
Abstract
Background:
In recent decades, laparoscopic liver resection (LLR) has been gradually adopted at high-volume centers, particularly for hepatocellular carcinoma and liver metastasis. However, LLR in patients with gallbladder cancer (GBC) is a controversial issue, and there are few studies of LLR for GBC. Our aim was to compare the outcomes of patients who underwent laparoscopic or open liver resection for GBC.
Materials and Methods:
All patients admitted with stage II or III GBC requiring liver resection, together with cholecystectomy and lymphadenectomy, were analyzed retrospectively. Patients with thickness of the resected liver specimen >2 cm in pathology reports were included.
Results:
A total of 56 patients with stage II or III GBC were included in this study; 23 (41.1%) underwent laparoscopic surgery and 33 (58.9%) underwent open surgery. Propensity score matching was performed using a 1:1 matching scheme. After matching, 12 patients were included in each group. The preoperative characteristics of both groups were similar, as were the operative times (laparoscopic versus open group: 237.5 minutes versus 272.5 minutes, respectively; P = .319) and blood loss (300 mL versus 275 mL, respectively; P = .307). The laparoscopic group had a significantly shorter postoperative hospital stay than the open surgery group (4.5 days versus 8 days, respectively; P = .012). There were no major complications in either group. There was no difference between the groups in the number of lymph nodes harvested at surgery (P = .910). There were no differences between the two groups in disease-free (P = .503) or overall (P = .719) survival.
Conclusion:
LLR extended to GBC provides outcomes similar to those of open surgery. With increasing experience, LLR can be a viable alternative to open surgery for GBC.
Introduction
Although cholecystectomy was the first procedure performed with laparoscopy, the use of laparoscopy for gallbladder carcinoma (GBC) is still not widely accepted. 1 This is attributable to the disadvantages associated with laparoscopy, such as the risk of bile spillage, port-site recurrence, and the inadequacy of lymph node dissection. 2 Nevertheless, there was a good study showing the safety of laparoscopy for GBC in the early stage of the disease. 3 A recent comparative study of laparoscopic and open cholecystectomy for stage TII GBC showed the oncological similarities of laparoscopy and open surgery. 4 Therefore, laparoscopic surgery can be well suited for the surgical treatment of GBC.
Liver resection is necessary in patients with stage ≥II GBC, and may involve wedge resection or segment IVB and V resection. Although laparoscopic liver resection (LLR) is often performed for hepatocellular carcinoma or colorectal liver metastasis in expert centers, liver resection is rarely performed for GBC. Reports of LLR for GBC are limited to rare articles and case reports.5–8 Furthermore, there have been very few comparative studies of laparoscopy and open liver resection in patients with GBC. Therefore, we compared the outcomes of LLR for GBC with those of open surgery.
Materials and Methods
This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital, South Korea. We retrospectively analyzed all patients who underwent radical cholecystectomy, including resection of the liver parenchyma of ≥2 cm, between January 2004 and December 2018. In total, 135 patients underwent liver resection for stage II or III GBC. Of these, 79 patients were excluded because the thickness of the liver sections available for pathology was <2 cm. Eventually, 56 patients were enrolled in the study.
Operative procedures
Patients underwent radical cholecystectomy, which included cholecystectomy with en bloc liver resection and lymphadenectomy. If GBC was diagnosed incidentally intraoperatively in frozen pathological sections, complete lymphadenectomy and liver resection were performed. In cases who underwent second-stage surgery, which was performed after postoperative pathological diagnosis of GBC, lymphadenectomy was performed first followed by liver resection.
Liver resection comprised either wedge resection with >2 cm thickness of liver parenchyma or anatomical resection of segments IVB and V. In most cases, liver resection was performed en bloc with the gallbladder after completing lymphadenectomy.
Patients' demographics, clinical characteristics, and pathological, operative, and postoperative data were collected from the hospital's electronic medical reporting system. The median follow-up period was 21.5 months (9–80 months) for open liver resection and 22.5 months (12–50 months) for LLR.
Statistical analysis
To avoid selection bias between the two groups, we used a propensity score model. Matching was performed with a 1:1 ratio. The variables selected included potential confounding variables unrelated to exposure but related to outcome. This model is said to reduce the variance of an exposure effect without increasing the bias. 9 The patients' baseline characteristics, such as age, gender, body mass index, American Society of Anesthesiologists (ASA) score, diabetes mellitus, hypertension, and hyperlipidemia, were the matching factors used. Patients were also matched for tumor size and the number of positive nodes.
The final data analysis was performed with SPSS for Windows, version 20 (IBM-SPSS, Inc., Chicago, IL, USA). Categorical data are presented as frequencies and percentages, whereas continuous data are presented as means and standard deviations, or as medians and ranges for data not normally distributed. The Mann–Whitney U test was used for continuous data and the chi-square test was used for categorical data when two groups were compared. Kaplan–Meier survival curves were plotted for overall survival and disease-free survival. A P value of <.05 was deemed significant.
