
Abstract
Background and Objectives:
The role of laparoscopy during a pancreatoduodenectomy (PD) is not clearly defined. The purpose of this study was thus to compare the cost-effectiveness between laparoscopic pancreatoduodenectomy (LPD) and open pancreatoduodenectomy (OPD).
Materials and Methods:
From 2010 to 2019, 140 patients underwent PD (60 LPD and 80 OPD). After 60–60 matching, the clinical-pathological characteristics, surgical technique, and type of rehabilitation were identical in both groups. Complications, R0 resection, and cost were compared.
Results:
Complication rates were 48% (12% Clavien-Dindo grade 3–4) in the LPD group and 64% (22% Clavien-Dindo grade 3–4) in the OPD group. The LPD group had significantly fewer pulmonary complications (6%) than the OPD group (20%) (P = .04). The oncological quality of the R0 resection did not differ between the two groups. The operating time was 312 ± 50 minutes in the OPD group and 392 ± 75 minutes in the LPD group (P < .001). The mean length of hospital stay was significantly shorter for the LPD group (13 ± 10) days compared to the OPD group (19 ± 8) days (P = .02). The average cost of total hospital stay was significantly lower for the LPD group compared to the OPD group (P = .02).
Conclusions:
Despite longer operative times, LPD had fewer (pulmonary) complications and reduced hospital costs.
Introduction
Almost all digestive surgery can be performed laparoscopically, improving morbidity and the resumption of physical and occupational activities. Pancreatoduodenectomy (PD) is a long and difficult procedure associated with high morbidity (25%–65%), which can lead to long hospital stays. 1 Although it is the only curative treatment for pancreatic cancer, the prognosis for this disease remains quite poor. In this context of high morbidity and poor prognosis, could laparoscopy improve certain parameters for the patient? Despite the advantages gained from minimally invasive surgery, the spread of PD by laparoscopy is slow for several reasons.
The first is that minimally invasive surgery involves a long learning curve and surgical dexterity, 2 the second is the postoperative and oncological results obtained in the literature, which are not very encouraging, and the third is the cost, which is not very well evaluated.3–6 The aim of our study was to compare the cost-effectiveness of laparoscopic pancreatoduodenectomy (LPD) and open pancreatoduodenectomy (OPD).
Materials and Methods
Patients
From 2010 to 2019, the data of all patients who had a PD (n = 216) were obtained from medical records of hospitalization, consultation, and the code of the Programme for the Medicalization of Information Systems (PMSI). This study was reviewed and approved by the Institutional Ethics Committee in April 2020.
Data collection
The clinical, biological, and anatomopathological data were retrieved from the Clinicom® and Cyberlab® software packages, preoperative and postoperative consultation reports (surgery and anesthesia), operating reports, and hospitalization reports from the digestive surgery department and the intensive care unit. The start and end of treatments (in particular, sandostatin and erythromycin) were retrieved from the Pharma® software, which indicates all the prescriptions and their completion during the hospital stay.
Inclusion criteria
Patients included were those operated on for a PD by laparotomy or laparoscopy for a tumor of the head of the pancreas (malignant or benign tumors), a noncancerous disease of the cephalic pancreas, a choledochlear tumor, and an ampullary or duodenal tumor. Only patients with the same surgical technique and surgical setup were included.
Exclusion criteria
Patients excluded were those who had exploratory laparotomy or laparoscopy that revealed a contraindication to PD and patients who had left pancreatectomy or total pancreatectomy, pancreatic shunt.
Matching
From 2010 to 2015, 80 patients had consecutive intention-to-treat OPD and from 2016 to 2019, 60 patients had successive intention-to-treat and LPD, respectively, by the same operator and surgical technique (Fig. 1). Patients who had LPD were matched to patients who had OPD: age, body mass index, American Society of Anesthesiologists score, albuminemia, heart and lung status, tumor type, and digestive reconstruction technique. In the laparoscopy group, 5 patients were converted by laparotomy. The 5 patients who were converted were included in the match.
