
Abstract
Background:
Rectal cancer is a common malignant tumor in the gastrointestinal tract. This work compares the effects of transumbilical laparoscopic surgery (TULS) and laparoscopic-assisted surgery on the anus-preserving effect of low/ultralow rectal cancer.
Materials and Methods:
Eighty patients with rectal cancer admitted to our hospital from February 2011 to July 2016 were randomly selected and divided into the laparoscopic group and TULS group, 40 cases in each group, all underwent radical anorectal cancer radical surgery. Statistical analysis was performed on surgical-related indicators in the two groups.
Results:
Two patients converted to open surgery were excluded. Five patients were excluded because of radical abdomen perineal resection for rectal cancer. Six patients were converted to TULS from laparoscopic surgery. Sixty-seven patients in the experimental group successfully completed anus-sparing surgery, and none died during the operation. The compliance rate of the distance between the lower edge of the tumor and the incision edge of the specimen in the TULS group was better than that in the laparoscopic group (P < .05). There were no significant differences between the two groups in terms of surgical time, blood loss, number of lymph node dissections, functional time of voluntary defecation and postoperative complications, tumor-free recurrence rate at 3 years, and 3-year survival rate after surgery (P > .05).
Conclusions:
The TULS method is safe and feasible in low and ultralow rectal cancer surgery. It has more advantages than laparoscopic-assisted surgery for anus preservation.
Introduction
Rectal cancer is a common malignant tumor in the gastrointestinal tract. Clinically, rectal cancer with a lower edge of the tumor with 5–8 cm from the anal margin is usually referred as low rectal cancer, while rectal cancer less than 5 cm from the anal margin as ultralow rectal cancer. 1 Among the new patients with colorectal cancer in China, rectal cancer accounts for 60%, while low-grade and ultralow rectal cancer accounts for 70%–80% of the total rectal cancer. 2 Traditionally, rectal cancer with tumors located below the peritoneal reentry is often treated with radical perineal surgery, which brings incision pain, long indwelling urinary catheters, prolonged bed rest, high lung infection rate, loss of anal defecation function, and decreased quality of life of fistula after abdominal surgery. 3
With the advancement of tumor biology, it is widely believed that rectal cancer with less than 2 cm from the dentate line of the lower edge of the tumor is feasible for radical anus preservation. It was also found that the lower margin of greater than 2 cm can achieve negative specimen margin. 3 Neoadjuvant chemoradiotherapy before surgery can degrade the tumor, and reduce the positive rate of resection margin and local recurrence rate. It is conducive to anus preservation. Stapler can perform low-level anastomosis in a narrow pelvic cavity. Laparoscopic technology makes the operation field clear and more accurate, which allows anal sphincter control, and urination and sexual function to be preserved to the greatest extent after surgery. 4
The 5-year survival rate and disease-free survival rate of the laparoscopic group were slightly higher than those of the open group.5,6 However, it becomes increasingly difficult to expose when laparoscopic surgery enters a low-level separation, especially with distal tumor. The distance judgment of the lower edge of the tumor is still not accurate due to the lack of hand touch, even assisted by digital anal diagnosis during the operation.
As an alternative, hand-assisted laparoscopy can make up for these shortcomings to a certain extent, which could compensate for the abovementioned shortcomings and retain the advantages of laparoscopy to free the hand for surgery. 7 During the operation, the tactile sense of the hand and the flexibility of the hand are used to expose the rectum, which can better expose the surrounding space of the ultralow rectum and more fully free the distal rectum. Meanwhile, with the fine touch of the hand, the bowel to be resected at the lower edge of the tumor can be controlled more accurately. Anus-preserving surgery is more effective and reliable for patients with low/ultralow rectal cancer. 8
Transumbilical laparoscopic surgery (TULS) is a method that combines laparoscopy, hand assistance, and openness, which converts in one operation according to the needs of the operation. 9 In this work, we compare the effects of TULS and laparoscopic-assisted surgery on the anus-preserving effect of low/ultralow rectal cancer.
