
Abstract
Background:
The new da Vinci single port (SP) robotic platform has great appeal for pediatric surgery. To assess its efficacy and identify potential challenges, 7 adolescents underwent SP cholecystectomy.
Materials and Methods:
The surgeon controls three fully wristed elbowed instruments, and the first fully wristed da Vinci endoscope through a single 2.5 cm cannula. Instruments can reach 24 cm deep and triangulate distally. Instruments can also reach anatomy anywhere within 360° of port placement. A vertical incision was made through the umbilicus for port access. The cystic duct and cystic artery were dissected, clipped, divided, and hook cautery was used to remove the gallbladder. Patient characteristics and outcomes were collected and analyzed.
Results:
Patients were American Society of Anesthesiologists (ASA) classes I, II, and III; mean age was 17 years; mean weight was 72 kg; and 6 of 7 patients were female. There were no fatalities, and there were no returns to the operating room. Mean estimated blood loss was 2 mL and mean case duration was 126 minutes. Five out of seven patients were treated as outpatients, and none of them required narcotics on discharge. One patient reported bilateral shoulder pain 1 day postoperatively and was taking hydrocodone/acetaminophen at the time of 13-day follow-up.
Conclusions:
SP robotic platform cholecystectomy in adolescents appears to be safe and effective. The wristed movement of the robotic instruments improves surgeon dexterity, and the single incision hidden in the contour of the umbilicus provides good cosmesis. This series sets an exciting precedent and provides a glimpse of what is possible in pediatric robotic surgery. Clinical Trial Registration number 2014-0396.
Introduction
The widespread adaptation of robotic surgery in children has proved challenging. Although the first robotic surgery on a child was reported in April 2001, 1 robotic surgery within the spatially constrained workspaces of a child's habitus makes traditional platforms less suitable. The single port (SP) da Vinci surgical system, however, appears to make robotic surgery more feasible in pediatric populations.
The SP is the latest advancement from da Vinci surgical systems. A single 2.5 cm cannula allows the surgeon to control three instruments and the da Vinci camera. The instruments are fully wristed and the camera is the first fully wristed da Vinci endoscope. In addition to being fully wristed, the instruments have mid instrument flexion and can be manipulated immediately beyond the end of the cannula. This allows SP instruments to reach up to 24 cm deep, target anatomy anywhere within 360° of port placement, and triangulate within a space as restricted as 7 cm in diameter once deployed. The combination of these capabilities provides narrow deep surgical access, 2 making the SP platform highly applicable for pediatric surgery.
Seven adolescents underwent SP robotic cholecystectomy at the University of Illinois at Chicago. These procedures and their outcomes were evaluated to assess feasibility, efficacy, and identify potential challenges.
Materials and Methods
The University of Illinois at Chicago Institutional Review Board gave approval for this study. The research protocol number is 2014-0396 (Fig. 1).

