
Abstract
Objective:
To compare the outcomes of secondary minimally invasive pyeloplasty (MIP) versus primary MIP for the patients with ureteropelvic junction obstruction (UPJO).
Materials and Methods:
We searched all the literature of PubMed, Web of Science, EMBASE, and Cochrane Library comparing secondary MIP and primary MIP and performed a systematic review and meta-analysis.
Results:
We included 15 studies involving 1637 patients with 1371 in the primary MIP group and 266 in the secondary MIP group. There were no significant differences in length of hospital stays, and the risk of hematuria, urinary tract infection, intestinal obstruction, stent complications, and overall complications (P > .05). Comparing with the secondary MIP group, the primary MIP group has shorter operative time (mean difference [MD] = −36.91 minutes, 95% confidence interval [CI]: −50.21 to −23.62, P < .00001), less estimated blood loss (MD = −16.70 mL, 95% CI: −31.60 to −1.80, P = .03), lower risk of urinary leakage and injury of blood vessel (relative risk [RR] = 0.32, 95% CI: 0.11–0.93, P = .04) (RR = 0.10, 95% CI: 0.02–0.61, P = .01), and higher success rate (RR = 1.07, 95% CI: 1.02–1.11, P = .003). The robot-assisted pyeloplasty is superior to the laparoscopic pyeloplasty in controlling the amount of blood loss in the secondary operation.
Conclusions:
Considering the poorer outcomes of secondary surgery, we believe that special attention should be paid to not missing crossing vessels, and it would be more prudent to perform a more definitive procedure with pyeloplasty instead of endopyelotomy for primary UPJO.
Introduction
Ureteropelvic junction obstruction (UPJO) is a common disease of upper urinary tract obstruction. In the past, open dismembered Anderson Hynes pyeloplasty is the gold standard for the treatment of UPJO. Since laparoscopic pyeloplasty (LP) was first reported by Schuessler et al. in 1993 as a successful case in the treatment of this disease, it has been continuously promoted and improved.
1
Laparoscopic or robot-assisted pyeloplasty has become the first choice for the treatment of
In addition, although the success rate of endopyelotomy is lower than that of pyeloplasty, it is also widely used in clinical practice due to its advantages of minimally invasive and repeatability.4,5 Despite the high success rate of various treatments, 11%–33% of patients with recurrent
Methods of re-intervention include double-J tube implantation, endopyelotomy, retrograde endoscopic balloon dilation, and secondary open, laparoscopic, or robotic pyeloplasty.8–11 Minimally invasive LP is more preferred by scholars because of its higher surgical success rate than endourological minimally invasive surgery and its minimally invasive advantages compared with open surgery.12–15
Secondary minimally invasive pyeloplasty (MIP) has reported a high success rate in some institutional studies. 16 However, some researchers believe that the secondary LP is more difficult, with higher complications and lower success rate compared with the primary operation due to the complicated local anatomy and aggravating adhesion after the initial treatment. Unfortunately, there is still not enough literature comparing the outcomes of the two procedures. Therefore, we conducted a systematic review and meta-analysis to evaluate the feasibility and safety of secondary MIP by comparing preoperative, intraoperative, and postoperative parameters and success rates with primary MIP.
Materials and Methods
We did this systematic review and meta-analysis following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 17 This study was approved by local institutional review boards (IRB). The meta-analysis was registered on PROSPERO (PROSPERO Registration No. CRD42021282495).
Search strategy
We systematically searched all the literature of PubMed, Web of Science, EMBASE, and Cochrane Library comparing secondary MIP and primary MIP in the treatment of
Inclusion and exclusion criteria
Inclusion criteria: (1) the original studies that compared the safety and clinical efficacy of primary with secondary MIP including LP and robot-assisted pyeloplasty and published in English-language journals were included. (2) Indicators of safety and clinical efficacy are mainly operation time, estimated blood loss, conversion rate, length of hospital stays, complications, and success rate.
Exclusion criteria: (1) studies comparing MIP with other surgical modalities such as endopyelotomy or open laparoscopy; (2) nonoriginal studies (vitro studies, animal studies, letters to editors, editorials, review articles, case reports, and conference abstract); (3) studies with no comparison group; (4) studies with poor comparability between groups due to lack of demographic contrast; (5) data incomplete and cannot be obtained by contacting authors of the original studies; (6) studies from nonrepresentative populations or with explicitly convenient samples (lack of institutional individuals, vulnerable groups, and sample selection based on investigator interest).