Materials and Methods
Patients
From February 2011 to July 2016, 80 patients with rectal cancer treated in The Second Hospital of Hebei Medical University were randomly divided into 2 groups, with 40 in the TULS group and 40 in the laparoscopic group. The inclusion criteria include the following. (1) Colonoscopy- and pathological examination-confirmed rectal cancer. (2) The distance between the lower edge of the tumor and the anal edge being less than 8 cm. (3) Patients with rectal cancer Tumor, Node, Metastasis (TNM) stage I–III. (4). Preoperative chest computed tomography (CT) plain scan, total abdominal plain scan and enhanced CT, pelvic plain scan, and enhanced CT examination showed no distant metastasis and surrounding tissue infiltration.
Exclusion criteria include the following. (1) Severe cardiopulmonary diseases and cachexia, intolerable surgery. (2) Combined with intestinal obstruction, intestinal perforation, or hemorrhagic emergency surgery. (3) Infiltration of distant tumors and surrounding tissues. (4). History of cancer. (5) History of abdominal surgery. There was no significant difference between the two in terms of preoperative indicators, including gender, age, and tumor pathological type and stage (P > .05, see Table 1).
Comparison of the General Situation of the Two Groups
TNM, Tumor, Node, Metastasis; TULS, transumbilical laparoscopic surgery.
After signing the informed consent for laparoscopic-assisted or TULS on Low/Ultralow Rectal Cancer for Anal Sphincter Preservation, the double-stapling technique was applied to complete the rectal and colon end-to-end anastomosis for those with the lower edge of the rectal mass less than 8 cm from the anal edge.
Preoperative preparation
The preoperative preparation was conducted according to the following procedures. (1) The first is routine examination, including blood, urine, stool routine, biochemical full, coagulation function, infectious disease detection, chest X-ray, electrocardiogram, cardiac color Doppler ultrasound, pulmonary function test, chest and abdominal pelvic CT examination, and colonoscopy. (2) The patients prepare skin, combine blood, take liquid food 3 days before surgery, take antibiotics orally, fast 8 hours before surgery, drink 2 hours before surgery, no antibiotics 30 minutes before surgery, and diarrhea and enema 1 day before surgery. (3) The patient agrees to the surgical treatment and signs the informed consent form. The clinical trial study was approved by the scientific Research Ethics Committee of the Second Hospital of Hebei Medical University, and the Clinical trial registration number is 2019-P044.
TULS laparoscopic low/ultralow rectal cancer radical surgery
The surgical procedure was consistent with the previous study. 9 The patient underwent general anesthesia with tracheal intubation. Lithotripsy position was taken after anesthesia, and routine disinfection and spreading were performed. We took a right umbilical incision, about 1 cm in length, and placed a 10 mm trocar, established a pneumoperitoneum, adjusted the pressure to 12 mmHg, placed a 5 mm trocar 3 cm above the pubic bone in the middle of the lower abdomen, and placed a 5 mm trocar as the auxiliary operation hole. A 12 mm trocar was the main operation hole, and a 5 mm trocar was disposed as a secondary operation hole on the upper 10 cm side of the head. A 10 mm trocar was placed as a secondary operation hole on the left Maison's point incision.
The abdominal cavity was inspected with a microscope and cut along the sigmoid colon. The posterior peritoneum converged down to the pelvic floor peritoneum reflex, and freed the rectum in the anterior intercondylar space to the level of the tailbone. We handled the sigmoid mesentery proximally to separate and protect the sigmoid vessels, ligated and severed the roots of the superior rectum vessels, and protected the lateral ureter. Ultrasound knife was continuously used to process the two sides of the rectal mesentery to the apical plane of the tailbone. Then, we stopped the pneumoperitoneum, removed the trocar from the umbilical incision, extended the incision upward and downward, and cut the left side of the abdomen wall.
