 68 minutes (48–76), and 142 minutes for sleeve to RYGBP (118–164).
Average BMI of patients with previous RYGBP was of 44.7 kg/m2 (31–49).
Surgical time for by-pass revisions was 159 minutes (127–178), and, for vertical banded gastroplasties, 129 minutes (110–152).
One patient (sleeve to RYGBP revision) required reoperation due to persistent bleeding at the jejunum-jejunal anastomosis. No leaks or other complications were observed after revisional procedures, no 30 days readmissions were documented, and no mortality occurred.
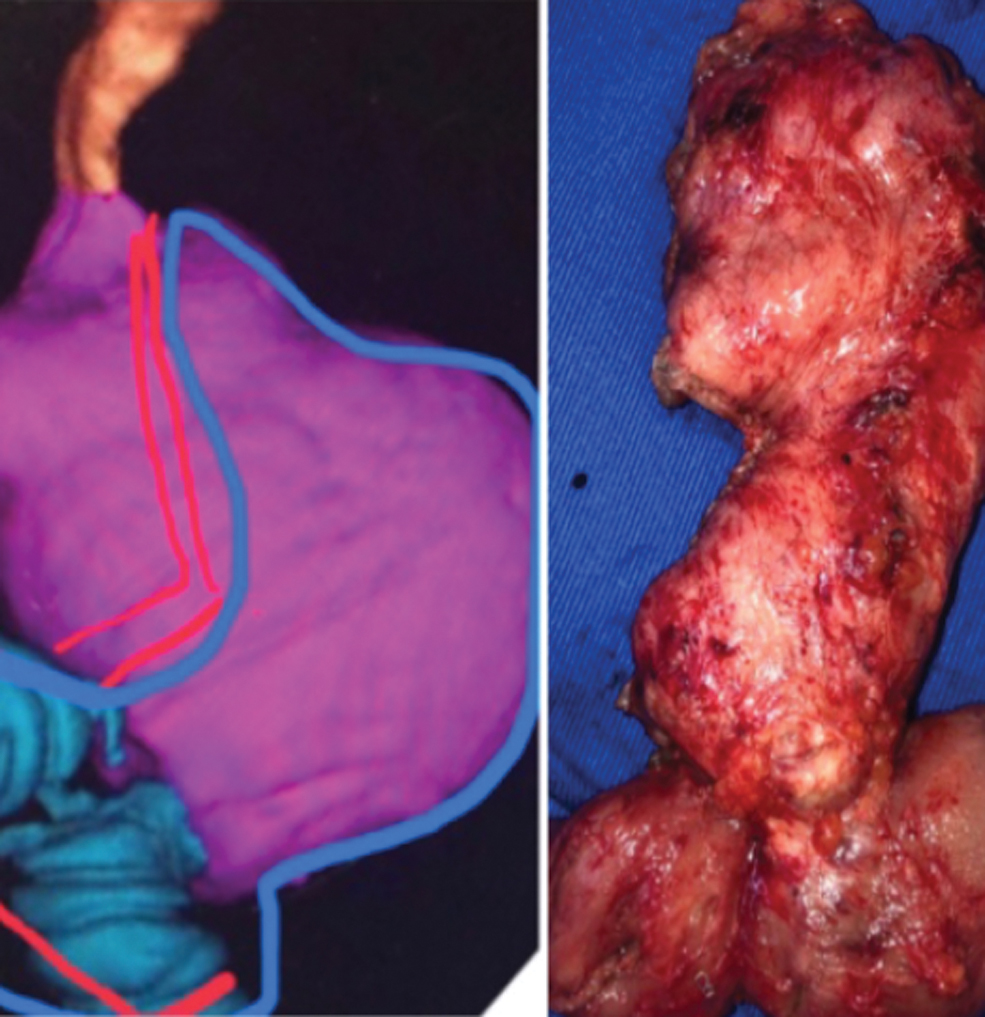
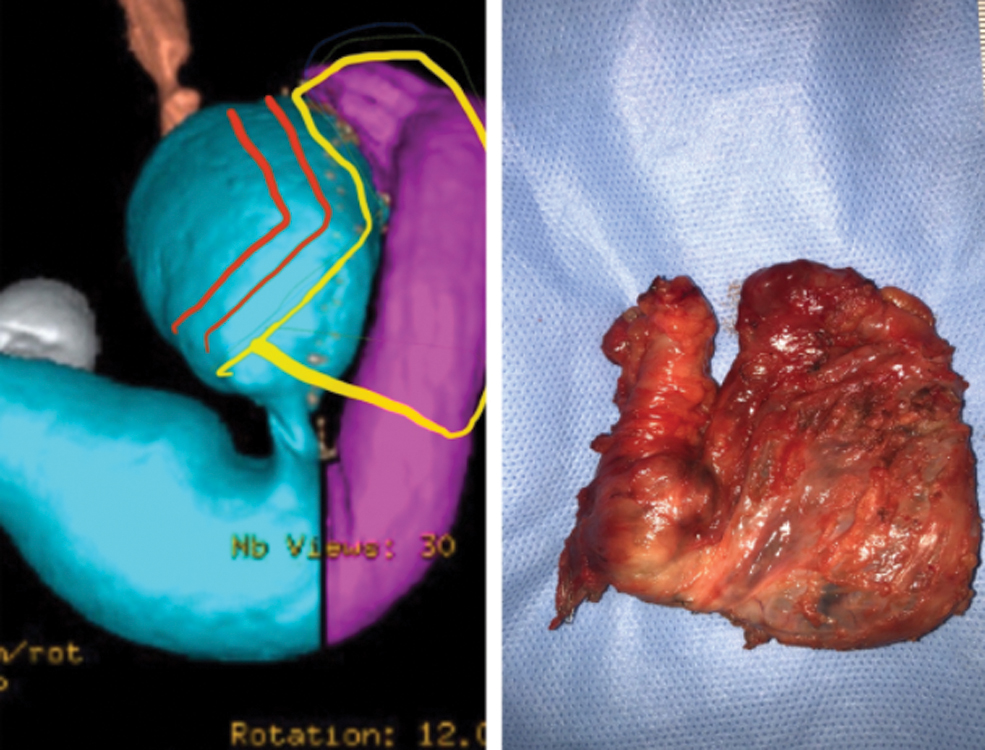
CAT scan with 3D reconstruction was especially useful in the planning of revisional surgery in all the revised cases. The surgical findings were identical to the anatomic shape shown in the scans. 3D reconstruction accurately estimated the volume of the gastric remnant after sleeve gastrectomy, showing the shape of the gastric tube, and the direction of the staple line, allowing us to see the length of strictures, twisting of the sleeve, fundus presence (Figs. 1–3) migration to the thorax (Fig. 4) or other shape distortions (Fig. 3).

Typical sleeve gastrectomy. Color images are available online.