Screening
Studies from relevant reviews and bibliographic lists of the original articles were also manually searched. Bibliographic management software EndNote 20 was used to manage the references to exclude repeated citations. Titles, abstracts, and keywords were selected by two reviewers according to the above criteria. After preliminary selection of titles, abstracts, and keywords, the full text would be evaluated by the same two reviewers.
Data extraction
Two authors will independently extract data. Any disagreement will be resolved by discussion until consensus is reached by consulting a third author. The following data will be extracted: author, year of publication, the country where the study was conducted, study design, number of included patients, procedures, mean age, sex, laterality, presence of a crossing vessel, operative time, estimated blood loss, conversion rate, length of hospital stays, various complications and overall complications rate, follow-up period, and success rate.
Quality assessment
The quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS). Items of NOS were based on three quality parameters (selection, comparability, and outcome). Each item on the scale was scored from 1 point to score up to 2 points. Most studies consider a score of 7 or above to be of high quality. Studies with a score between 5 and 6 are considered of medium quality, and any study with a score less than 5 is considered of low quality.
Statistical analyses
All statistical analyses were performed by Review Manager Version 5.3 (The Nordic Cochrane Centre; The Cochrane Collaboration, 2014). For dichotomous variables, we used the number of events and a total number of participants per treatment group to calculate the relative risk (RR) and the corresponding 95% confidence interval (CI). For continuous variables, we used mean difference (MD) for analysis. If there is no or low heterogeneity (I 2 < 50%), the fixed effect model is selected; on the contrary, when there is significant heterogeneity (I 2 > 50%), the random effect model is selected. Moreover, to explore sources of heterogeneity, subgroup analysis was performed according to operational procedures. P < 0.05 was defined as statistically significant.
Results
Study selection process
One thousand three hundred six studies are retrieved from four databases, namely PubMed (508), Embase (445), Web of Science (333), Cochrane Library (20), with 412 duplicate reports. There are no additional records from other sources. After browsing the titles, abstractions, and keywords, there are 43 remaining for full-text review. Then, 28 studies were excluded because they did not meet the inclusion and exclusion criteria. In the 28 studies, 17 studies were excluded because of the lack of a control group consisting of primary MIP, 8 studies were excluded because grouping criteria do not match, 2 studies18,19 were excluded due to lack of baseline data comparison and poor intergroup comparability, and 1 study
20
was excluded because 3 of 17 patients in the case group had atypical anatomical horseshoe kidney rather than recurrent
Finally, we included 15 studies21–35 involving 1637 patients with 1371 in the primary MIP group and 266 in the secondary MIP group for systematic review and meta-analysis. Figure 1 shows the PRISMA flowchart for the inclusion and exclusion study.

The PRISMA flowchart for the inclusion and exclusion study. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Study characteristics
Table 1 presents the study characteristics and methodology for the 15 studies21–35 included in the meta-analysis. Most of the included studies21–31 (11/15, 73.3%) were published since 2015. Of the 15 studies included, the authors are mainly from the United States,21,23,25,28,29,32–35 China,22,24 India, 31 Brazil, 26 Egypt, 27 and Japan. 30 The remaining 14 studies21–32,34,35 were retrospective except for 1 study 33 combined with retrospective and prospective. Fourteen studies21–24,26–35 were followed for an average of more than 1 years except for 1 study, 25 9 studies22,24,26–28,30–32,34 were followed for an average of more than 2 years, with the minimum follow-up time being 1 month after surgery. 30
The Study Characteristics and Methodology for the 15 Studies Included in the Meta-Analysis
Bold data indicate significance between the groups.
Only overall results were reported.
Article only reported the details of previous pyeloplasty procedures among the 12 patients with crossing vessels in the secondary robot-assisted pyeloplasty group.
CRP, combined with retrospective and prospective; LP, laparoscopic pyeloplasty; MIP, minimally invasive pyeloplasty; M/F, male/female; NA, not available; NOS, Newcastle–Ottawa Scale; OP, open pyeloplasty; P/S, primary versus secondary; RAP, robot-assisted pyeloplasty; R/L: right/left.