For hand-assisted device, the left hand was an auxiliary hand to pull the rectum to expose the anterior rectal space. If necessary, the auxiliary hand was pulled at the lower edge of the tumor. The left auxiliary operation hole was the observation hole to enter the mirror. The auxiliary hand was used. The position of the lower edge of the tumor was determined by touch, and the rectum was freed 1–2 cm to the distal end again. The other handheld a laparoscopic cutting closure to break the rectum at 2 cm distal to the lower edge of the tumor. The pneumoperitoneum was lifted, and the specimen was raised from the hand-assisted incision. In addition, under the open operation, the sigmoid colon and its mesentery were separated at 10 cm from the upper edge of the tumor.
A 29 mm tubular stapler was inserted into the proximal end of the colon. After purging the anus, the 29 mm stapler handle was inserted into the anus after the anus was sterilized. The assistant assisted the end-to-end anastomosis of the sigmoid colon and rectum. We touched the anastomosis ring with the hand to record the distance from the anastomosis ring to the anal margin, and checked the anastomosis for patency and integrated. With no active bleeding in the abdominal cavity under the microscope, we checked the equipment and dressing, and placed a drainage tube in the pelvic cavity, leading from the right ventral trocar hole. Intraperitoneal injection of sodium hyaluronate was used to prevent intraperitoneal adhesions. The incision and trocar hole were closed layer by layer. The vital signs of the patient were stable during the operation, and the amount of bleeding was calculated.
Laparoscopic low/ultralow rectal cancer radical surgery
The patient was intubated under general anesthesia. After anesthesia, the lithotomy position was taken and routinely disinfected and spread. We did a 1 cm incision on the umbilical cord, pierced the pneumoperitoneum needle, established a pneumoperitoneum, adjusted the pressure to 12 mmHg, and inserted a 10 mm trocar as an observation hole. In the right lower abdomen, 12 and 5 mm trocars were, respectively, placed as operation holes. In the left lower abdomen, two 5 mm trocars were placed as auxiliary operation holes. No abnormalities were found in the abdomen. We lifted the sigmoid colon, cut from the sides of the sigmoid mesentery, and merged the peritoneum down to the pelvic floor before the peritoneum refolds to protect the ureter.
We freed the rectum along the anterior iliac space to the tip of the coccyx, and clipped and cut off the root of the superior rectum artery. We opened the peritoneal reflex, freed the rectum along the anterior rectal space to 2 cm from the lower edge of the tumor, and cut off the ligament tissue on both sides of the rectum. The small gauze strip was ligated under the rectal tumor, and the gauze strip was pulled proximally with endoscopic forceps. After revealing the gap, the rectum was cut off with a laparoscopic cutting closure 2 cm below the tumor with digital rectal diagnosis.
A longitudinal incision was made at the trocar puncture hole in the left lower abdomen, ∼5 cm long. We protected the incision, raised the specimen and sigmoid colon, cut off the sigmoid colon 10 cm above the tumor, and removed the specimen. A 29 mm tubular stapler was inserted into the proximal end of the colon and purse sutured, and then returned to the abdominal cavity. We sutured the incision and re-established the pneumoperitoneum. The assistant sterilized the anus and put the 29 mm stapler handle into the anus. The laparoscope connected the stapler head with the stapler handle to complete the colorectal end-to-end anastomosis. The assistant recorded the distance from the edge of the anus by touching the anastomosis ring with the anus by hand. We made sure that the anastomosis was unobstructed, and there was no active bleeding in the abdominal and pelvic cavity.
After checking the equipment and dressing correctly, we placed 2 drainage tubes in the pelvic cavity and led them out from both sides of the abdomen. Intraperitoneal injection of sodium hyaluronate prevents abdominal adhesions (Fig. 1).

Surgical procedure.
Postoperative treatment
The treatment included monitored vital sign, oxygen inhalation, parenteral nutrition support, observe incision, corrected the patient's anemia and hypoproteinemia etc. We removed the patient's catheter and encouraged them to get out of bed exercise as early as possible. The patient started to drink small amounts of water after venting. Next, we made the follow-up of 3 years after the operation, including digital rectal examination, abdominal pelvic CT, colonoscopy, blood Carcinoembryonic Antigen, and other tests to evaluate the effect of treatment.
