
Abstract
Background:
The aim of this study was to explore the efficacy and safety of endoscopic ultrasound-guided biliary drainage (EUS-BD) and percutaneous transhepatic biliary drainage (PTCD) in patients with malignant biliary obstruction and failed endoscopic retrograde cholangiopancreatography.
Methods:
We searched PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov to identify studies reporting outcomes comparing EUS-BD and PTCD.
Results:
We identified 9 studies involving 469 patients. Technical success was similar for EUS-BD and PTCD (odds ratio [OR], 0.76; 95% confidence interval [CI], 0.17–3.30; P = .71). EUS-BD was associated with higher clinical success versus PTCD (OR, 2.11; 95% CI, 1.15–3.87; P = .02) in all studies. However, there was no significant difference between groups in studies using self-expandable metal stents (OR, 0.36; 95% CI, 0.06–2.00; P = .24). The reported adverse event rate was significantly lower for EUS-BD compared with PTCD (OR, 0.33; 95% CI, 0.22–0.52; P < .00001).
Conclusion:
The available literature suggests that EUS-BD is associated with fewer adverse events, greater clinical success, and comparable technical success compared with PTCD. According to the shortcomings of our study, more large, high-quality, randomized controlled trials are needed to compare these techniques and confirm our findings.
Introduction
For patients with unresectable malignant biliary obstruction (MBO), endoscopic retrograde cholangiopancreatography (ERCP) is the recommended method for biliary drainage.1,2 However, ERCP fails in up to 5%–10% of patients for various reasons, such as inability to access the papilla, surgically altered anatomy, or failed biliary cannulation.3–5 Traditionally, percutaneous transhepatic biliary drainage (PTCD) was used most often for patients with MBO and failed ERCP. However, PTCD can be associated with a high rate of adverse events (up to 33%), which may include catheter dislodgement, recurrent infection, and acute cholangitis. 6 Additionally, PTCD could lower patients' quality of life. 7 Since its first report in 2001, endoscopic ultrasound-guided biliary drainage (EUS-BD) has been used increasingly worldwide as an alternative procedure for unresectable MBO. 8 To date, a few studies have compared the outcomes of EUS-BD with PTCD after failed ERCP.9–11 A prospective study conducted by Lee et al. involving 66 patients showed that EUS-BD had similar efficacy compared with PTCD (94% versus 96%, respectively). 12 Regarding adverse events, EUS-BD may be associated with lower rates. Previous studies have reported variable results when comparing these two procedures, and studies were limited owing to their relatively small sample sizes, although several studies have been published recently. Therefore, we conducted an up-to-date systematic review and meta-analysis to compare the efficacy and safety of EUS-BD and PTCD in MBO.
Methods
Literature search
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 13 In an academic medical setting, we searched the following electronic databases to identify relevant studies between January 2000 and January 2021: PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov. The search was restricted to human subjects and English language articles. References from the initial articles were checked manually for further analysis, and disagreements between the authors were resolved by consensus. Our search strategy involved selecting English free text and the following medical subject heading (MeSH) terms: “endoscopic ultrasound,” “endoscopic ultrasonography,” “EUS,” “EUS-guided,” “biliary drainage,” “biliary stent,” “percutaneous biliary drainage,” “percutaneous transhepatic biliary drainage,” “transluminal biliary drainage,” “choledochoduodenostomy,” “hepaticogastrostomy,” and “EUS-guided biliary drainage.”
Inclusion and exclusion criteria
Two authors searched independently for original articles using the following inclusion criteria: (1) studies (including randomized controlled trials or observational studies) that compared the efficacy and safety of EUS-BD and PTCD for MBO; and (2) studies (including data and details) with at least technical success and clinical success. Studies were omitted if no adequate outcomes were reported. Noncomparative or nonhuman studies, review articles, editorials, letters, and case reports were also excluded as well as studies combining benign and malignant obstruction. Studies with sample sizes of <10 were also excluded.