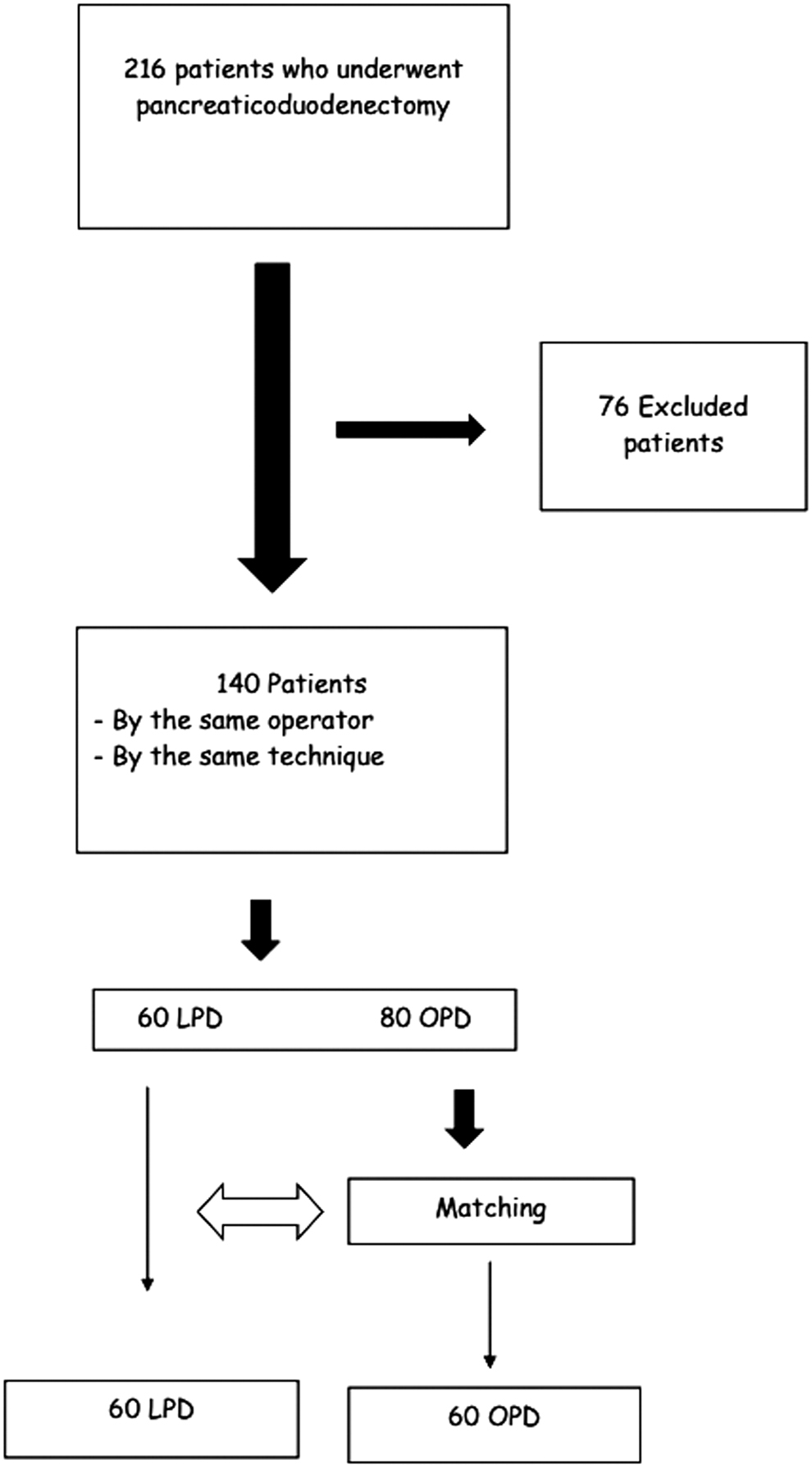
Flow chart.