Main observation indicators
The main observation indicators included the operation time, the amount of blood loss during operation, the number of lymph node dissections, the distance from the anal margin to the anastomosis ring, the distance from the tumor specimen to the incision margin, postoperative complications, postoperative voluntary defecation time, and follow-up observation of 3 years of survival.
Statistical processing
Statistical analysis was performed using SPSS21.0 software. The measurement data were expressed as x ± s. The t-test was used for comparison between groups. The chi-square test was used for counting data. Survival analysis was performed by the Kaplan-Meier method and the survival curve was drawn. P < .05 was considered statistically significant.
Results
Patients
The operation was successfully completed in both groups. Four patients were converted to laparotomy, 3 patients were converted to perineal combined with radical rectal cancer surgery, and the rest successfully completed anus-preserving surgery without death during operation.
Comparison between the two groups
The distance between the anal margin and the anastomotic ring in the TULS group was significantly shorter than that in the laparoscopic group, and the difference was significant (P < .05). The distance between the tumor edge and the incision edge in the TULS group was significantly longer than that in the laparoscopic group (P < .05). There was no significant difference between the two groups in terms of operation time, intraoperative blood loss, number of lymph node dissections, voluntary defecation time, postoperative complications, and tumor-free recurrence rate at 3 years (P > .05, shown in Table 2).
Comparison of Surgical Results Between the Two Groups
TULS, transumbilical laparoscopic surgery.
Complications and prognosis
Among the TULS laparoscopic group, there were 6 postoperative complications, including 1 case of incision infection, 1 case of pulmonary infection, 1 case of defecation incontinence, 2 cases of urinary retention, and 1 case of anastomotic fistula (cured by conservative treatment). There were 5 postoperative complications in the laparoscopic group, including 1 case of pulmonary infection, 1 case of defecation incontinence, 1 case of urinary retention, 1 case of anastomotic hemorrhage, and 1 case of anastomotic fistula (cured by secondary surgical transcolostomy), as shown in Table 3.
Comparison of Postoperative Complications Between the Two Groups
TULS, transumbilical laparoscopic surgery.