Patient was prepped and draped with single port through the midline of the umbilicus. Color images are available online.
Patients were placed supine and a small incision was made through the midline of the umbilicus, through all layers of the abdominal wall, and into the peritoneal cavity. The robotic single port was introduced and the peritoneum was insufflated. The neck of the gallbladder was grasped for retraction as the duct and vessels were isolated, clipped, and divided (Fig. 2). Hook cautery was used to dissect the gallbladder from its bed (Fig. 3). Suction and a 5 mm EndoCatch were placed directly through an instrument channel. No additional instruments or ports were required. The robotic instruments and the single port were then removed. The fascia was closed using 0 polydioxanone suture. The incision was closed in layers and skin glue was applied over the incision (Fig. 4).
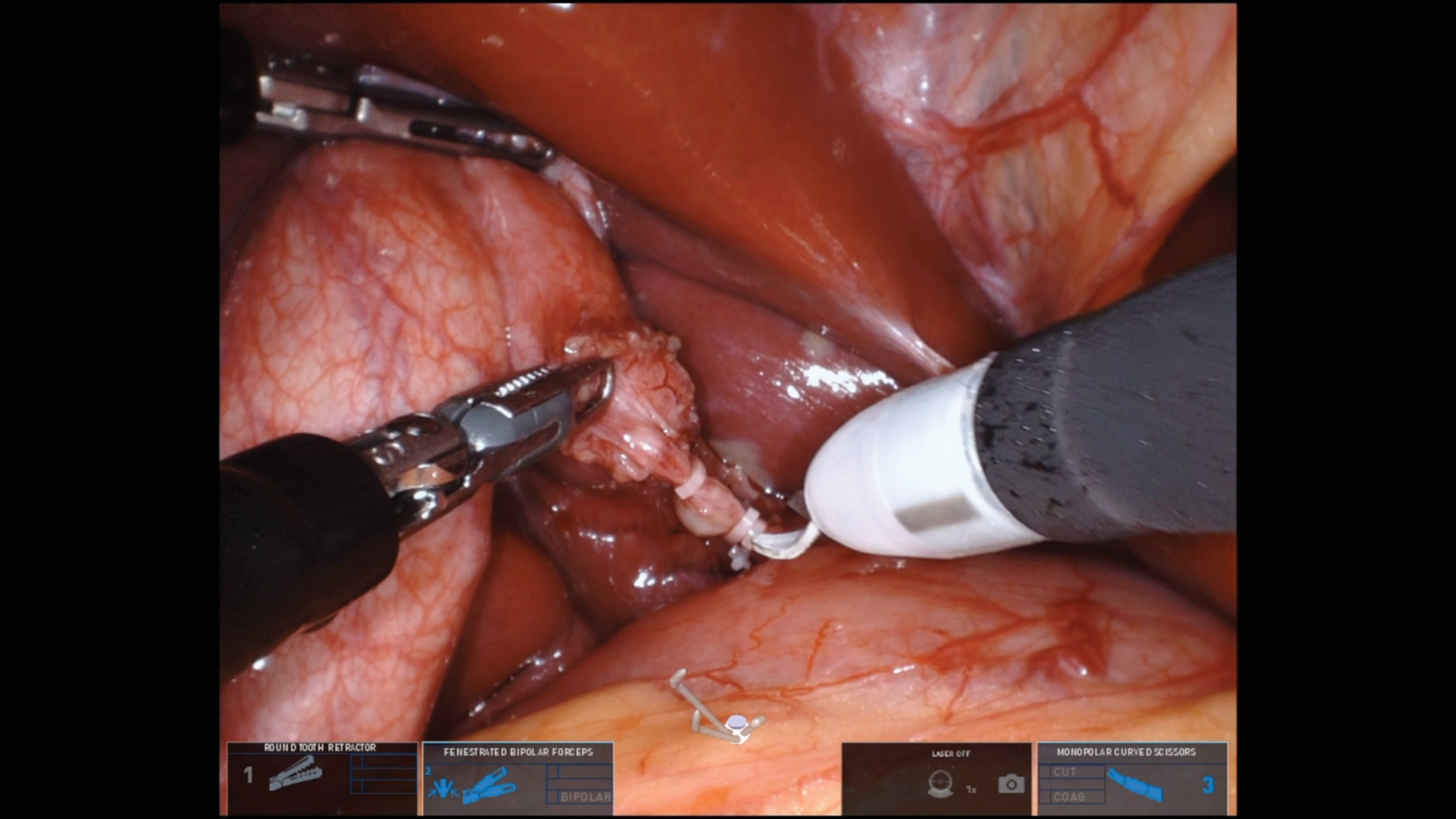
Neck of the gallbladder grasped for retraction as the duct and vessels were isolated, clipped, and divided. Color images are available online.

Dissection of the gallbladder from its bed with hook cautery. Color images are available online.

Single port insertion site immediately postoperatively. Color images are available online.
Key demographic information and patient outcomes were collected in a retrospective chart review and results were analyzed.
Results
Of these 7 patients, 6 were female, and the mean age was 17 years old. Patients were American Society of Anesthesiologists (ASA) classes I, II, and III, and the mean weight was 72 kg. There were no fatalities, and no returns to the operating room. The mean estimated blood loss was 2 mL, and the mean case duration was 126 minutes. In total, 5 of 7 patients were treated as outpatients, and none of them required narcotics on discharge. One patient reported bilateral shoulder pain 1 day postoperatively and was taking hydrocodone/acetaminophen at the time of 13-day follow-up. The 2 patients with overnight stays were sickle cell patients, 1 of whom reported a superficial wound infection. This superficial wound infection resolved with a 7-day course of clindamycin twice daily.
Discussion
Open and laparoscopic approaches are both alternatives to robotic cholecystectomy. Laparoscopic and robotic surgeries share the same relative and absolute contraindications. These include the inability to tolerate pneumoperitoneum, uncorrectable coagulopathy, abdominal compartment syndrome, abdominal wall infection, and previous extensive abdominal surgery. 3
Robotic surgery is more costly than traditional approaches but the increased functionality gives the experienced robotic surgeon more tools to perform an operation. In addition, traditional robotic surgery requires multiple trocar sites, whereas SP robotic surgery utilizes one incision—providing improved cosmesis. Furthermore, patients reported limited pain with a prompt return to full activity.
Conclusion
SP robotic cholecystectomy in adolescents appears to be safe and successful, even in our sickle cell population. The wristed movement of the robotic instruments improves the surgeon's dexterity and the single incision is concealed in the contour of the umbilicus, yielding an excellent cosmetic result. The cost, procedure duration, and long-term complications should all be further considered, but this series sets an exciting standard for pediatric robotic surgery, demonstrating what is ultimately possible on the SP robotic platform.
Footnotes
Authors' Contributions
G.K. was involved in original draft/project administration. A.G., T.S., M.R., N.K., and T.L. took care of review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
Research was funded by the University of Illinois at Chicago Department of Surgery.