
Abstract
Background:
Residual postoperative pneumoperitoneum (RPP) can be confused with postoperative complications. Our aim was to study RPP characteristics in pediatric patients.
Materials and Methods:
Prospective study in children with noncomplicated appendicitis, from July to December 2019, divided into open appendectomy (OA) or laparoscopic appendectomy (LA). Abdominal ultrasounds were performed daily to assess RPP. Demographic, surgical data, and RPP characteristics were analyzed.
Results:
Forty-one patients (63% male) aged 9.8 ± 2.9 years were included: 19 had OA and 22 LA. RPP was present in 90.9% of LA patients versus 21.1% of OA (P < .001). RPP disappeared by the postoperative day (POD) 2, in all OA patients. RPP was present in 90.9% of LA patients in POD 1, 53.8% on POD 2, 25% on POD 3, and in no patient from POD 4. RPP prevalence was not associated with surgical duration, age, gender, or type of appendicitis. RPP was associated with pain radiating to the shoulders (PRS) (P = .018), with a sensitivity of 50.0% and specificity of 88.23% for diagnosis.
Conclusions:
Surgical approach was the main factor associated with RPP persistence. PRS in the physical examination may be helpful for diagnosis when RPP is suspected. The persistence of RPP beyond POD 4 is uncommon, and should be considered when making decisions.
Introduction
The finding of pneumoperitoneum in the imaging test during the postoperative period can be a challenge for pediatric surgeons, both to achieve a correct diagnosis and to establish a proper therapeutic approach. Pneumoperitoneum can be a direct consequence of complications derived from the surgery itself (intestinal perforation, anastomotic leakage, or intra-abdominal abscess), but it may also represent as a residual postoperative pneumoperitoneum (RPP) from either CO2 insufflation during laparoscopic procedures or air entry into the peritoneal cavity during open surgery.1–4
It is obviously important to differentiate these two entities (RPP or pathological pneumoperitoneum) to establish the therapeutic approach, which may range from expectant management to exploratory laparotomy or laparoscopy. It has been reported that ∼5%–15% of postoperative pneumoperitoneum cases are not associated with intestinal perforation, so these patients may be candidates for conservative treatment, who do not require unnecessary further interventions.1,5
Different studies in adult patients have shown that the persistence of postsurgical pneumoperitoneum during the later postoperative period has been associated with a greater need for surgical reintervention.2,3 Some authors have attempted to establish, with variable results, the cutoff point at which pneumoperitoneum after surgery should no longer be considered as residual but rather as pathological and secondary to a possible postsurgical complication, not only in humans2,3,6–10 but also in experimental animals.11,12 However, no studies have analyzed this question in pediatric patients after both open and laparoscopic surgery.
The aim of this article is to establish the duration of RPP in pediatric patients and to analyze associated clinical and surgical features in both open and laparoscopic surgery.
Materials and Methods
Study design
A prospective observational study was performed with patients <18 years of age diagnosed with noncomplicated acute appendicitis in our center who underwent appendectomy, either open or laparoscopic, between July and December 2019.
Patient selection was carried out through consecutive sampling and they were divided into two groups according to the surgical approach: open appendectomy (OA) or laparoscopic appendectomy (LA). For patients undergoing OA, a Rocky-Davis incision was made. In patients undergoing LA, a three-port LA was performed (two 5 mm port and one 10 mm port), cutting the vermiform appendix between two endoloops and taking it out with an endobag. The pneumoperitoneum was instilled with an intra-abdominal CO2 pressure of 12–15 mmHg and it was attempted to be removed mostly of it by opening the trocars valve at the end of surgery. The selection of the surgical approach depended on the surgeon preference.
To assess postoperative pneumoperitoneum, a daily abdominal ultrasound was performed after surgery in all patients included in the study until the resolution of the pneumoperitoneum or until discharge. Inclusion in this study in no case implied a change in the treatment protocol of our center or discharge criteria.
Following institutional guidelines, the study protocol and the informed consent form were approved by the Ethics Committee of Clinical Research. Before being included, each child's parents or legal guardians signed the informed consent form.