The causes of conversion were tumoral invasion of the mesenteric vein requiring resection of the vein with venovenous anastomosis, tumor adhesions with the superior mesenteric artery, the presence of a right hepatic artery hindering dissection of the retroportal blade, aneurysm of the hepatic artery, and tumor invasion of the inferior mesenteric vein requiring partial resection of the inferior mesenteric vein. Patients with intention-to-treat LPD were matched with 60 patients with OPD.
Biliary drainage
Preoperative biliary drainage was not systematically performed. The indications were a total bilirubin level threshold above 150 μmol/L, angiocholitis, and the presence of coagulopathy. The method was endoscopic retrograde cholangiopancreatography with a plastic or metal stent performed by gastroenterologists.
Surgical procedure
The patients included in this study were patients operated on by a surgeon with expertise in laparoscopy and pancreatic surgery, who performed the same dissection and reconstruction (anastomosis) technique regardless of the approach, allowing technically homogeneous groups.
The approach for the OPD was a right subcostal incision. The surgical technique was the same regardless of the approach. Restoration of pancreatic continuity was achieved by jejunal pancreatic anastomosis for LPD and OPD. The assembled jejunal loop was passed behind the mesenteric vessels to perform the pancreaticojejunal anastomosis with two hemisections of 4/0 monofilament nonresorbable suture taking the pancreatic parenchyma without crossing the jejunal mucosa and the pancreatic duct, followed by biliojejunal anastomosis with two hemisections of 4/0 braided resorbable suture. The pancreatic duct was never taken in the suture or stented (Fig. 2).
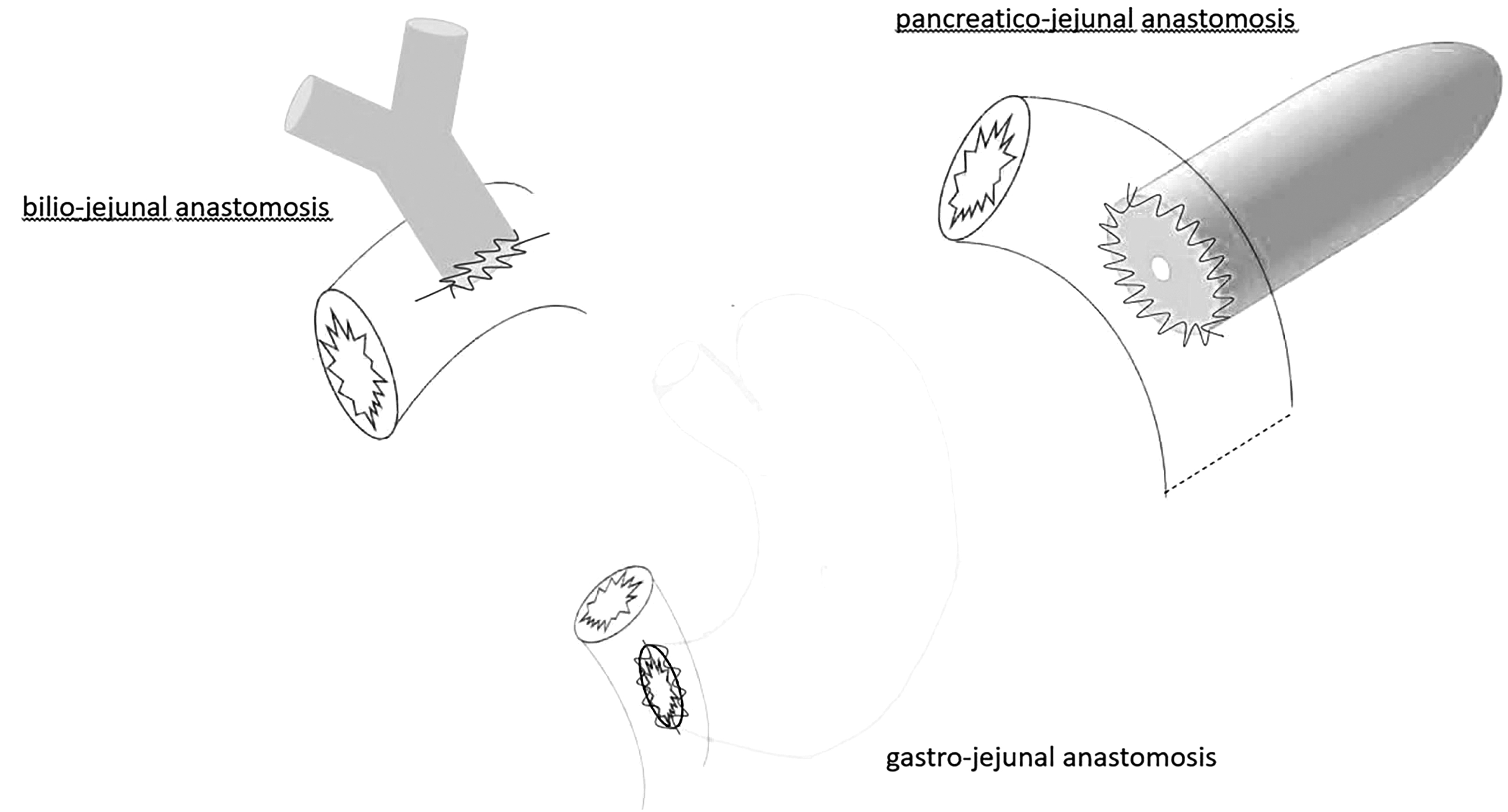
pancreaticojejunal, biliojejunal, and gastrojejunal anastomosis.
Gastrojejunal anastomosis was carried out in precolic with two hemisections of resorbable monofilament 4/0 thread. All DPCC anastomoses were performed under laparoscopy. A mini laparotomy was performed only to externalize the specimen.
Postoperative rehabilitation program
The enhanced recovery program was identical in both groups before and after matching the following: peridural analgesia, amount of perioperative IV fluid infusion, mobilization, and respiratory physiotherapy. After the operation, all patients went to continuing care.
Definitions