Results
A total of 135 patients underwent radical cholecystectomy, of which 48 (40.3%) underwent laparoscopic surgery. After 79 patients were excluded because their liver samples for pathology were <2 cm thick, 56 patients were included in this study. Of these, 23 patients underwent laparoscopic surgery and 33 underwent open resection. Table 1 shows the characteristics of the patients in both groups before propensity score matching.
Characteristics of Patients Before Propensity Score Matching
ASA, American Society of Anesthesiologists; BMI, body mass index; GB, gallbladder; N, nodal; T, tumor.
Propensity score matching using a 1:1 model was performed and 12 patients were selected in each group. The patients were matched for demographic characteristics and comorbidities, in addition to tumor size and number of positive lymph nodes. There were no significant differences in the baseline characteristics between the two groups (Table 2). Both groups included two patients in whom GBC was detected incidentally.
Characteristics of Patients After Propensity Score Matching
ASA, American Society of Anesthesiologists; BMI, body mass index; DM, diabetes mellitus; N, nodal; T, tumor.
Surgical outcomes
Anatomical IVB and V resection was performed in two patients in the open group and in one patient in the laparoscopy group (P = .537); the remaining patients underwent a wedge resection of the liver.
The operative times (laparoscopy group versus open group: 237.5 minutes versus 272.5 minutes, respectively; P = .319) and blood loss (300 mL versus 275 mL, respectively; P = .307) were similar in both groups. No patient in the laparoscopy group required a blood transfusion, whereas one patient in the open group required a transfusion (P = .307). The median number of lymph nodes harvested was similar between both groups (P = .910) with a median of 6.5 lymph nodes in the laparoscopic group. There were no intraoperative complications or deaths in either group. The laparoscopy group had a significantly shorter hospital stay (median [range]; 4.5 days [2–12]) than the open group (8 days [5–32], P = .012).
Postoperative outcomes
No patients in either group suffered postoperative bile leakage, intra-abdominal fluid collection, or wound-related complications. Two patients in the open group developed postoperative respiratory complications (P = .140), but no patients in either group experienced major complications.
Long-term outcomes
There were no cases of port-site recurrence in the laparoscopy group. Six patients in the open group and five in the laparoscopic group (P = .682) experienced intra-abdominal recurrence. The 1-year (P = .226) and 3-year (P = .503) disease-free survival rates and the 1-year (P = .269) and 3-year (P = .719) overall survival rates were not significantly different between the two groups (Figs. 1 and 2).

Kaplan–Meier plots of disease-free survival. Color images are available online.
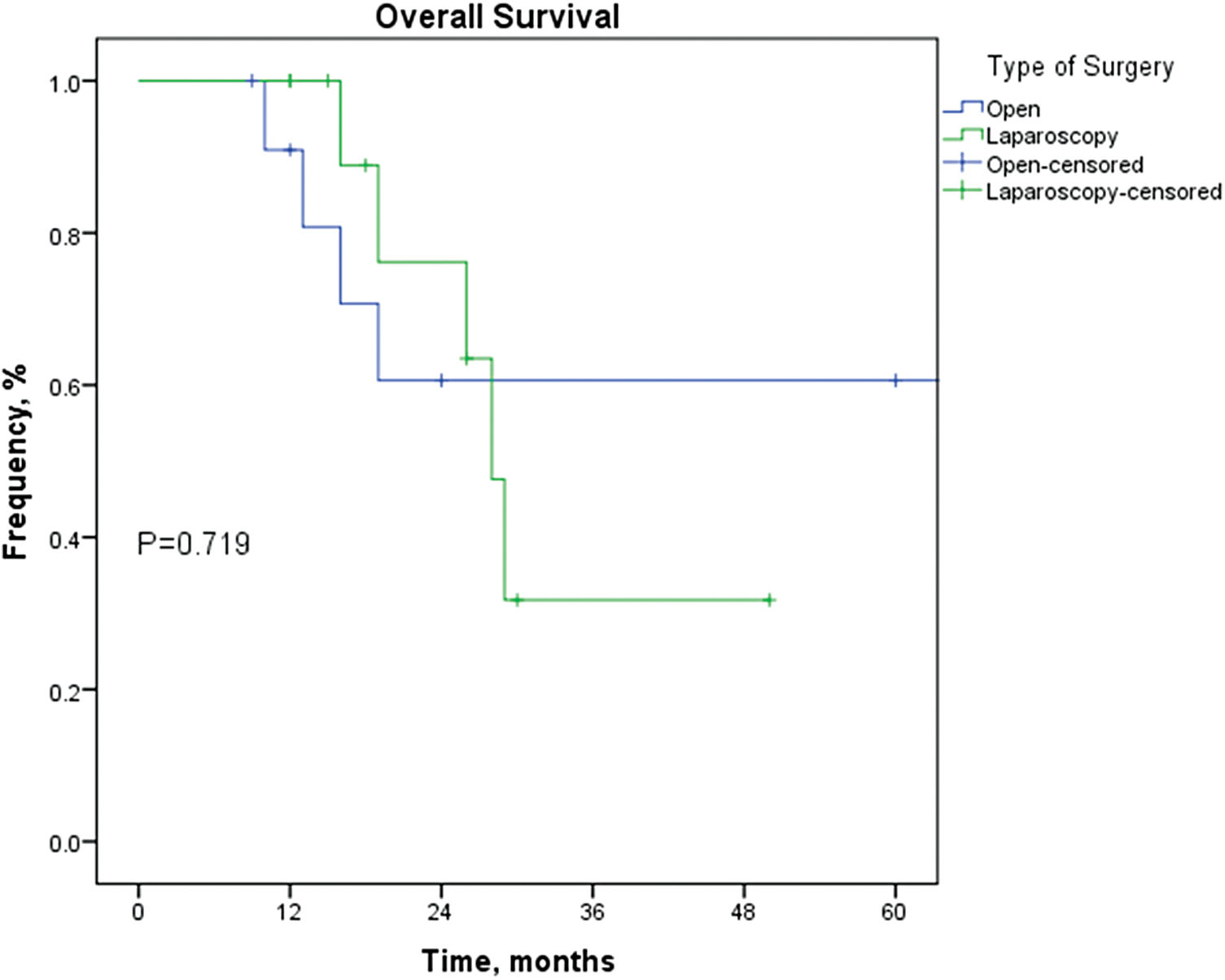
Kaplan–Meier plots of overall survival. Color images are available online.
Discussion
