
Abstract
Background:
The implementation of the acute surgical unit (ASU) model has been demonstrated to improve care outcomes for the emergency general surgery patient in comparison to the traditional “on call” model. Currently, only few studies have evaluated surgical outcomes of the ASU model in patients with acute biliary pathologies. This is the first comparative study of two different emergency surgery structures in the acute management of patients with acute cholecystitis and biliary colic.
Methods:
A retrospective review of patients who underwent emergency cholecystectomy for acute cholecystitis and biliary colic at two tertiary hospitals between April 2018 and March 2019 was conducted. Primary outcomes included length of hospital stay, time from admission to definitive surgery, and postoperative complications. Secondary outcomes include proportion of cases performed during daylight hours, length of operating time, rate of conversion to open cholecystectomy, and consultant surgeon involvement.
Results:
A total of 339 patients presented with acute biliary symptoms and were managed operatively. Univariate analysis identified a shorter mean time to surgery in the traditional group compared to the ASU group (29.2 hours versus 43.1 hours; P < .001). There was no difference in mean length of stay, operation duration between models, and postoperative complication rates between groups, with the majority of surgeries performed during daylight hours. The ASU group had a greater proportion of consultant-led cases (48.2% versus 2.5%, P < .001) compared to the traditional group.
Conclusion:
Patients with acute biliary pathology requiring laparoscopic cholecystectomy achieve equivalent surgical outcomes irrespective of the model of acute surgical care.
Introduction
Acute cholecystitis is a common acute surgical presentation. 1 Randomized data support the role of early surgery in patients presenting with acute cholecystitis. 2 Early laparoscopic cholecystectomy has been demonstrated to be a safe and a more cost-effective approach than delayed-interval cholecystectomy without significant difference in morbidity rates from surgery but with reduced overall length of hospital stay, hence translating to overall cost saving in patient care. 3
The traditional approach to emergency surgical presentations, such as in those with acute cholecystitis, is managed under the on-call consultant surgeon who comanages their on-call commitments alongside routine duties.4,5 Emergency surgeries are typically placed as add-ons to the end of elective lists or are placed on emergency operating theater lists as per availability. 1 Under this model of care, patients may receive delayed consultant assessment and prolonged time to surgery. 4 At times, routine duties may be prioritized, and emergency presentations where possible may be managed conservatively. For example, cholecystitis was previously commonly managed with a 5-day admission for intravenous antibiotics and an elective booking for cholecystectomy in 6 weeks. To improve the care of the acute surgical patient, an acute surgical unit (ASU) model was introduced. The ASU model was initially established in Australia in 2005. 4 With a dedicated consultant-led ASU, the surgical management of the acute general surgical patients is prioritized based on illness severity to allow for expedient operation to be performed when required.3,5
Following the implementation of the ASU model, initial cohort studies have shown improvement in patient outcomes defined by reduced time to definitive surgery and decreased length of hospital stay through a comparison of retrospective single institution data pre- and postimplementation of ASU care in patients with acute appendicitis. 1 There are only a limited number of studies examining the application of the ASU model to acute cholecystitis. In addition, there are no studies that offer a direct comparison of the traditional “on-call” model versus the ASU model for patients with acute cholecystitis and biliary colic. This study evaluates the outcomes between the traditional model and ASU model for the management of acute cholecystitis and biliary colic.
Methods
Patient selection
A retrospective review of hospital records of patients who underwent emergency cholecystectomy at two metropolitan South Brisbane hospitals, the Queen Elizabeth II (QEII) Jubilee Hospital (Brisbane, Queensland) and Logan Hospital (Brisbane, Queensland), between April 2018 and March 2019 were examined. Patients who presented to QEII Jubilee Hospital were managed under a traditional on-call system, and patients presenting to Logan Hospital were managed under the ASU model. This reflects the current care model for emergency general surgery at each respective hospital. Ethics approval was granted by the Metro South Health Human Research Ethics Committee (LNR/2019/QMS/56922; LNR/2020/QMS/62457).