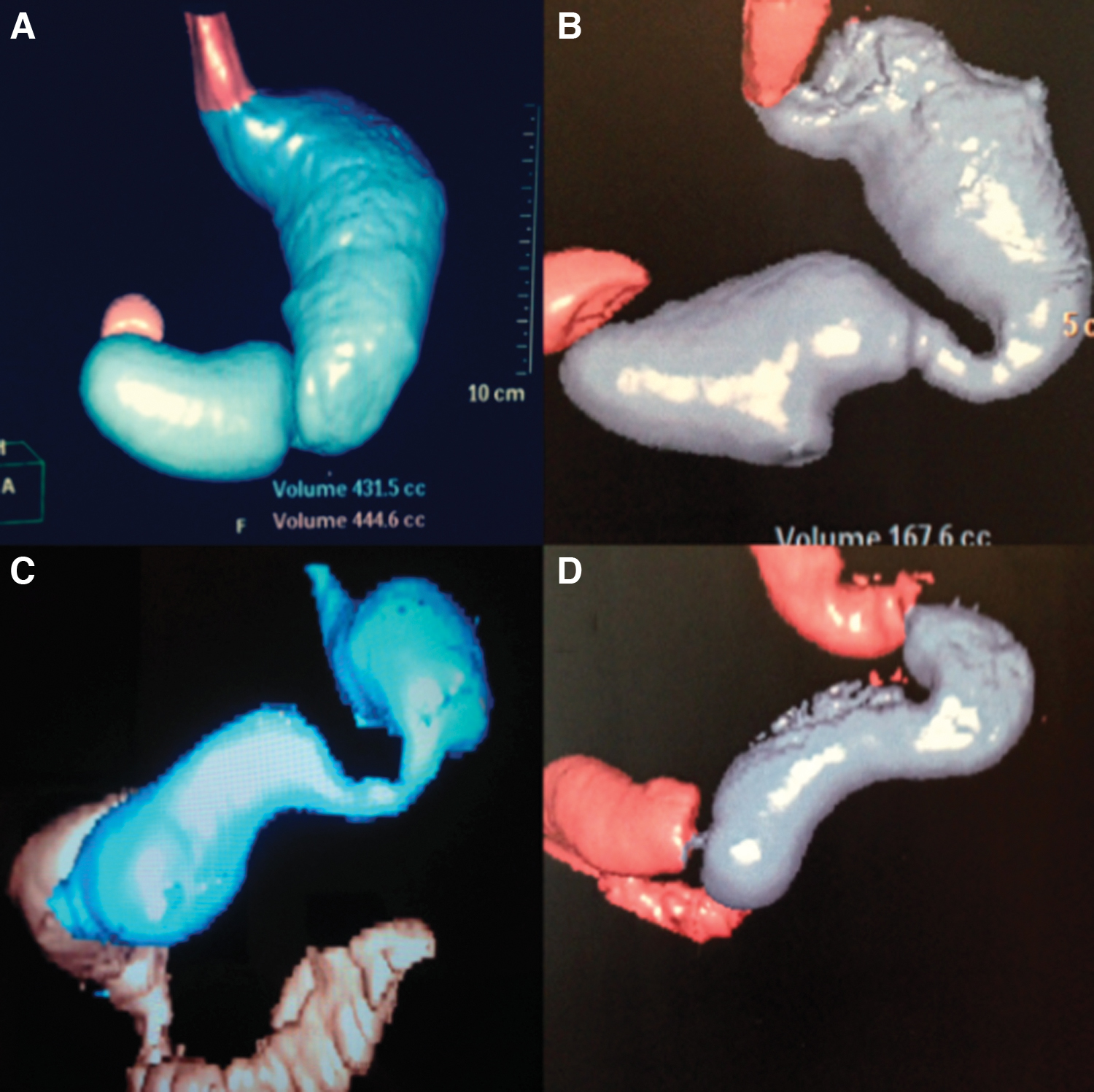
Different sleeve shapes:

Sleeve to RYGBP planning (big fundus remnant and distal stricture, weight regain and GERD). Red lines (projected transection. Blue lines planned resection). GERD, gastroesophageal reflux disease; RYGBP, “Roux-en-Y” gastric bypass. Color images are available online.

Type III paraesophageal hernia with sleeve completely herniated to the mediastinum. Color images are available online.
3D reconstruction allowed us to accurately estimate the volume of the gastric pouch (Fig. 5) and the size of the G-J anastomosis after gastric by-pass and allowed to plan if a pouch remodeling, anastomosis resection, or other procedures were necessary (Fig. 6).

Typical RYGBP. RYGBP, “Roux-en-Y” gastric bypass. Color images are available online.
RYGBP Revision planning: Red lines: Projected transection. Blue lines planned resection. RYGBP, “Roux-en-Y” gastric bypass. Color images are available online.