LP was performed in six of our studies,26–31 and robot-assisted pyeloplasty was performed in nine of our studies.21–25,32–35 Two hundred four patients were secondary to previous pyeloplasties among 266 participants in the secondary MIP group. Of the 15 studies, Sivaraman et al. 32 only reported the details of previous pyeloplasty procedures among the 12 patients with crossing vessels in the secondary robot-assisted pyeloplasty group. NOS is between 7☆ and 9☆.
Meta-analysis results
Operative time
We included a total of 1323 patients in 13 studies21–23,25–31,33–35 analyzing operative time: 1092 in the primary MIP group and 231 in the secondary MIP group. Subgroup analysis showed that the average operative time of primary LP (Z = 4.11, P < .0001, MD = −38.45 minutes, 95% CI: −56.80 to −20.10) and RAP (Z = 3.38, P = .0007, MD = −35.69 minutes, 95% CI: −56.38 to −15.00) was shorter than that of secondary LP and RAP. Overall, the average operative time in the primary MIP group was shorter than that in the secondary MIP group (Z = 5.44, P < .00001, MD = −36.91 minutes, 95% CI: −50.21 to −23.62). The random effect model was adopted because of the high heterogeneity (I 2 = 69%; Fig. 2 and Table 2).
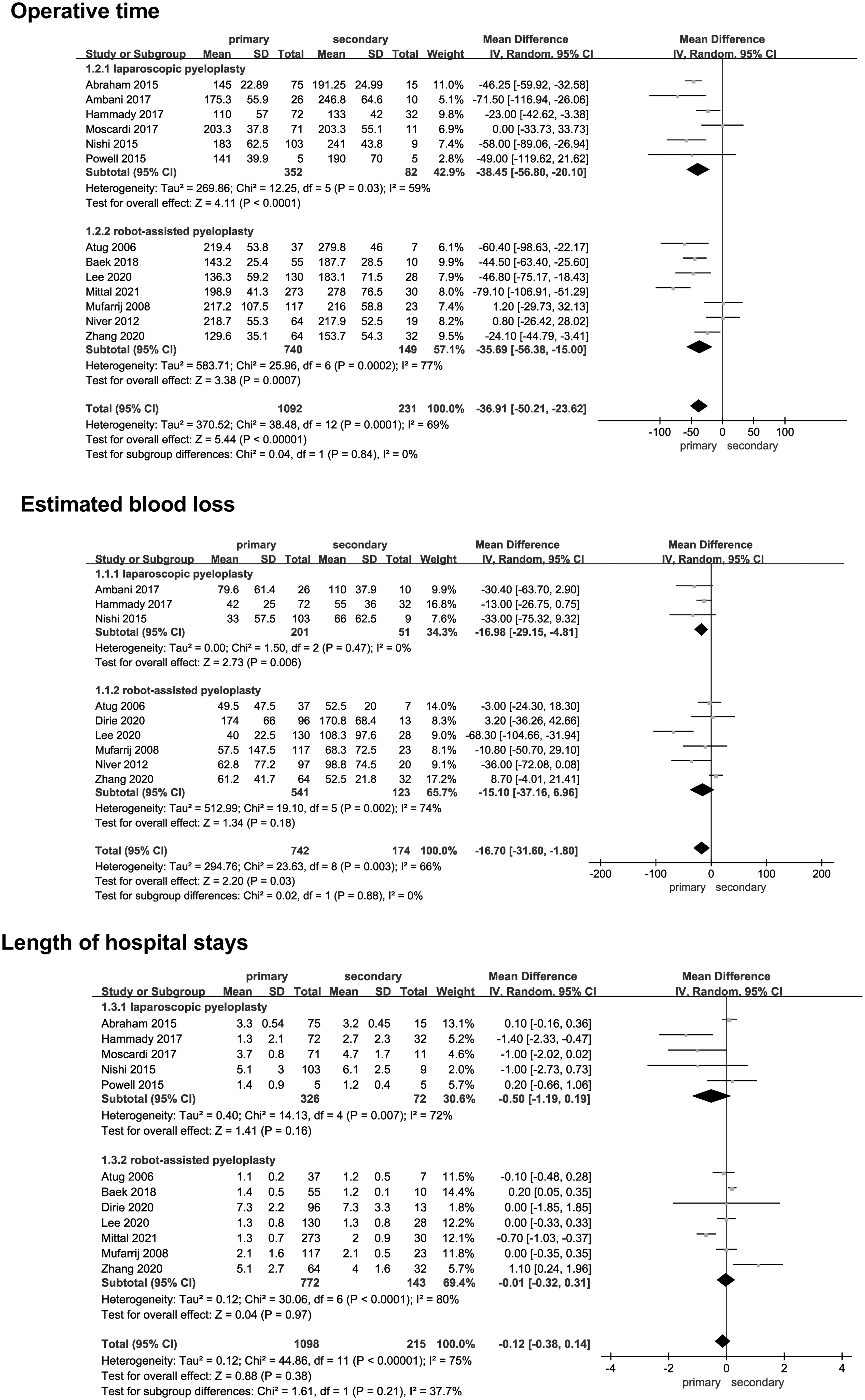
The perioperative results of primary versus secondary minimally invasive pyeloplasty.