All patients ≥18 years who underwent an emergency open or laparoscopic cholecystectomy were reviewed for potential study inclusion. Patients were included if they met the diagnostic criteria for acute cholecystitis as described by the Tokyo Guidelines 2018 (TG18) or had biliary colic. 6 A definite diagnosis of acute cholecystitis was presumed if patients presented with local and systemic signs of inflammation and imaging findings characteristic of acute cholecystitis. Imaging using ultrasound or computed tomography is required for radiological confirmation. Using the TG18 severity grading criteria for acute cholecystitis, patients were assigned a severity grade of Grade I (mild), Grade II (moderate), or Grade III (severe). 6 Grade II acute cholecystitis is defined as a white cell count greater than 10.8 × 109/L, a palpable tender mass in the right upper quadrant, a duration of symptoms greater than 72 hours, or marked local inflammation (e.g., gangrenous cholecystitis). Grade III acute cholecystitis is defined as acute cholecystitis with substantial cardiovascular, neurological, respiratory, renal, hepatic, or hematological dysfunction. If patients do not meet the criteria for Grade II or Grade III acute cholecystitis, they are given the classification of Grade I acute cholecystitis. Patients with biliary colic had typical symptoms of epigastric pain that resolved with analgesia and have sonographic evidence of gallstones.
Patients with cholecystitis who were managed conservatively or who underwent a delayed interval cholecystectomy or had a cholecystectomy for a different primary indication than acute cholecystitis were excluded.
Data collection
Patient data were retrieved from the Queensland Health integrated electronic medical record. Primary outcomes include length of hospital stay, time from admission to definitive surgery, and postoperative complications (e.g., bile duct injury, postoperative infection, return to theater). Secondary outcomes included proportion of cases performed during daylight hours (0800–1700), length of operating time, rate of conversion to open cholecystectomy, and consultant surgeon involvement. Consultant surgeons hold a Fellowship in General Surgery administered through the Royal Australasian College of Surgeons and are formally appointed in the role at the hospital.
Traditional on-call model
The surgical care for patients who are admitted with an acute surgical condition is managed under a consultant of the day. The surgeon may concurrently have other commitments, including clinics or elective operating sessions, but remain available when required. A surgical fellow with the support of registrars coordinates the care of the acute patients and is tasked with the role of operating and/or supervising the cases. An emergency operating theater shared between orthopedics, urology, obstetrics and gynecology, and general surgery is reserved for surgical emergencies.
Acute surgical unit
In 2016
Statistical analysis
Data were recorded using Microsoft Excel and analyzed using SPSS® version 27.0 for Windows (IBM Corporation, New York, NY). Categorical and continuous variables were analyzed using Pearson's chi-squared test and the independent samples t-test, respectively. A P value of <.05 was considered statistically significant.
Results
Comparison of patient characteristics
A total of 339 patients underwent emergency cholecystectomy for acute cholecystitis and biliary colic. There were 121 patients in the traditional group and 218 patients in the ASU group. In the traditional group, 111 patients had acute cholecystitis and 10 patients had biliary colic (91.7% and 8.3%, respectively). Of the patients with acute cholecystitis, 7 patients (5.8%) had concurrent choledocholithiasis. Similarly, 185 patients in the ASU group had acute cholecystitis and 33 patients had biliary colic (84.9% and 15.1%, respectively). Ten patients (4.6%) in the ASU group had acute cholecystitis with concurrent choledocholithiasis.
There were no significant differences between the traditional and ASU groups in gender (65.3% versus 74.9% female; P = .052) or body mass index (30.8 kg/m2 versus 32.2 kg/m2; P = .072). Both groups were similar in TG18 severity grading for acute cholecystitis (P = .230). The ASU group was slightly younger in age (43.6 years versus 48.0 years; P = .018) with a lower prevalence of hypertension (14.2% versus 24.8%; P = .015) and higher prevalence of smoking (30.3% versus 13.2%; P < .001) than the traditional group (Fig. 1). All other patient demographics are described in Table 1.