Patients with an associated pathology, those who developed postoperative complications or those whose parents or legal guardians refused to participate, were excluded from the study. Patients with postoperative complication after appendectomy (such as abdominal abscess) were excluded to avoid bias, as the aim of the study was to determine the behavior of residual pneumoperitoneum not associated with complications.
Study variables
The following variables were extracted from the patients' medical records:
Demographic variables: age, gender, weight, and weight-for-age percentiles (according to World Health Organization child growth standards
13
). Clinical features: type of acute appendicitis (phlegmonous, gangrenous, or appendicular peritonitis) according to findings during surgery, postoperative clinical symptoms (presence or not of pain radiating to the shoulder [PRS]), and postoperative ileus (considering its finalization when the patient presented with bowel movement or bowel sounds). Surgical features: type of surgical approach (OA or LA) and surgical duration (minutes). Ultrasound findings: ultrasounds were performed in all cases with the patient seated with the bed headboard inclined at 45°. Pneumoperitoneum was assessed in right subcostal and subxiphoid area (between the hepatic rim and the abdominal wall). The parameters analyzed were presence of RPP, its quantity (mild, moderate or abundant) established by subjective ultrasound criteria (defined in Fig. 1), as well as RPP duration (postoperative days [PODs]). All ultrasounds were performed by the same person (a radiologist experienced in pediatric abdominal ultrasound).

Quantity of pneumoperitoneum. Color images are available online.
Statistical analysis
A descriptive study of the sample was performed first. Quantitative variables were compared, after a normality study, with the Student's t-test (on variables with normal distribution) or the Mann–Whitney U test (on variables that did not follow a normal distribution). To compare discrete variables, the chi-square test or the Fisher's exact test were used, as appropriate. The survival charts were calculated with the Kaplan–Meier method, making the corresponding comparisons with the log-rank test (Mantel–Cox).
Data were analyzed using the IBM SPSS Statistics 22.0 statistical package. Results with a value of P < .05 were considered significant. All intervals were calculated with 95% confidence.
Results
Patients and groups characteristics
During the 6-month recruitment period, 48 patients were considered. Seven patients were excluded (Fig. 2 shows patient flowchart selection process). Finally 41 patients were included and divided into two groups depending on the surgical approach: 19 underwent OA and 22 underwent LA.
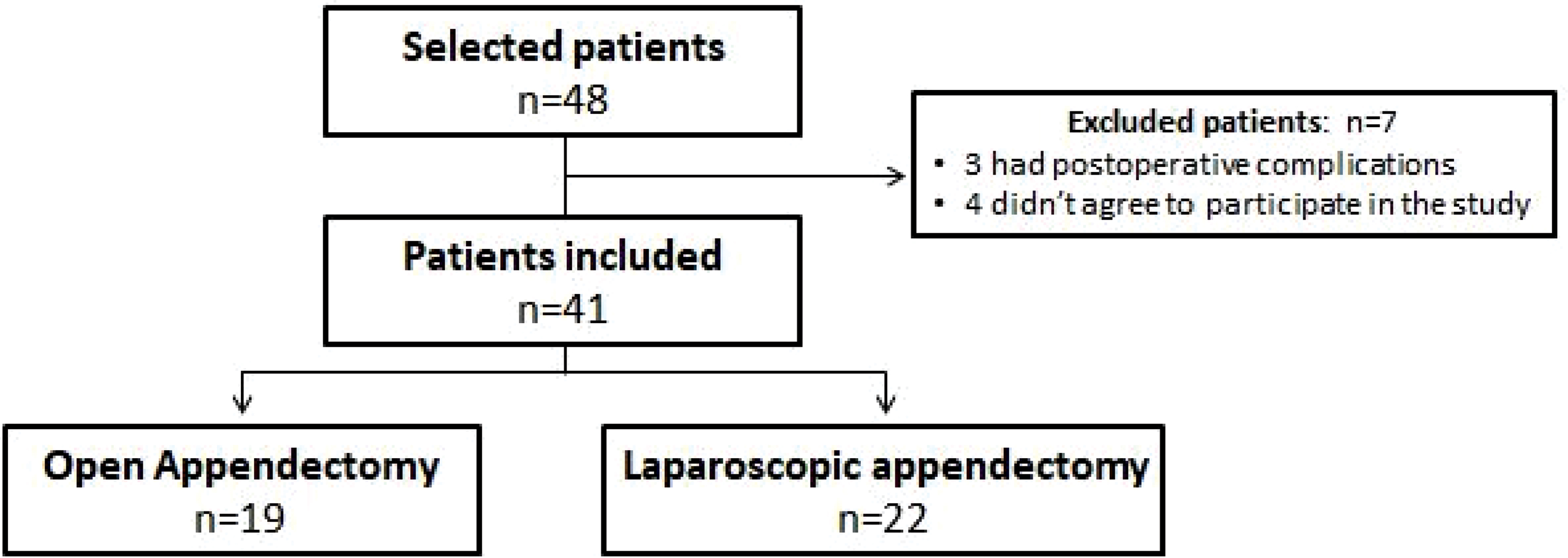
Patient flowchart.