Laparoscopic surgery has become a frequent procedure in many fields. However, the uptake of laparoscopy has been slow in some surgical specialties, particularly laparoscopic surgery for GBC and LLR. The adoption of laparoscopic surgery for GBC has been slow because its technical difficulties increase the risk of gallbladder perforation with bile spillage, port-site metastasis, and inadequate lymph-node dissection. However, several reports have supported the surgical safety of laparoscopy for GBC.10,11 LLR is routinely performed at expert centers for resection of hepatocellular carcinoma and liver metastasis,12,13 but there are few reports of LLR for GBC. 11 Our study is one of the few studies to compare laparoscopy and open surgery for GBC.
In this study, laparoscopic surgery had similar intraoperative outcomes in terms of the operative time and blood loss to those of open surgery. There were no major complications in either group, which confirms that laparoscopic surgery is safe in this setting. However, patients in the open group had respiratory complications, probably related to the long subcostal incision necessary, leading to postoperative pain and atelectasis. Patients in the laparoscopic group had a significantly shorter hospital stay than those in the open group.
There has been concern regarding the oncological safety of laparoscopic surgery for GBC. Although several studies have compared the oncological outcomes between open surgery and laparoscopy for TII GBC, 14 few studies have compared laparoscopic and open extended cholecystectomy with liver resection for GBC. In this study, we found that the oncological outcomes of this procedure were similar to those of open surgery. There was no difference in the number of lymph nodes harvested in the laparoscopic group with both groups dissecting a minimum of six lymph nodes. Many studies of LLR have shown similar oncological outcomes after hepatocellular carcinoma and colorectal liver metastasis.15,16 All these findings suggest that survival is not influenced by the operative method used in these cases.
The aim of liver resection for GBC is to achieve a negative margin with minimal complications. 8 With current advances in LLR, fulfilling this aim can be safely achieved. Liver resection for GBC may involve wedge resection or anatomical resection of segments IVB and V, and studies have reported similar outcomes with both techniques.17,18 Laparoscopic anatomical resection of segments IVB and V is technically challenging, and requires a longer operative time. Laparoscopic wedge resection is a good method for achieving adequate margins as well. Some patients require major liver resection, which can also be completed laparoscopically.19,20
Reports have shown that laparoscopic surgery reduces the adverse immunological responses and improves postoperative recovery. 21 Patient satisfaction after laparoscopic surgery was also reported to be significantly better than after open surgery. 22
There were some limitations to this study. The patient number was small and matching reduced this number further. Furthermore, this was a retrospective study. Therefore, prospective randomized controlled trials are required to further examine the role of laparoscopic surgery in patients with GBC.
In summary, laparoscopic surgery can be safely performed and meets the oncological standards of open surgery, even when liver resection is required. This finding, coupled with the reduced immunological response and better patient satisfaction associated with LLR for GBC, may soon make this the procedure of choice in expert centers.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.