Comparison of preoperative characteristics between traditional and ASU groups. ASU, acute surgical unit. Color images are available online.
Comparison of Preoperative Characteristics Between Traditional and Acute Surgical Unit Groups
ASA, American Society of Anesthesiologists; ASU, acute surgical unit; BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; CVD, cerebrovascular disease; DM, diabetes mellitus; HTN, hypertension; IHD, ischemic heart disease; SD, standard deviation; TG18, Tokyo Guidelines 2018; WCC, white cell count.
Surgical outcomes
The mean time to surgery was significantly shorter in the traditional group compared to the ASU group (29.2 hours versus 43.1 hours; P < .001). In the traditional group, 2.5% of operations compared to 48.2% in the ASU group were performed by a consultant surgeon (P < .001). When the traditional group was compared to the ASU group the mean length of stay (3.0 days versus 3.3 days; P = .070), mean operation duration (96.0 minutes versus 95.2 minutes; P = .869), and postoperative complication rate (9.9% versus 8.7%; P = .713) were similar between both groups. Furthermore, in both groups, the majority of surgeries were performed during daylight hours (84.3% versus 90.4%; P = .980) with neither group requiring conversion to open surgery. A summary of these comparisons is shown in Table 2 and Figures 2 and 3.

Comparison of surgical outcome measures between traditional and ASU groups. ASU, acute surgical unit. Color images are available online.
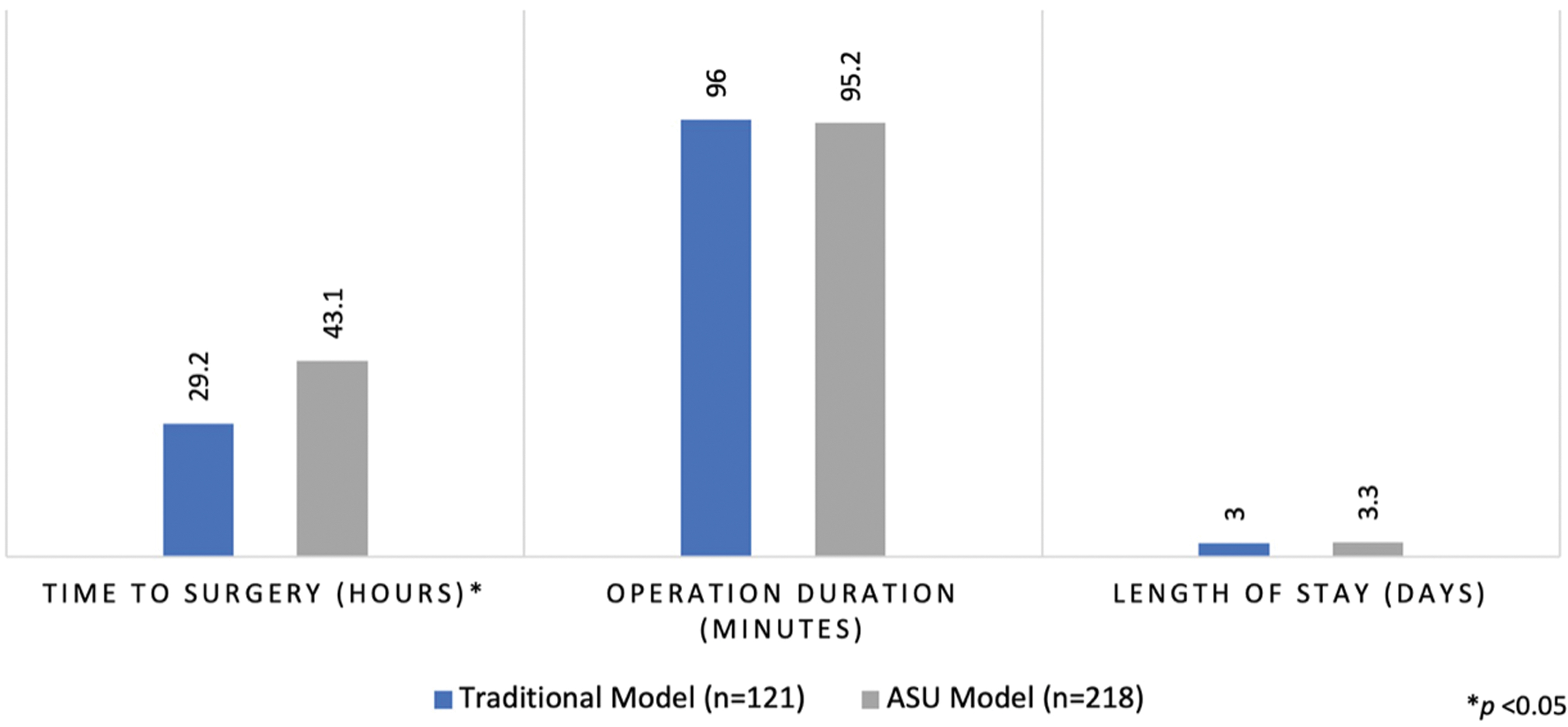
Comparison of surgical outcome measures between traditional and ASU groups. ASU, acute surgical unit. Color images are available online.
Comparison of Surgical Outcome Measures Between Traditional and Acute Surgical Unit Groups
ASU, acute surgical unit.
Discussion
Emergency cholecystectomy is associated with a higher morbidity and mortality than elective cholecystectomy.7,8 Emergency cholecystectomies are also associated with higher rates of conversion to open surgery, longer operative times, and increased length of hospital stay. 8 The ASU model was developed to improve outcomes for patients with an acute surgical condition, in particular, those requiring emergency surgery. The model prioritizes the care of