Outcomes of interest and definitions
The evaluated outcomes were technical success, clinical success, and adverse events. Technical success was defined as successful stent placement, as determined endoscopically or radiographically, and clinical success was defined as improvement in symptoms and liver function tests. Adverse events were defined as any postprocedure complications, such as bleeding, biloma, and bile leakage. We also conducted a subgroup analysis according to the type of stent used in EUS-BD.
Data extraction
Two independent authors screened references and extracted the data to ensure similarity. Any disputes in data abstraction were resolved by consensus and by referring to the original article. The following study details were selected: first author, year of publication, country, study design, sample size, sex, and age. Data on the type of EUS-BD and the type of stent used in the procedures were also extracted. Attempts were made to contact the study authors if data were unavailable or uninterpretable.
Risk of bias assessment
The Newcastle–Ottawa Scale (NOS) was used to evaluate the quality of nonrandomized studies. 14 The NOS scores range from 0 to 9, and studies with scores >6 were deemed to have qualified. The randomized controlled trial quality was assessed using the Cochrane risk of bias tool, which assesses the presence of selection bias by evaluating methods of randomization and allocation concealment; performance and detection bias by checking for blinding of personnel and outcome assessment; and attrition and reporting bias by evaluating studies for incomplete and selective data reporting.
Statistical analyses
All statistical analyses were performed using Review Manager (RevMan), version 5.4.1, software (Cochrane Informatics and Knowledge Management Department, Nordic Cochrane Centre, Copenhagen, Denmark). Odds ratios (ORs) with 95% confidence intervals (CIs) were used for dichotomous outcomes. To assess heterogeneity, we used I2 statistics and the Cochran Q test, in which a P value <.1 indicated the presence of heterogeneity. We used a random effects model for I2 values >50%; otherwise, we used a fixed effects model. A two-tailed P value <.05 was considered statistically significant. We also assessed the potential for publication bias through visual inspection of funnel plot asymmetry.
Results
Study selection and trial characteristics
Figure 1 shows a flow chart of the systematic literature search strategy. The search identified 338 studies; 120 references were excluded because the titles indicated that they were duplicate articles. Of the remaining 218 articles, 163 references were excluded because the studies were not relevant to the research question; 55 full-text articles were assessed for eligibility. Among the 55 articles, 46 references were excluded for the following reasons: reviews (n = 18), meta-analyses (n = 1), case reports (n = 32), and language other than English (n = 3). The study conducted by Kongkam et al. was excluded because it combined ERCP and EUS-BD. 15 The study published by Giovannini et al. did not state whether patients with benign biliary obstruction were included. 16 Two studies were excluded as they involved both benign and MBO.17,18 Finally, 9 studies constituting 535 patients were included for quality evaluation and quantitative analysis.9,11,12,19–24 On reviewing the data collection, accordance between the two reviewers was 100%.