Twenty-six were male (63.4%) and 15 were female (36.6%). Mean age was 9.8 ± 2.9 years (range 5–15 years), with a mean weight of 37.4 ± 13.5 kg.
No significant differences in appendicitis type distribution, weight-for-age percentile distribution or patient gender were found between the OA and LA groups. However, weight (P = .007), age (P < .001), and surgical duration (P < .001) were higher in the LA group. The remaining data for the descriptive analysis are shown in Table 1.
Analysis of the Sample
Bold p values considered statistically significant (p < 0.05).
LA, laparoscopic appendectomy; OA, open appendectomy; SD, standard deviation.
Prevalence, quantity, and factors associated with RPP
RPP was observed during POD 1 in 20 patients (90.9%) in the LA group, being significantly more frequent than in the OA group, in which 4 (21.1%) patients had RPP (P < .001).
All 4 patients (100%) in OA group presented mild pneumoperitoneum (grade 1). In the LA group, pneumoperitoneum presented as mild (grade 1) in 10 patients (50%), moderate (grade 2) in 9 patients (45%), and abundant (grade 3) in 1 patient (5%). Data about quantity of RPP are summarized in Figure 3.
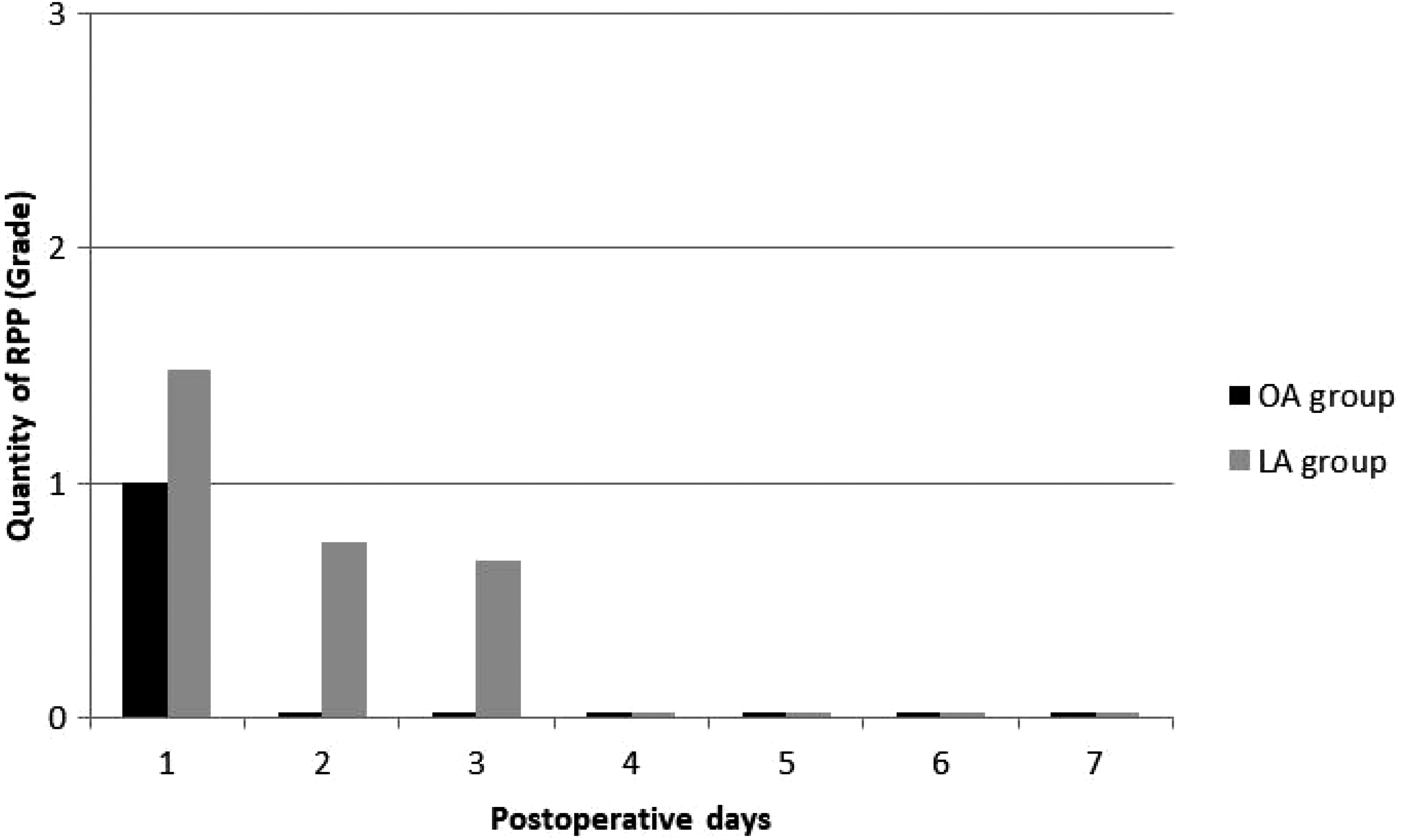
Evolution of the mean quantity of RPP. RPP, residual postoperative pneumoperitoneum.