Meta-Analysis Summary (Primary versus Secondary Minimally Invasive Pyeloplasty)
CI, confidence interval; LP, laparoscopic pyeloplasty; MD, mean difference; P/S, primary versus secondary; RAP, robot-assisted pyeloplasty; RR, relative risk.
Estimated blood loss
We included a total of 916 patients in 9 studies22–24,27,28,30,33–35 analyzing estimated blood loss: 742 in the primary MIP group and 174 in the secondary MIP group. Subgroup analysis showed that the average estimated blood loss of primary LP was less than that of secondary LP (Z = 2.73, P = .006, MD = −16.98 mL, 95% CI: −29.15 to −4.81), whereas there were no significant differences between the primary RAP and secondary RAP (Z = 1.34, P = .18, MD = −15.10 mL, 95% CI: −37.16–6.96). Overall, estimated blood loss in the primary MIP group was less than that in the secondary MIP group (Z = 2.20, P = .03, MD = −16.70 mL, 95% CI: −31.60 to −1.80). The random effect model was adopted because of the high heterogeneity (I 2 = 66%; Fig. 2 and Table 2).
Length of hospital stays
We included a total of 1313 patients in 12 studies21–27,29–31,34,35 analyzing length of hospital stays: 1098 in the primary MIP group and 215 in the secondary MIP group. Subgroup analysis showed either LP (Z = 1.41, P = .16, MD = −0.50 days, 95% CI: −1.19–0.19) or robot-assisted pyeloplasty (Z = 0.04, P = .97, MD = −0.01 days, 95% CI: −0.32–0.31), and there were no significant differences between the primary and secondary surgery. Overall, there were no significant differences in length of hospital stays between two groups (Z = 0.88, P = .38, MD = −0.12 days, 95% CI: −0.38–0.14). The random effect model was adopted because of the high heterogeneity (I 2 = 75%; Fig. 2 and Table 2).
Urinary leakage
We included a total of 521 patients in 5 studies22,27,28,32,33 analyzing urinary leakage, 406 in the primary MIP group and 115 in the secondary MIP group. Primary MIP have a lower risk of urinary leakage than secondary surgery (Z = 1.70, P = .04, RR = 0.32, 95% CI: 0.11–0.93). The fixed effect model was adopted because of no heterogeneity (I 2 = 0%; Fig. 3 and Table 2).

Various complication rates of primary versus secondary minimally invasive pyeloplasty.
Hematuria
We included a total of 200 patients in 2 studies22,27 analyzing hematuria: 136 in the primary MIP group and 64 in the secondary MIP group. There were no significant differences in the risk of hematuria between the primary and secondary MIP (Z = 0.37, P = .71, RR = 0.72, 95% CI: 0.12–4.15). The fixed effect model was adopted because of no heterogeneity (I 2 = 0%; Fig. 3 and Table 2).
Urinary tract infection
We included a total of 433 patients in 4 studies22,25,27,32 analyzing urinary tract infection: 338 in the primary MIP group and 95 in the secondary MIP group. There were no significant differences in the risk of urinary tract infection between the primary and secondary MIP (Z = 0.67, P = .50, RR = 0.64, 95% CI: 0.17–2.37). The fixed effect model was adopted because of no heterogeneity (I 2 = 0%; Fig. 3 and Table 2).
Intestinal obstruction
We included a total of 337 patients in 3 studies25,27,32 analyzing intestinal obstruction: 274 in the primary MIP group and 63 in the secondary MIP group. There were no significant differences in the risk of intestinal obstruction between the primary and secondary MIP (Z = 0.52, P = .60, RR = 0.66, 95% CI: 0.14–3.11). The fixed effect model was adopted because of no heterogeneity (I 2 = 0%; Fig. 3 and Table 2).