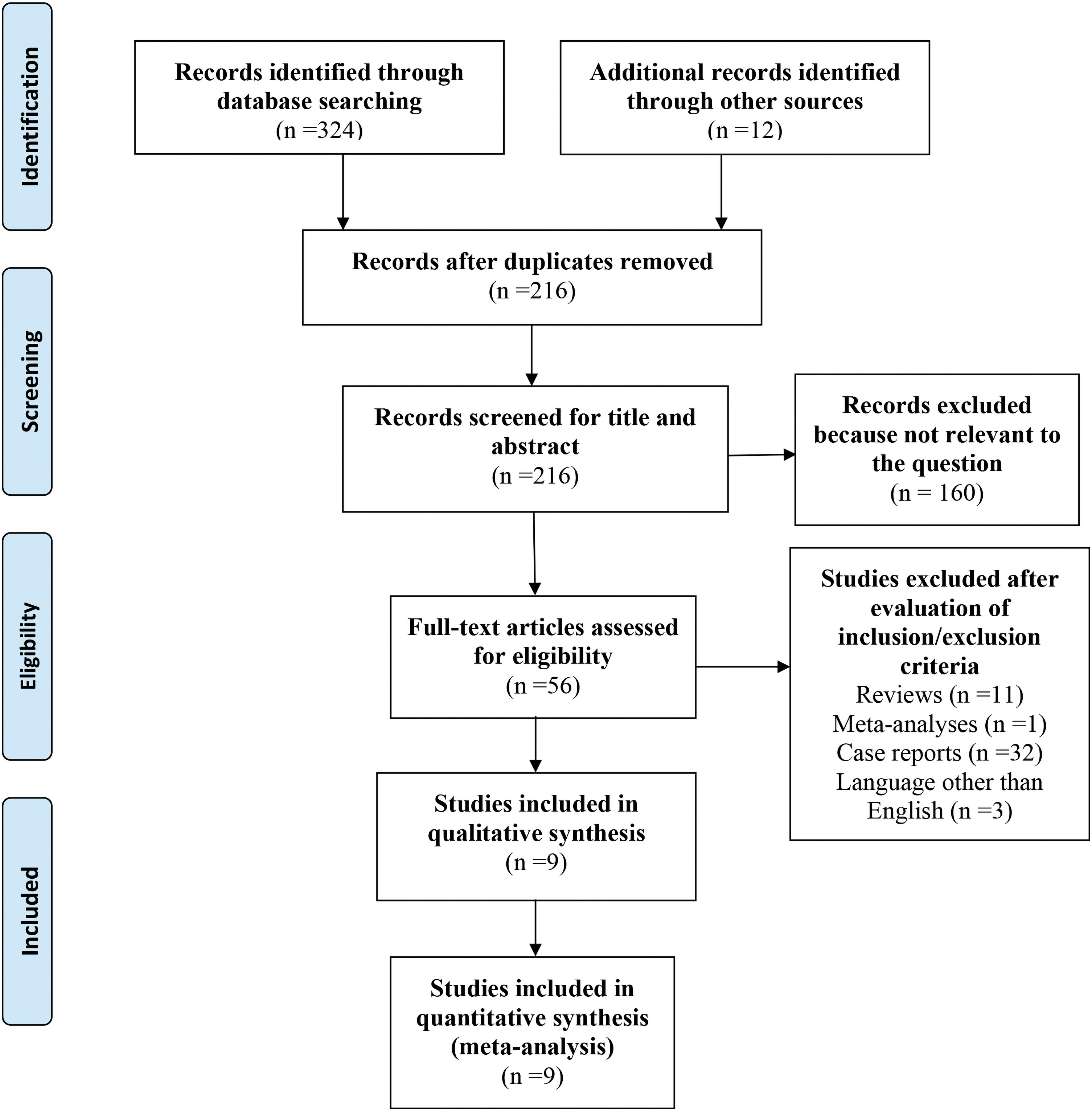
Flow diagram of the published articles evaluated for inclusion in this meta-analysis. Color images are available online.
Table 1 describes the baseline characteristics of the included articles. The publication year ranged from 2012 to 2020, and a total of 512 participants were divided into EUS-BD (256 patients) and PTCD (256 patients) groups. Regarding the study design, seven studies were retrospective studies and two were prospective studies. There were four methods used in the EUS-BD procedures, namely EUS choledochoduodenostomy (EUS-CDS), EUS hepaticogastrostomy (EUS-HGS), EUS antegrade (EUS-AG), and EUS rendezvous (EUS-RN). The types of stents used in EUS-BD were self-expandable metal stents (SEMS), plastic stents, metal stents, and lumen-apposing metal stents (LAMS). Five studies used SEMS, one study used LAMS, one study used SEMS or plastic stents, one study used metal stents, and one study did not report the stent data. The quality assessments of the included studies are plotted in Table 1. Both RCTs had high risk of performance bias, unclear risk of detection bias, and low risk of selection, attrition, and reporting bias. For the other eight observational studies, all studies had NOS scores >6.