No association between RPP and gender, operative findings (phlegmonous, gangrenous, or peritonitis) or patient weight-for-age percentile was found in either the OA or the LA group (Table 2). Despite this, persistence of RPP was less frequently observed in patients with a weight-for-age percentile ≥90.
Influence of Other Clinical and Demographic Factors in Residual Postoperative Pneumoperitoneum
Bold p values considered statistically significant (p < 0.05).
LA, laparoscopic appendectomy; OA, open appendectomy; RPP, residual postoperative pneumoperitoneum.
There were no differences in surgical time between patients with and without RPP in the OA group (27.50 ± 8.66 minutes versus 34.93 ± 8.95 minutes, respectively; P = .16) or in the LA group (61.42 ± 24.73 minutes versus 114.0 ± 0.01 minutes, respectively; P = .053). Also, there were no differences in the mean age of patients with and without RPP in the OA group (10.25 ± 2.22 years versus 8.64 ± 2.71 years, respectively; P = .296) or the LA group (10.89 ± 2.81 years versus 10.00 ± 0.01 years, respectively; P = .89).
RPP time duration
The mean time until the resolution of RPP (Fig. 4) was 2.00 ± 0.01 days after surgery in the OA group, compared with 2.45 ± 0.17 days in the LA group (P = .22).