We defined the distance between the lower edge of the tumor and the upper incision as 1.5 cm, the compliance value, and found that the number of compliances in the TULS group was 34, and the compliance rate was 94.4% (P < .05). In the survival analysis, KM method showed that the three-year survival rate of TULS group was slightly higher than that of laparoscopy assisted group (P > .05, Fig. 2).
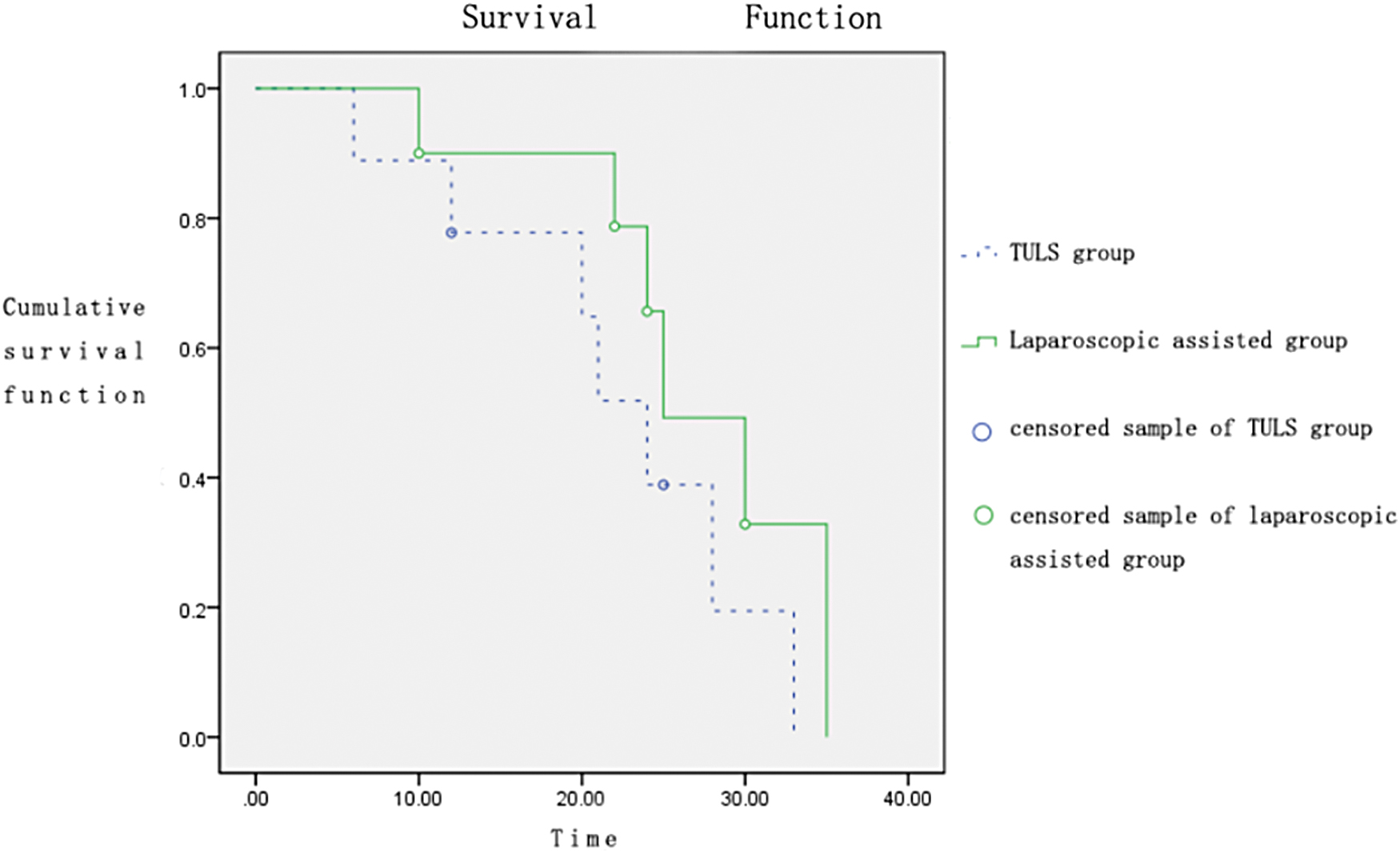
Survival curve of 3 years after surgery. Color images are available online.
Discussion
Rectal cancer has a high incidence in China, which is easy to be misdiagnosed. 10 Most patients have reached the advanced stage when they are found, and the number of ostomy patients has increased year by year. 11 With the accumulation of surgical experience of surgeons, endoscopic techniques have been well applied in anus-preserving surgery for low and ultralow rectal cancer, which reduces the trauma of the patient during surgery, and significantly improves the quality of life of the patient after surgery.
Hand-assisted laparoscopic surgery has the advantages of a short learning curve, hand-assisted pull exposure, and fine touch. However, it has the disadvantages of assisting the hand to affect the visual field and the device to clamp the assisting hand. Open surgery provides a guarantee for resection, with a history of pelvic surgery, large tumors, and possible metastases. 10 The purpose of the TULS method is to use the advantages of various methods to switch modes between each other in the same operation to better achieve a complete tumor cure and minimal trauma to the body. The anus-sparing operation of the distal bowel of the severed tumor has obvious advantages, especially in low and ultralow rectal cancer.
In TULS operation, laparoscopy is used to perform the previous exploration, which frees, disconnects the superior rectal blood vessels, and cleans the mesenteric root lymph nodes. 12 When entering the rectum low, especially the distal end of the tumor, it becomes more and more difficult. In this situation, hand-assisted laparoscopy is used in time. By touching the tumor boundary, the intestinal canal is directly pulled to expose the tissue space, and the surrounding tissues are further separated, and the lymph nodes are cleaned. Because the auxiliary hand has a large contact area with the bowel, the pulling is accurate, strong, and stable, which can better expose the surrounding space of the ultralow rectum and free the distal rectum more fully.