The scans did not provide information about the length of alimentary, biliopancreatic, or common limbs after gastric by-pass.
The total costs of the 3D-CT in our institution were the equivalent to U$ 560 for May 2021.
Discussion
3D tomographic images provide accurate and detailed information about the anatomy after bariatric procedures.1–3 This information is valuable to indicate and plan revisional procedures that are often complex. One of the potential benefits of 3D-CT is being able to estimate the volume of the stomach after sleeve gastrectomy,2–6 (Fig. 1) or of the gastric pouch after gastric by-pass.7–9 (Fig. 5) The size of the G-J anastomosis can also be assessed in derivative procedures.
Several authors have demonstrated a close correlation between 3D-CT estimated gastric volume and weight regain after sleeve gastrectomy,8,9 which is not uncommon. The objective and accurate volume estimation and the assessment of the gastric tube shape, the presence of torsions or strictures of the sleeve, or migration to the chest, the clear description of the implanted devices, such as bands or restrictive rings (Fig. 7), and their precise anatomical position, can be a crucial factor for the decision-making process before revisional surgery after sleeve gastrectomy and other bariatric procedures.

Adjustable gastric band in addition to a gastric sleeve. Color images are available online.
3D-CT is also particularly useful to assess the actual anatomy after almost every type of bariatric surgery (Fig. 8), but it does not provide information about the length of biliary or alimentary limbs in derivative operations.
Vertical banded gastroplasty provisional surgery planning (GERD and weight regain). Red lines planned transection, Blue lines tissue to be resected. GERD, gastroesophageal reflux disease. Color images are available online.
It is extremely important to standardize the protocol for patient preparation and image management to allow a reliable comparability of previous and future 3-CT examinations.
3D-CT also allows the diagnosis of long-term complications such as sleeve strictures, torsion, or thoracic migration that in some cases can be a complete paraesophageal hernia10,11 (Fig. 8); some of these complications may not always be evident during upper endoscopy. Thus, 3D-CT imaging is a valuable complementary resource that provides important information about functional anatomy after bariatric surgery.
Endoscopic studies performed by experienced bariatric endoscopists might also show or suggest the presence of these issues, but 3D-CT shows the anatomy as objective images that can be repeatedly reviewed and discussed by all members of the multidisciplinary bariatric surgery team.
The optimal volume of a gastric remnant after sleeve gastrectomy has not been established yet, but a previous publication of our group established a close correlation between gastric volume 6 months after sleeve gastrectomy and excess weight loss. 4 Other authors have reported a link between high sleeve volumes and weight regain.5,6 Therefore, an extended well-standardized protocol could become a reliable quality-assessment tool, useful for predicting results in terms of excess weight loss or odds for weight regain.
The inability of 3D-CT to assess the length of bowel loops after derivative procedures, such as RYGB, One Anastomosis Gastric Bypass (OAGB), Duodenal Switch (DS) and others, limits the possibility of using it as a single predictor of success or as an overall quality-assessment tool for these operations due to the many other factors involved, but this tool can be of important relevance for the diagnosis of other issues, as pouch and G-J anastomosis enlargement, gastro-gastric fistulas, or pouch migration to the chest.1,9,12
Conclusion
3D-CT is a fast, widely available, reliable, and accurate tool to assess the anatomy after bariatric procedures. This noninvasive method is gaining acceptance for the evaluation of postbariatric patients with failures, suboptimal results, and complications. 3D-CT could provide valuable and accurate information about the actual anatomy for the planning of revisional bariatric procedures and could be an extraordinary addition to the information provided by endoscopic studies in patients with postsurgical complications or poor results after bariatric surgery.
Footnotes
Authors' Contributions
Conception, design, patient recruitment, surgical procedures, and data analysis by A.H. Image processing and interpretation, and patient recruitment by D.J.S. Data collection and analysis by D.A.H. and R.A.H.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.