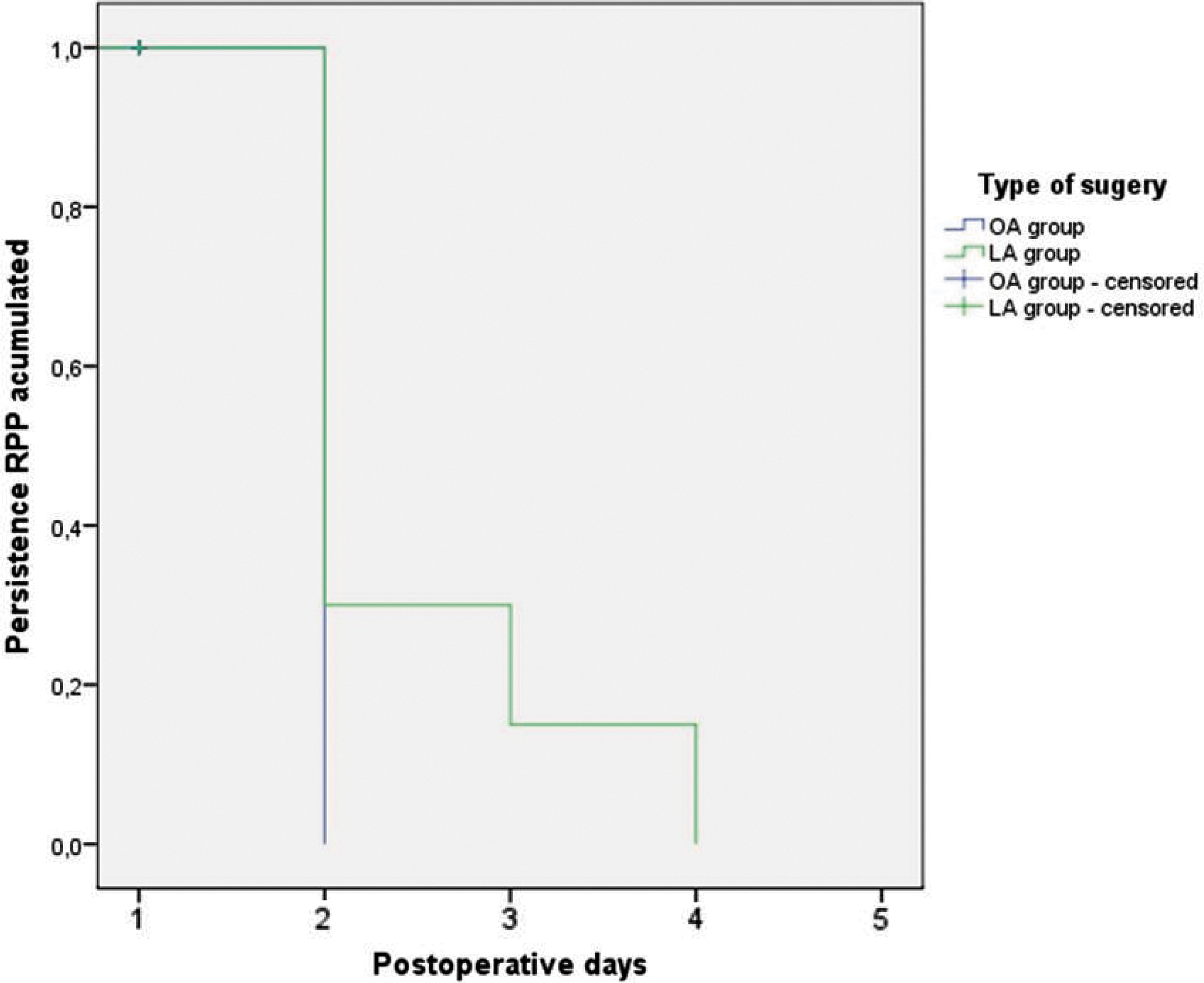
RPP disappearance (Kaplan–Meier method). RPP, residual postoperative pneumoperitoneum. Color images are available online.
All OA group patients (100%) with RPP observed on POD 1 presented spontaneous resolution on POD 2. In the LA group, RPP persisted in 7 patients (53.8%) on POD 2 and in 3 (25%) on POD 3, with no RPP detected in any patient on POD 4 (Fig. 5).

Persistence of RPP. RPP, residual postoperative pneumoperitoneum.
Clinical symptoms associated with RPP
The main clinical symptom statistically associated with RPP was radiating pain to the shoulder (P = .018), which was observed in 14 patients (13 [92.8%] in the LA group), of whom 12 (85.7%) had RPP in the abdominal ultrasound study. Among the remaining 27 patients who did not report PRS, 12 (44.4%) had RPP versus 15 (55.6%) who did not. The remaining data are summarized in Table 3.
Association Between Pain Radiating to the Shoulders and Residual Postoperative Pneumoperitoneum
LA, laparoscopic appendectomy; OA, open appendectomy; PRS, pain radiating to the shoulder; RPP, residual postoperative pneumoperitoneum.