The R0 resection margins were assessed at 1 mm. The TNM American Joint Committee on Cancer (AJCC) 2017 classification was used. 7 The classification changed between the beginning and the end of the study: appearance of the N0 N1 N2 character for the new classification, in the other classification, the patients were N0 or N1; for this reason we indicate N0 or N+ to homogenize the results.
Complications were classified according to degree of severity (minor or major) using the Clavien-Dindo classification, including postoperative pancreatic fistula (POPF), delayed gastric emptying (DGE), bile leakage, and postoperative bleeding.8–12 Pancreatic fistulas were diagnosed by means of the dosages systematically performed in the drains at D3 and D5 postoperatively. The duration of the operation corresponded to the time between incision and closure. The duration of hospitalization corresponded to the time between the day of the operation and the day of discharge.
Economic evaluation
The cost of hospitalization was calculated according to the length of stay and the price of the stay (1265.15 Euros in the digestive surgery department and 2049.97 Euros in continuing care). The cost per unit of all imaging procedures, interventional imaging, anesthesia, operation/reoperation, operation materials and hospitalization was obtained from the French classification of medical interventions (CCAM) (https://www.ameli.fr/accueil-de-la-ccam/index.php) and the PMSI data for each intervention. The costs of the instruments, which were usually re-sterilizable, were not taken into account as these costs were amortized by the other laparoscopic and laparotomy procedures.
Statistical analysis
The group of patients undergoing intention-to-treat LPD (n = 60) was compared to the group of patients undergoing OPD (n = 60). The qualitative variables were summarized in contingency tables showing the numbers and percentages associated with each modality of the variable and were compared by the Chi-squared test or the Fisher's exact test when the Chi-squared conditions were invalid. The quantitative parametric variables were described by mean and standard deviation and were compared by a t-test. Quantitative nonparametric variables were described by the median and extremes and were compared by the Wilcoxon-Mann-Whitney test. All tests comparing the two groups were bilateral at the 5% threshold. The data were analyzed using IBM® SPSS® version 23.7 software.