Injury of blood vessel
We included a total of 265 patients in 3 studies22,25,27 analyzing injury of the blood vessel: 191 in the primary MIP group and 74 in the secondary MIP group. Primary MIP has a lower risk of injury of blood vessel than secondary surgery (Z = 2.51, P = .01, RR = 0.10, 95% CI: 0.02–0.61). The fixed effect model was adopted due to no heterogeneity (I 2 = 0%; Fig. 3 and Table 2).
Stent complications
We included a total of 362 patients in 3 studies23,28,32 analyzing stent complications: 303 in the primary MIP group and 59 in the secondary MIP group. There were no significant differences in the risk of stent complications between the primary and secondary MIP (Z = 0.58, P = .56, RR = 1.62, 95% CI: 0.32–8.33). The fixed effect model was adopted because of no heterogeneity (I 2 = 0%; Fig. 3 and Table 2).
Overall complications rate
We included a total of 1547 patients in 14 studies21–30,32–35 analyzing overall complications rate: 1296 in the primary MIP group and 251 in the secondary MIP group. Subgroup analysis showed either LP (Z = 1.62, P = .11, RR = 0.55, 95% CI: 0.27–1.13) or robot-assisted pyeloplasty (Z = 0.49, P = .62, RR = 0.90, 95% CI: 0.58–1.39), and the risk of overall complications is no higher with the secondary procedure than with the primary procedure. Secondary MIP does not have a higher risk of overall complications than primary surgery (Z = 1.25, P = .21, RR = 0.79, 95% CI: 0.54–1.15). The fixed effect model was adopted because of the low heterogeneity (I 2 = 35%; Fig. 4 and Table 2).
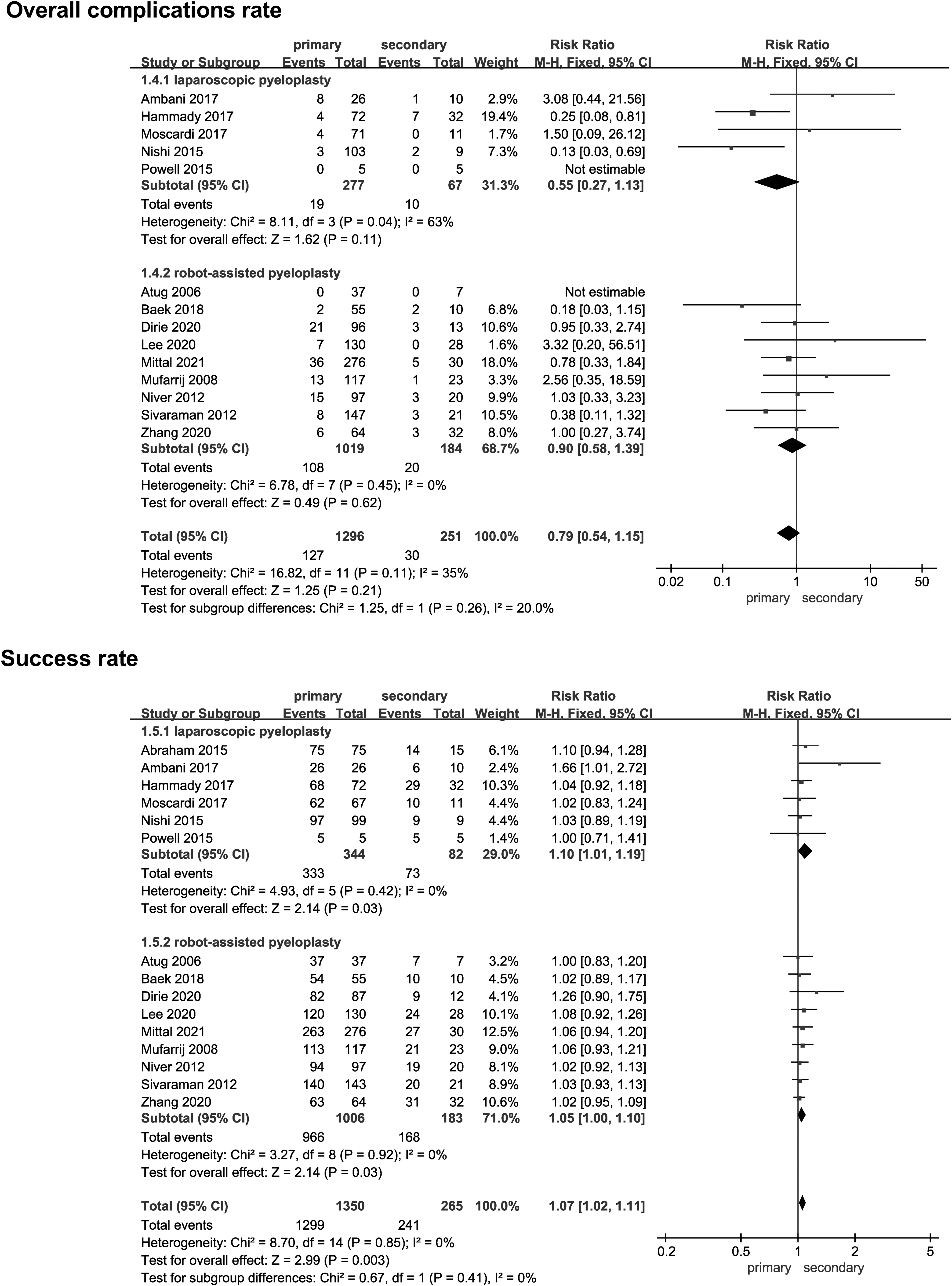
Overall complications and success rate of primary versus secondary minimally invasive pyeloplasty.
Success rate