Summary of Included Studies
EUS-AG, EUS antegrade; EUS-BD, endoscopic ultrasound-guided biliary drainage; EUS-CDS, EUS choledochoduodenostomy; EUS-HGS, EUS hepaticogastrostomy; EUS-RN, EUS rendezvous; LAMS, lumen-apposing metal stents; MBO, malignant biliary obstruction; MDBO, malignant distal biliary obstruction; MHBO, malignant hilar biliary obstruction; NR, not reported; PTCD, percutaneous transhepatic biliary drainage; SEMS, self-expandable metal stents.
Technical success
Nine studies involving 512 patients (50% in the EUS-BD group and 50% in the PTCD group) reported the technical success data. For all studies, pooled analysis demonstrated no significant difference between EUS-BD and PTCD groups for technical success (OR, 0.76; 95% CI, 0.17–3.30; P = .71) (Fig. 2a). The subgroup analysis revealed no significant differences between groups in the studies using SEMS (OR, 0.36; 95% CI, 0.06–2.00; P = .24) versus other stents (OR, 1.17; 95% CI, 0.15–9.14; P = .88) (Fig. 2b).
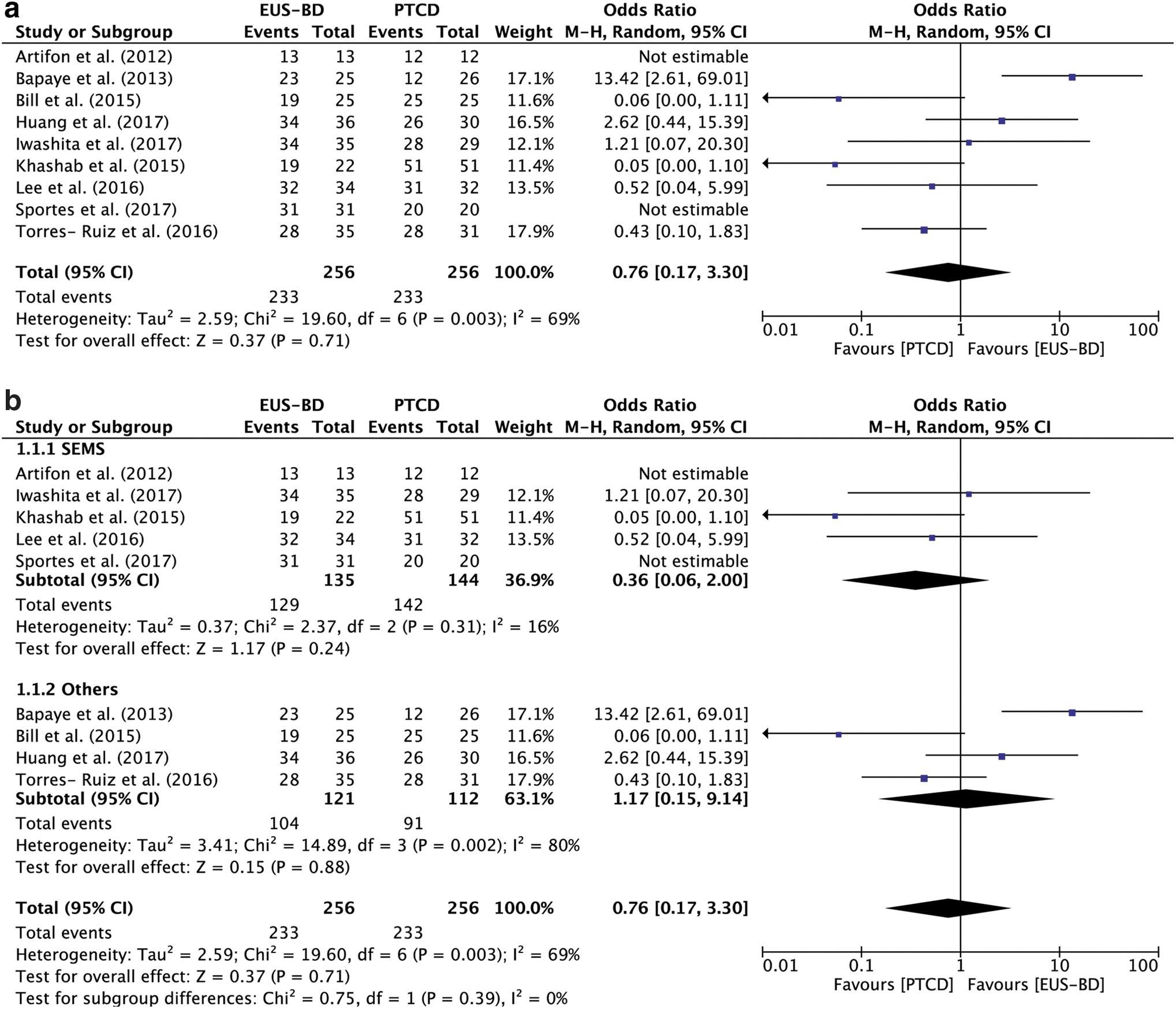
Forest plot of the meta-analysis comparing EUS-BD and PTCD according to technical success.
Clinical success
Eight studies involving 461 participants provided data for clinical success. Our study showed that EUS-BD was associated with higher clinical success versus PTCD (OR, 2.05; 95% CI, 1.19–3.56; P = .01) (Fig. 3a). The subgroup analysis revealed no significant difference between EUS-BD and PTCD in studies using SEMS (OR, 1.00; 95% CI, 0.47–2.15; P = 1.00), while EUS-BD was associated with higher clinical success versus PTCD in studies using other stents (OR, 4.67; 95% CI, 1.95–11.17; P = .0005) (Fig. 3b).
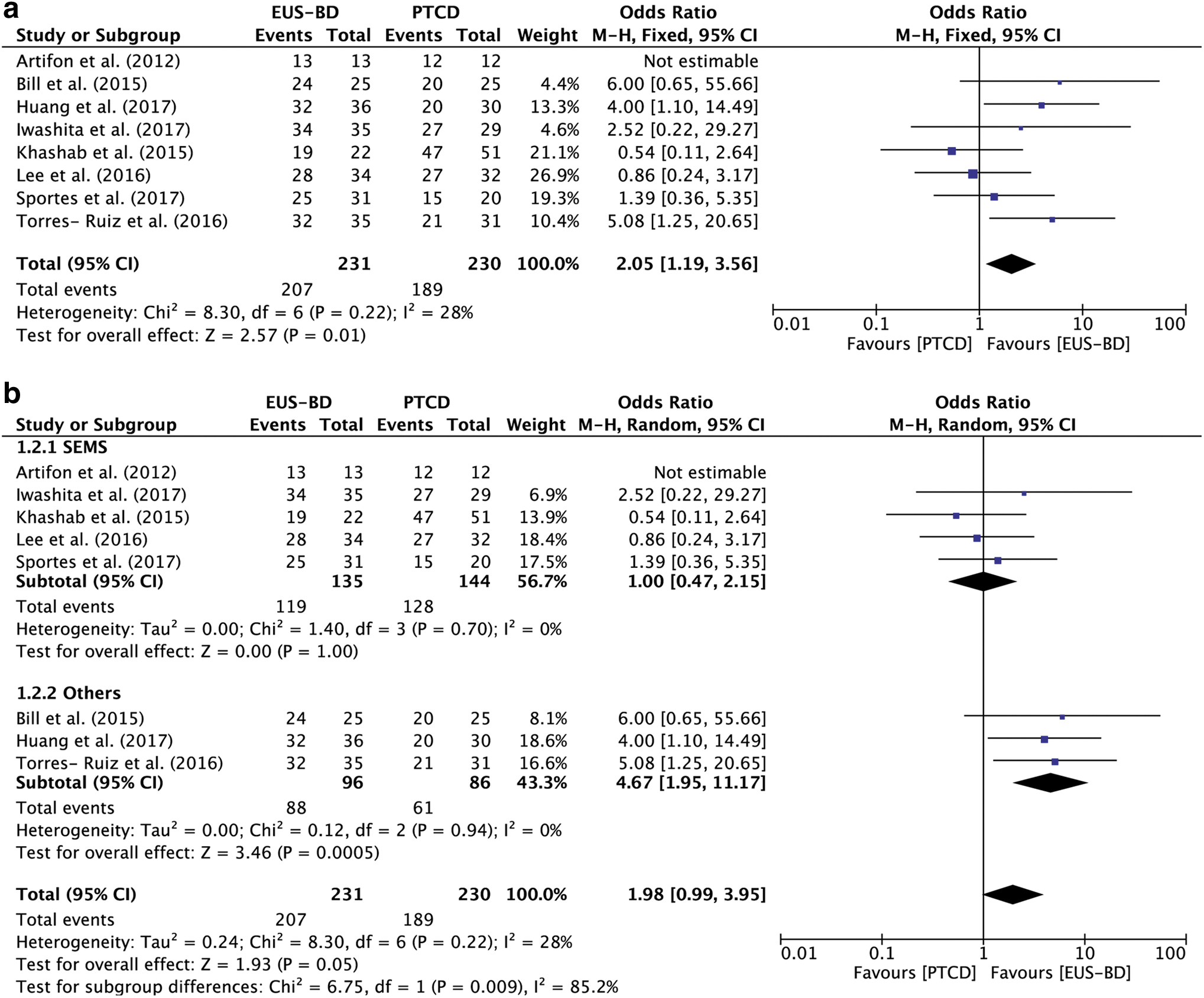
Forest plot of the meta-analysis comparing EUS-BD and PTCD according to clinical success.