this group of patients over elective surgical patients and delivers patient care through a team-based approach led by a consultant surgeon. This alleviates the competitive demands and priorities of the on-call surgeon who may be engaged in other clinical commitments who then have to juggle the responsibilities of caring for the acute surgical patient and elective clinical commitments. 9 The dedicated ASU surgeon does not have elective clinical commitments and hence provides day to day patient care, ensuring continuity of care, and provides input into decision-making at the level of a senior surgeon who is on-site and available for emergency surgery operations.
Since the implementation of the ASU care model, various studies have evaluated the impact of the ASU model on surgical outcomes for patients with appendicitis, acute cholecystitis, and small bowel obstruction.4,10 In a meta-analysis by Murphy et al. (n = 25), patient outcomes for appendicitis and/or acute biliary disease pre- and post-ASU were examined. 11 When the pre-ASU cohort was compared, these studies demonstrate that the ASU cohort had a shorter length of stay by 0.51 days for appendicitis (confidence interval [95% CI] −0.81 to −0.20 days) and 0.73 days for biliary disease (95% CI 0.09–1.36 days). The authors also report fewer complication rates for appendicitis and biliary disease in the ASU group (odds ratio [OR] 0.65; 95% CI 0.49–0.86 and OR 0.46; 95% CI 0.34–0.61, respectively) compared to the pre-ASU cohort where a traditional on-call general surgery model would have been in place.
Currently, there are no direct comparison studies of the ASU model to the traditional model for acute cholecystitis. The only available studies compare outcomes in a single institution pre-ASU to post-ASU implementation. Studies in Australia found that in comparison to pre-ASU patients, the ASU group had a shorter length of stay in hospital and shorter time to definitive surgery.1,3,5 The ASU group was also found to have fewer complications and lower rates of conversion to open surgery.1,3 These improvements are likely a result of the designation of an emergency operating theater. The ASU model in Australia indicates an improvement in care patterns for patients with acute cholecystitis.