This symptom was much more frequent among patient with moderate–severe RPP (70%) than in patients with mild RPP (38.5%; P = .004).
The sensitivity of this clinical sign for the diagnosis of RPP was calculated at 50.0%, with a specificity of 88.2%.
Outcomes
No patient in this study required reoperation. All patients were discharged according to their clinical symptoms, evolution, and type of appendicitis following our institution guidelines.
Discussion
This prospective study demonstrates that RPP appears more frequently in those children undergoing a laparoscopic approach and tends resolve itself around the POD 3–4, being infrequent beyond this date. Neither age, gender, weight-for-age percentile, surgical time, nor type of appendicitis seems to influence the prevalence or duration of this RPP.
Although the test used for the diagnosis of RPP in this study was abdominal ultrasound, most of the previous articles used abdominal radiography and/or computed tomography, with the latter being the test with the greatest sensitivity, especially in patients with obesity.10,14 Published literature about the use of ultrasound to detect pneumoperitoneum reports a sensitivity of ∼90% and a specificity of between 83.5% and 100%,15,16 so we consider abdominal ultrasonography a valid or complementary tool for the diagnosis of pneumoperitoneum. 17 This is important, especially in a pediatric population, because decreased the amount of radiation required to carry out the diagnosis of RPP and follow-up of these patients.
Previous experience in adult patients has shown that the duration of RPP after open or laparoscopic surgery is ∼7 days,7–9 and it may persist even up to 6–8 weeks after the surgery.1,6,18,19 In this study, we found no patients with residual RPP beyond POD 4, with a mean time to resolution of 48 hours, similar to previously published results in both experimental animals11,12 and in children after open surgery procedures, 20 where the disappearance of RPP was estimated to occur around POD 2–3 too.
Some factors could influence the duration of the RPP. Several authors have found RPP more frequently in patients with an asthenic habit or children with a weight-for-age percentile ≤37,20,21 being these findings questioned due to a reported decreased sensitivity of radiography to detect RPP in the obese. 9 In our study, no significant increase in the presence of RPP in patients with a low weight-for-age percentile was detected, although we found a higher incidence of RPP in patients with percentile <90.
Likewise, neither age nor gender appears to have any influence on the prevalence or duration of RPP.9,20 A longer operating time and open approach have traditionally been associated with a greater presence of RPP,20,21 but, again, our results do not support these findings, as the highest incidence of RPP was observed in patients undergoing LA. The type of appendicitis does not appear to influence the presence of RPP, being similar for phlegmonous, gangrenous, or appendicular peritonitis, concurring with the results of Ein et al. 20
Predisposing factors and duration of the RPP are key elements in decision-making for pediatric surgeons, since several studies have shown that the longer the time between the detection of the pneumoperitoneum and the original surgical procedure, the greater the probability that it is secondary to a postoperative complication requiring reoperation.
Likewise, a shorter time until detection of the pneumoperitoneum has been associated with RPP and good evolution with conservative treatment, avoiding unnecessary laparotomies or exploratory laparoscopies. Other factors associated with the need for reintervention have been the presence of fever, increased pneumoperitoneum over time or leukocytosis (>10.500/μL) on the blood test.2,3 Therefore, the POD, associated symptoms, and the analytical parameters are the basic elements that the pediatric surgeon must take into account when establishing the possible origin of the postoperative pneumoperitoneum and the therapeutic approach to follow.
The main limitations of this study are the absence of an objective validated scale to measure RPP, as well as the absence of a complementary X-ray study in each patient to compare with ultrasound findings. Additional investigations that collect information about RPP in newborns as well as open surgeries that require larger incisions will improve our knowledge about postoperative pneumoperitoneum.
Conclusion
Surgical approach is the main determinant of the persistence and quantity of RPP after appendectomy. This condition is more frequent and abundant after a laparoscopic approach. PRS is a guiding symptom in the physical examination of the patient with suspected RPP and it is associated with a greater quantity of free intraperitoneal gas. Moreover, the persistence of RPP beyond POD 4 is uncommon, when this occurs it should be considered together with other clinical and analytical findings to establish the diagnosis and therapeutic management of the postoperative pneumoperitoneum.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.