Adverse events
All nine studies provided data for adverse events, which occurred in 42/256 patients in the EUS-BD group and in 107/256 patients in the PTCD group. The meta-analysis showed that EUS-BD was associated with fewer adverse events versus PTCD (OR, 0.30; 95% CI, 0.19–0.46; P < .00001) (Fig. 4a), both in studies using SEMS (OR, 0.28; 95% CI, 0.15–0.52; P < .00001) and in studies using other stents (OR, 0.31; 95% CI, 0.17–0.57; P = .0002) (Fig. 4b).
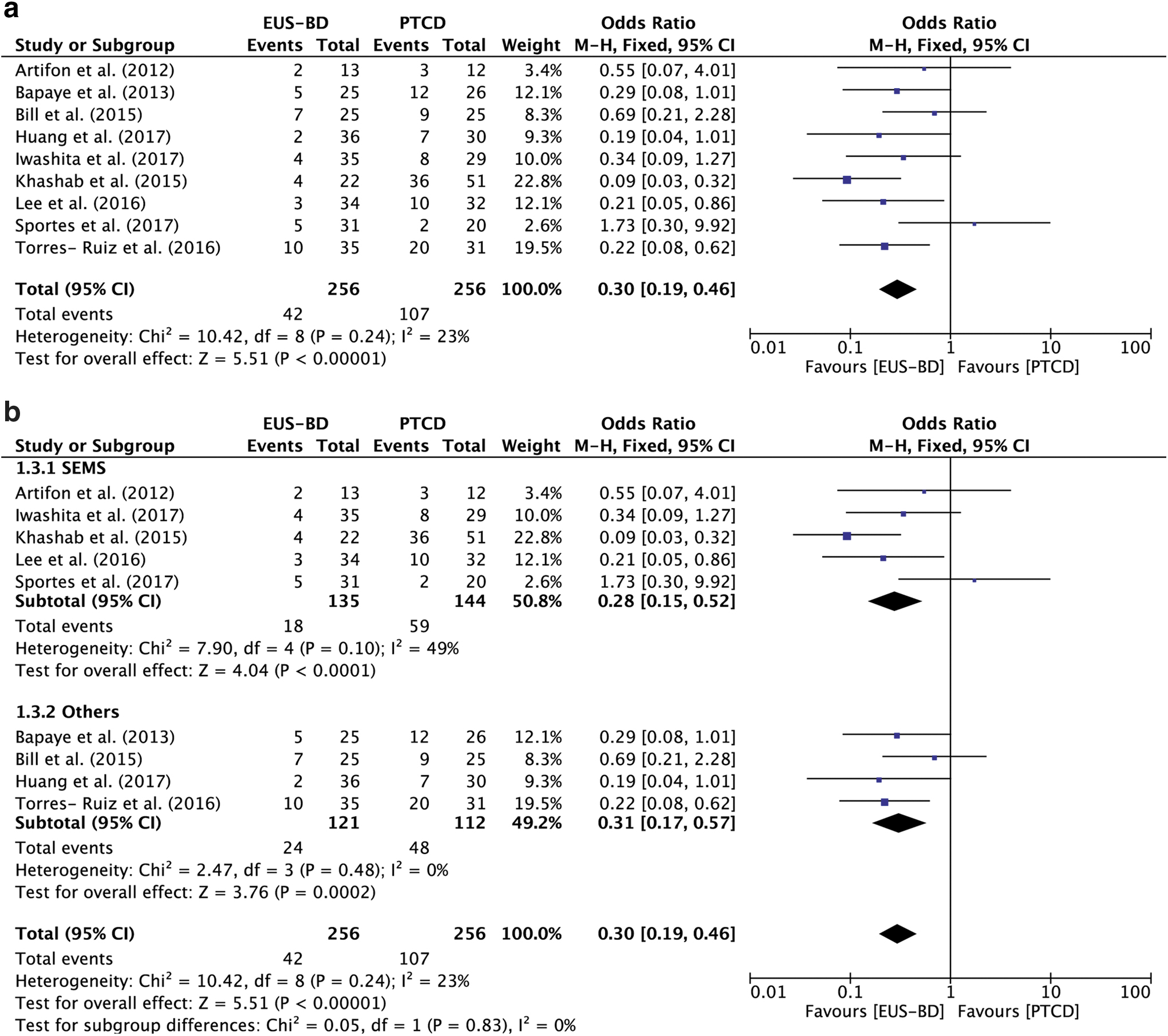
Forest plot of the meta-analysis comparing EUS-BD and PTCD according to adverse events.
Sensitivity analysis
The influence of each study on the overall meta-analysis estimate was investigated by omitting one study at a time. The omission of any study resulted in no significant difference, indicating that our results were statistically reliable.
Publication bias
Most graphical funnel plots of the parameters were symmetrical.
Discussion
We conducted an up-to-date systematic review and meta-analysis evaluating recently published studies of EUS-BD compared with PTCD for unresectable MBO after failed ERCP. The present study showed that EUS-BD had similar technical success to PTCD in all included studies. For all studies, EUS-BD was associated with better clinical success compared with PTCD. However, the subgroup analysis revealed no significant difference between EUS-BD and PTCD in studies using SEMS, while EUS-BD was associated with higher clinical success versus PTCD in studies using other stents. The meta-analysis showed that EUS-BD was associated with fewer adverse events compared with PTCD. More large, high-quality, randomized controlled trials are needed to compare techniques and confirm these findings.