Results
Preoperational characteristics before and after matching
The characteristics of the population are summarized in Table 1. No patient had preoperative chemotherapy or radiochemotherapy and 52 patients in the LPD group and 67 patients in the OPD group with adenocarcinoma, pancreatic head/ampullary, or cholangiocarcinoma tumor received adjuvant chemotherapy. After matching, re-operative biliary tract drainage was significantly more frequent in the LPD group (73% in the LPD group versus 47% in the OPD group, P = .05) and active smoking was significantly more common among patients in the LPD group (36% in the LPD group versus 15% in the OPD group, P = .015). Before matching, the mean albumin level was higher for the LPD group (36.2 g/L) than for the OPD group (31.1 g/L, P = .001) and after matching, the mean albumin levels did not differ between the groups.
Comparison of Baseline Characteristics Between Laparoscopic Pancreaticoduodenectomy and Open Pancreaticoduodenectomy Groups Before and After Matching
ASA, American Society of Anesthesiologists; BMI, body mass index; LPD, laparoscopic pancreatoduodenectomy; OPD, open pancreatoduodenectomy.
The type of pancreatic tumor is described in Table 2. The two groups were homogeneous with regard to the location of tumor lesions. Most patients were operated on for pancreatic head and periampullary adenocarcinoma.
Comparison of Pathologic Findings Between Laparoscopic Pancreaticoduodenectomy and Open Pancreaticoduodenectomy Groups Before and After Matching
LPD, laparoscopic pancreatoduodenectomy; OPD, open pancreatoduodenectomy.
Result after matching
Intraoperative characteristics
The operative time was significantly less for the OPD group (312 ± 50 minutes) than for the LPD group (392 ± 75 minutes) (P < .001). There was less blood loss in the LPD group (194 mL on average ±196) than in the OPD group (375 mL on average ±361) (P = .01). Two patients in the OPD group and 2 patients in the LPD group had a superior mesenteric portal/vein resection.
Morbidities
Postoperative complications are described in Table 3. The rate of pulmonary complications was higher in the OPD group (20%) than in the LPD group (6%) (P = .04). One of the patients in the LPD group had two pulmonary complications (Acute Respiratory distress syndrome [ARDS] and pneumopathy) and 4 patients had two pulmonary complications (ARDS, pneumopathy or effusion) in the OPD group counted. Before matching, postoperative mortality in the LPD and OPD groups was 3% (n = 2) and 1% (n = 1) (P = .2), respectively. After matching, postoperative mortality in the LPD and OPD group was 3% (n = 2) and 2% (n = 1) (P = .8), respectively.
Perioperative Outcomes of All Unmatched Patients Who Underwent Laparoscopic Pancreaticoduodenectomy or Open Pancreaticoduodenectomy
Interval for readmission: 90 days
LPD, laparoscopic pancreatoduodenectomy; OPD, open pancreatoduodenectomy.
Anatomopathological and oncological results
The TNM stages are described in Table 4. Perinerve sheathing was more frequent for patients in the LPD group (76%) than in the OPD group (50%) (P = .01). There was no significant difference between the two groups with regard to the oncological quality of the resection (R0 resection), nor with regard to lymph node removal: the number of lymph nodes removed did not differ significantly between the two groups.
Pathologic Findings of Matched Patients Who Underwent Laparoscopic Pancreaticoduodenectomy or Open Pancreaticoduodenectomy
Nondegenerated noninvasive intraductal papillary mucinous neoplams: 2 missing in the LPD group and 2 in the OPD group.
AJCC, American Joint Committee on Cancer; LPD, laparoscopic pancreatoduodenectomy; OPD, open pancreatoduodenectomy.
Length of stay
The average length of hospital stay was significantly shorter for the LPD group (13 days on average) (±10) than for the OPD group (19 days) (±10) (P < .001). The average length of stay in continuing care was 4.8 days (±3) in the LPD group and 5 days (±4) in the OPD group (P = .65). Forty-five patients (90%) in the LPD group and 44 patients (88%) in the OPD group had a home discharge (P = .99).