We included a total of 1615 patients in 15 studies21–35 analyzing success rate: 1350 in the primary MIP group and 265 in the secondary MIP group. Subgroup analysis showed either LP (Z = 2.14, P = .03, RR = 1.10, 95% CI: 1.01–1.19) or robot-assisted pyeloplasty (Z = 2.14, P = .03, RR = 1.05, 95% CI: 1.00–1.10), and the success rate of primary pyeloplasty was higher than that of secondary pyeloplasty. Overall, the success rate of the primary MIP was higher than that of the secondary MIP (Z = 2.99, P = .003, RR = 1.07, 95% CI: 1.02–1.11). The fixed effect model was adopted because of no heterogeneity (I 2 = 0%; Fig. 4 and Table 2).
Publication bias
We use the funnel plots of operative time, estimated blood loss, length of hospital stays, overall complications rate, and success rate in this study to evaluate the publication bias, which has no obvious asymmetry and can be considered as having a small bias (Fig. 5).
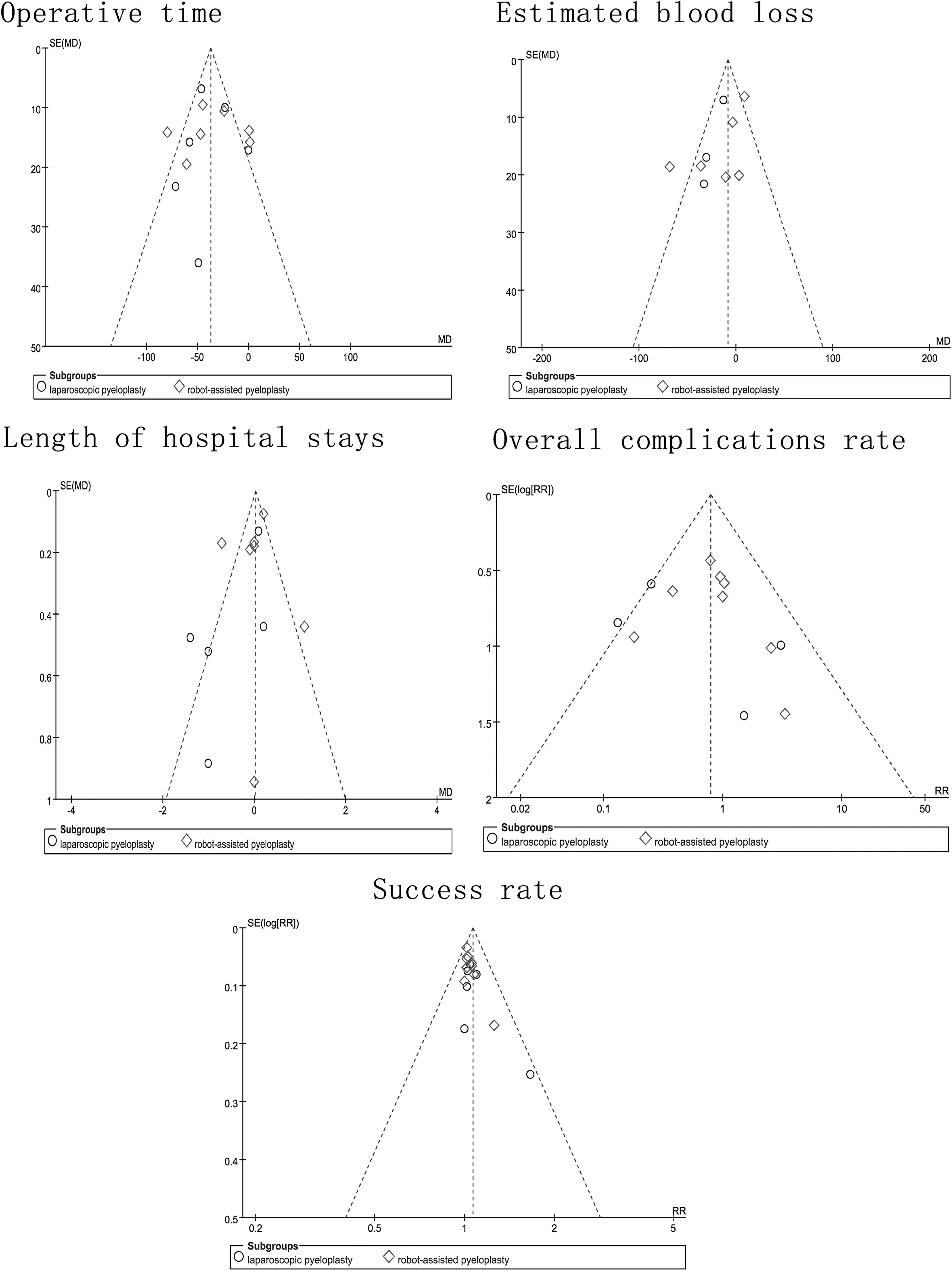
The funnel plots of the study.
Discussion
Recurrent obstruction after primary surgery is a tough problem in the treatment of
Therefore, patients younger than 4 years and ureteral segment stricture greater than 10 mm had a poor prognosis after retrograde endopyelotomy. Abdrabuh et al. 36 compared 27 patients who had undergone endopyelotomy with 16 patients who had undergone pyeloplasty with recurrent UPJO. Although there was no statistically significant difference in surgical success rates: 22 (81.5%) versus 15 (93.8%) in the two groups, all patients who had undergone failed endopyelotomy had stenosis lengths greater than 15 mm, and the average length of ureteral stenosis was longer in the failed group than in the successful group (17.8 ± 1.7 mm versus 10 mm ±3.08, P = .001). Therefore, they concluded that ureteral segment stenosis greater than 15 mm was significantly associated with poor prognosis after endopyelotomy.