For patients with unresectable MBO, various nonsurgical interventions, including ERCP and PTCD, are options. ERCP with biliary stent placement is considered the standard method for MBO. 25 When ERCP fails, PTCD is used most often as a nonsurgical procedure. However, PTCD is associated with complications, such as bleeding, cholangitis, and pneumothorax. Since its first use in 2001, EUS-BD has become widely used in the past several years. 8 Our study showed that EUS-BD has comparable technical success compared with PTCD, similar to findings in most previous studies. However, several EUS-BD procedures, namely EUS-CDS, EUS-HGS, EUS-RN, and EUS-AG, were reported for MBO in the included studies. The prospective study conducted by Artifon et al. showed that EUS-CDS and PTCD had similar technical success rates. 24 Another study performed with EUS-HGS demonstrated no difference between EUS-HGS and PTCD. Several studies, including a meta-analysis, have compared EUS-CDS and EUS-HGS. After evaluating 10 studies, Uemura et al. demonstrated that EUS-CDS and EUS-HGS had comparable technical success rates. 26 More studies of the specific techniques should be evaluated. A high technical success rate was obtained in most clinical studies, which is partly because EUS-BD has been performed in advanced endoscopy centers until recently as EUS-BD has higher technical requirements. EUS-BD is technically complex and requires a steeper learning curve. 27
Regarding clinical success, the present study showed that EUS-BD had greater efficacy than PTCD. This result was consistent with a study published in 201717; however, another meta-analysis involving six studies demonstrated no significant difference between EUS-BD and PTCD in terms of clinical success. 27 There are several explanations for this discrepancy: more studies were included in our study, and we excluded studies involving benign obstruction. Interestingly, our research found that clinical success was similar between EUS-BD and PTCD in studies in which SEMS were used. One explanation for this may be the small sample size in the included studies. Additionally, the definitions of clinical success varied in the included studies. For example, clinical success was defined as a drop in serum total bilirubin concentration of >50% or <2 mg/dL over 2 weeks in the study conducted by Iwashita et al. 9 However, in the study by Bill et al., clinical success was defined as a 50% decrease in bilirubin within 7 days.
Similar to previous studies, EUS-BD was associated with fewer complications than PTCD. It is worth noting that the definition and classification of complications in the included studies were not uniform. A meta-analysis published in 2017 classified adverse events as mild, moderate, and severe. 17 Studies have shown that there is no statistical difference between EUS-BD and PTCD regarding mild adverse events, but that EUS-BD is associated with fewer moderate and severe adverse events compared with PTCD. The main complications associated with EUS-BD and PTCD differed in the studies. The main adverse events following EUS-BD are bleeding, bile leak/peritonitis, and cholangitis, while perihepatic bile collection, hemobilia, and cutaneous leak are associated with PTCD. Furthermore, the follow-up time varied greatly in the included studies.
Differing from a previous meta-analysis of EUS-BD and PTCD, our study included the latest research. Moreover, all of the studies included in our study exclusively involved patients with MBO; no studies involving benign stenosis were included. However, there are still several limitations in the current study. First, the definitions of technical success, clinical success, and adverse events varied, which may have created bias in our study. Second, our meta-analysis was weakened by limitations inherent to meta-analyses and related to the included studies. Third, the number of cases was small, which is associated with a high risk of type II statistical errors. According to these shortcomings, more high-quality, randomized controlled studies are necessary in the future.
In conclusion, the available literature suggests that EUS-BD is associated with better clinical success and comparable technical success with PTCD, while EUS-BD is associated with fewer adverse events. According to the shortcomings of our study, more large, high-quality, randomized controlled trials are needed to compare techniques and confirm our findings.
Consent for Publication
All authors approved the publication of the manuscript.
Availability of Data and Materials
As this is a systematic review and meta-analysis, all included studies and the related results in our article are listed in the reference and article.
Footnotes
Authors' Contributions
Y.W. and Y.L. were involved in conception and design of the study. B.W. and Y.L. were involved in selection of studies. Y.C., B.W., were involved in data extraction. Y.L. and B.W were involved in statistical analyses. Y.W. and Y.L. wrote the article. The manuscript was revised and approved by Y.L.
Acknowledgment
Disclosure Statement
No competing financial interests exist.
Funding Information
This meta-analysis is supported by the scientific and technological research project of JinHua, China, No. 2021-4-142.