Cost of hospital stay
The average cost of the stay in continuing care was lower in the LPD group (13,242.8 Euros on average ±10,912) than in the OPD group (16,030.7 Euros ±14,140) (P = .3) (Table 5). The average cost of the total hospital stay was significantly lower for the LPD group (22,023 ± 1285) compared to the OPD group (28,758 ± 1507) (P = .02). Total costs in the LPD group and the OPD group were, respectively, 1,101,147.36 and 1,437,908.72 Euros, that is, a difference of 336,761.36 Euros.
Cost of the Hospital Stay of Matched Patients Who Underwent Laparoscopic Pancreaticoduodenectomy or Open Pancreaticoduodenectomy
LPD, laparoscopic pancreatoduodenectomy; OPD, open pancreatoduodenectomy.
Discussion
This study comparing LPD to OPD suggests that laparoscopy offers significant economic advantages with the same or less morbidity than laparotomy. Some limitations of this study are worth mentioning: the retrospective and monocentric design of the study, and the involvement of only one expert center and one expert operator. This characteristic, however, avoids biases linked to the experience of the operator, the center, and the medical team and related to the surgical technique, which remains the same whatever the approach. This rigor made it possible to objectively formalize the place of LPD on the basis of this study.
While feasibility has been demonstrated in studies from expert centers, it depends above all on the surgical indication and the surgeon's experience. In recent decades, medical imaging has made it possible to better select resectable patients. On the other hand, the surgeon's experience in this field always requires a more or less long learning curve of 50 procedures. 2 The most constraining element for the surgeon is the duration of the operation. In our study, the operative times were longer for LPD than for OPD. This difference has been found in several studies. 13
Dang et al., however, describe shorter operative times in the LPD group and explain this by the time taken to close the abdomen for LPD, which is much shorter than for OPD, along with the effect of a long learning process for the surgeons. 1 This longer operative time, however, did not appear to have any effect on the clinical condition of the patients in view of the results of the literature and our experience. 13
A poor preoperative evaluation of the patient, resection difficulties, and the patient's morphotype can lengthen the operative time and even force a conversion by laparotomy. The conversion rate in our study was 15% of LPD to laparotomy. Data from the literature show rates ranging from 15% to 31%. 14 These conversion rates are expected to decrease with surgical experience and improved patient selection.
In 2020, the meta-analysis of Aiolfi et al., including 41 studies involving 56,440 patients (5570 LPD and 48,382 OPD), found similar complication rates to our study. 13 Two beneficial effects of laparoscopy were consistently found, the first on the rate of pulmonary complications and the second on preoperative blood loss.
In our study, compared to OPD, LPD was associated with a significant reduction in infectious and general pulmonary complications. This decrease in respiratory complications has been found in heavy operations such as esophagectomy. In meta-analysis, postoperative complications after minimally invasive esophagectomy were significantly decreased compared to open esophagectomy 15 ; this decrease in pulmonary complications has also been demonstrated after LPD or robot PD in meta-analysis.13,16,17
A recent study showed a beneficial effect, although not significantly, after minimally invasive pancreatectomy, with rates of 0% versus 17% in laparotomy. 18 There are several explanations for this improvement. The first is the reduction of postoperative pain by mini invasive surgery, which has been shown to lead to a decrease in the incidence of pneumonia in several studies.19,20 Other explanations, however, have been found such as a reduction in tissue trauma, pulmonary impairment, and response to systemic stress.13,16,17
Similarly, LPD was associated with a significant reduction in blood loss in our study and in many studies. Reducing blood loss and reducing the need for transfusion would have an impact on the prognosis of patients with cancer and would likely preserve patients' immune systems and enhance the antineoplastic response.16,21 Kazanjian et al. describe an improved survival rate after LPD for pancreatic head neoplasm in patients with limited (<400 mL) operative blood loss. 22 In our study, the pancreatic fistula rate (grade B and C) was in the low range in both groups (10% for LPD and 12% for OPD) compared to data in the literature, which estimates fistula rates ranging from 4% to 20%.9,13 The expertise of our center with the standardization of preoperative and postoperative care protocols is a factor explaining these rates.