In an emergency surgical unit in the United Kingdom, Bokhari et al. similarly report a reduction in overall length of stay due to a higher rate of early laparoscopic cholecystectomies being performed. 12 This reduction in length of stay translated into significant cost savings. However, a higher rate of conversion to open cholecystectomy (9% versus 0%) in the ASU group compared to the traditional group was observed. 12 This may reflect a practice trend of being more aggressive in offering surgery to patients compared to opting for conservative treatment with salvage nonoperative procedures such as a cholecystostomy in patients with severe cholecystitis. In America, similar findings are observed with reduction in length of stay.13–15 A summary of these studies is shown in Tables 3 and 4.
Primary Surgical Outcomes Reported in Studies Comparing Models of Care in Emergency Cholecystectomy
P < .05.
ASU, acute surgical unit; T, traditional model; —, indicates not reported.
Secondary Surgical Outcomes Reported in Studies Comparing Models of Care in Emergency Cholecystectomy
P < .05.
ASU, acute surgical unit; T, traditional model; —, indicates not reported.
These results together demonstrate that the ASU model selects patients for early laparoscopic cholecystectomy in an expedient manner hence reducing the length of time from admission to definitive surgery, translating to reduced length of stay and overall cost savings in patient care. In contrast to previous studies, the length of time to operation in our study was found to be longer in the ASU group compared to the traditional group. These differences may be explained by differences in how each institution runs the ASU. The ASU examined in this study utilizes a shared emergency theater with other specialties, including orthopedics, obstetrics and gynecology, and general surgery, with two to three sessions allocated solely for ASU patients. Other ASU models have a dedicated theater assigned for acute surgical emergencies. 9 The utilization of a shared operating theater may lead to unexpected surgical delays if the theater is being used by another surgical specialty. Our study also identified that a high percentage of operations were completed by surgical consultants in the ASU group compared to the traditional model where the operations were typically performed by registrars and surgical fellows. Lehane et al. in a cohort study of 202 patients reported higher consultant presence in the operating theater in the ASU group compared to the traditional group (73.9% versus 56.3%; P = .009). Consultant involvement in emergency surgeries has been shown to decrease complication rates. 9 Increased consultant participation also provides a suitable teaching environment for surgical registrars, allowing them to learn in a supervised environment. 16 These outcomes suggest that under the ASU model, greater consultant presence may have a beneficial effect on both the patient and surgical trainees.
Access to the emergency theater is dependent on competing needs from other specialties and is based on patient categorization and length of time waiting. Although emergency laparoscopic cholecystectomy is now considered a standard of care, the majority of patients with acute cholecystitis do not meet criteria to being a true emergency and hence are booked on a 24-hour priority category that when competing interests occur from other more emergent cases, laparoscopic cholecystectomies can often be further delayed and even postponed. The ASU model was developed to improve operating theater availability and reduce the need for after-hour surgeries. Interestingly, the traditional model examined in this article challenges previous results and shows a comparable number of surgeries performed during daylight hours as the ASU model. This suggests that implementation of an ASU in a smaller nontertiary hospital, where operating theater key performance index is often based on the number of elective cases performed, may limit its overall throughput and effectiveness due to a limitation of resources. In a smaller hospital, close collaborations between anesthetists and surgeons across disciplines along with the nursing teams would best promote effective management of theater lists and utilization of theater time to facilitate the completion of emergency cases.
This study is the first true comparative study of two different emergency surgery structures, the traditional on-call model versus the ASU model in the acute management of patients with cholecystitis. At present, the ASU model has only been evaluated through single institution pre- and post-ASU implementations. While the studies are useful, the results cannot be generalized because of the bias that exists from a single institutional comparison. In summary, patients with acute biliary pathology requiring laparoscopic cholecystectomy can be effectively managed in either a traditional or ASU model of care with comparable outcomes.
Footnotes
Authors' Contributions
Conceptualization: T.C.C., M.J.B., P.J.Y.; Data Acquisition: A.W.; Data Analysis: A.W.; Article Preparation: A.W., T.C.C.; Final Reviews: T.C.C., M.J.B., P.J.Y., R.P.L., S.N., A.W.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding received.