In addition, the fine touch of the hand can be used to affect the lower edge of the tumor. The quasicut line can be accurately controlled. In the occasional large-vessel bleeding during surgery, the assisting hand can quickly compress the bleeding site, effectively stop bleeding, and avoid conversion to open laparotomy. 13 After the severance, the proximal tumor was treated openly, which was fast and reliable.
For patients undergoing TULS, the laparoscopic instrument was used for pulling and the intestinal canal was further lifted after being dissociated with the auxiliary hand. 12 We found that the anal canal with scale was inserted through the anus, and the perspective line was measured. The laparoscopic group was 0.8 cm shorter on average than the TULS group. This 0.8 cm played a key role in meeting anus preservation and margin of the patient. There were 6 patients. It was difficult to perform the operation during laparoscopic lifting, and it was changed from the laparoscopic group to the TULS group.
We used the TULS method to convert the surgical method in a timely manner. Compared with the two groups of laparoscopic surgery alone, we found that TULS laparoscopic radical rectal cancer surgery had a short operation time and a high rate of compliance with the length of the inferior margin of the tumor. There was no significant difference in the time of voluntary defecation from the laparoscopic group. Tuls is effective in the treatment of rectal cancer with TNM stage I to III, the distance between the lower edge of the tumor and the anal edge is less than 8 cm and no metastasis and peripheral infiltration.
Most patients with rectal outlet obstruction present a concomitant pelviperineal dyssynergia. It should be adequately recognized and treated along with organic alterations or coexistent physiologic deficit. Retaining of external sphincter response to rectal distension and improving of conscious sensory threshold are important goals of treating defecatory disorders. 14 The Brusciano score used in this study seems to be a useful tool in selecting and assessing the outcome of patients who might benefit from rehabilitation treatment. Constipation and quality of life were significantly improved by the rehabilitation treatment.
It should also be considered whether the patients, before beginning the rehabilitative treatment, have reached an adequate selectivity of contraction or have acquired a correct knowledge of the anatomical and physiological notions. Probably, in the case of presence of muscular synergies without selective contraction of anal sphincter, a high percentage of the failed patients would have benefited in a previous electrostimulation treatment to acquire consciousness and sensitization of the patient to the anal area. 15
There were some limitations of this study. The situation of preoperative radiochemotherapy of the patients was not recorded. Further study with regular rehabilitation treatment was needed. The body mass index (BMI) of the patients was also not recorded. The correlation between BMI and the surgery needed further investigation. The statistical power was not calculated. The sample size of this study was relatively small. Further study with a larger sample size and multicenter was needed.
In terms of the distance from the anal margin to the anastomotic ring, the TULS laparoscopic group was significantly shorter than the laparoscopic group, suggesting that the TULS laparoscope can free the rectum further during the operation. It is more advantageous for low and ultralow rectal cancer surgery. The TULS method is safe and feasible in low and ultralow rectal cancer surgery. It has more advantages than laparoscopic-assisted surgery for anus preservation.
Footnotes
Authors' Contributions
L.L. is responsible for the integrity of the entire study, study concepts, definition of intellectual content, clinical studies, experimental studies, article editing, and review. Z.W., Q.Z., and C.W. are responsible for the literature research, clinical studies, experimental studies, data acquisition and analysis, statistical analysis, and article preparation. Z.Z. is responsible for the integrity of the entire study, study concepts and design, definition of intellectual content, clinical studies, experimental studies, article editing, and review. All authors read and approved the final article.
Ethics Approval and Consent to Participate
From February 2011 to July 2016, 80 patients with rectal cancer treated in The Second Hospital of Hebei Medical University were randomly divided into 2 groups, 40 in the TULS group and 40 in the laparoscopic group. The clinical trial study was approved by the scientific Research Ethics Committee of the Second Hospital of Hebei Medical University, and the Clinical trial registration number is 2019-P044. The patients agreed to the surgical treatment and signed the informed consent form.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.