Our study showed that the length of stay was shorter in the LPD group. Although pancreatic complications (fistula) did not differ between the two groups, the reduction in respiratory complications and intraoperative bleeding likely improved patient recovery. The beneficial effects of laparoscopy found in many studies, such as a reduction in the length of postoperative stay, surgical site infections, intraoperative bleeding and pulmonary and general complications, allow easier access to adjuvant treatment and potentially improve survival. 23
As a result, laparoscopic surgical management is recommended for several neoplastic diseases, such as colon cancer, for example. 24 Croome et al. have found that LPD is associated with a shorter hospital stay and faster recovery than OPD and allows patients to recover more quickly and pursue adjuvant treatment options. 25 Several studies, however, have tended to oppose the minimally invasive approach to LPD and have insisted on careful patient selection.3,4
In our study, the lack of significant difference in oncological outcomes was also a major finding. There was no significant difference between the two groups in terms of the oncological quality of the resection, the rate of recurrence at 1 year, or the delay of adjuvant treatment due to surgical complications. Several studies also found similar results.13,26,27
The literature confirms the feasibility and good results of LPD, but economic evaluation has rarely been addressed, especially the cost of stays. 27 Our study showed a difference in hospitalization costs between the two approaches in favor of laparoscopy. The reduction in the length of hospitalization in the LPD group largely compensated for the extra cost of laparoscopy. The reduction in the cost of hospital stays resulted in a saving of almost 6735 Euros, on average, for each patient, that is, 336,761.36 Euros, including the patients operated on by laparoscopy during the observed period. Due to the current policy of reducing health care expenditure, this saving can be a very important argument for expert surgical services.
A recent study evaluating the costs of DP shows that LPD is associated with an increase in the cost of care in low- to medium-volume centers and is cost-neutral in very high-volume centers. 28 The extra cost is explained first by the cost of managing complications, which can lead to cost differences between centers, and second by the inherent costs associated with LPD (increased operative time and equipment costs), which are mitigated by the economies of scale achieved by very high-volume centers. Numerous studies have shown that increased DP costs are related to the management of complications. While major complications (sepsis, bile leakage, DGE, and pulmonary, renal, and thromboembolic complications) contributed to increased costs after DP, POPF was the main factor in over-costing.29–33
The few cost studies that have examined the cost associated with index hospitalization alone, however, have shown that there is no excess cost after LPD.34–36 Consequently, the extra costs reproached for the laparoscopic approach are not due to postoperative complications. Indeed, systematic reviews of the literature and meta-analyses have found that LPD was not associated with any clinically major difference in postoperative outcomes such as resection margins, POPF rates, bile leakage, DGE, reoperation rates, intraoperative and postoperative mortality, and blood loss compared to OPD.13,37
In our study, the rates of postoperative complications were not significantly different between the two approaches. These results confirm that the additional costs associated with the laparoscopic approach are not due solely to postoperative complications, but to other characteristics of the laparoscopic approach, such as operative time and laparoscopic instrumentation and equipment. A study evaluating the cost in patients undergoing PD in high-volume centers by Tran et al. found that patients undergoing LPD in high-volume centers had lower costs of care ($76,572 versus $106,367, P < .01) than patients undergoing OPD when comparing clinical outcomes at 30 days postoperatively. 36
Low- to medium-volume centers should be more careful in the indication of LPD, and in the application of national early rehabilitation protocols to accredit their institution to perform laparoscopic procedures in patients with pancreatic disease.
In conclusion, despite its longer operative time, LPD had fewer (pulmonary) complications and reduced hospital costs. As the learning curve is significant, however, this minimally invasive pancreatic surgery must be performed in expert centers.
Footnotes
Authors' Contributions
Study conception and design: F.B., C.P., and S.F. Acquisition of data: C.P. and M.N. Analysis and interpretation of data: F.B., C.P., and S.F. Drafting of article: C.P. and F.B. Critical revision of article: F.B. and S.F.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.