Ceyhan et al. 37 reported that redo pyeloplasty was the most effective intervention, with an effective rate of 83.3%, whereas double-J stents implantation, endopyelotomy, and balloon dilation had a success rate of 45.5%, 50%, and 30.8%, respectively. In general, the minimally invasive operation of endourology is less effective than pyeloplasty as well as suitable for the limited population such as patients with short stricture ureteral segment and elder people, and MIP has become an ideal surgical method for the treatment of recurrent UPJO compared with open surgery due to the needs for aesthetic and minimally invasive concepts.
Gettman et al.
38
reported the first case of robotic pyeloplasty in 2002, and since then, it has been widely used worldwide. Robotic surgery offers enhanced three-dimensional vision, reduced tremor, and higher mobility and flexibility, with the added advantage of better maneuverability compared with laparoscopic surgery, improved vision, ease of suturing, and improved ergonomics. Several publications have demonstrated the safety and feasibility of robot-assisted pyeloplasty for the treatment of recurrent
The average operative time (2.10 ± 0.65 hours versus 3.23 ± 0.50 hours, P < .001), suturing time (21.47 ± 2.59 minutes versus 62.43 ± 4.62 minutes, P < .001), and length of hospital stays (7.80 ± 3.10 days versus 9.79 ± 1.76 days, P < .05) of patients in RALP group was significantly shorter than those in LP group. There was no significant difference in the success rate between the two groups (87.7% and 85.7%, respectively). Cheng et al. 41 retrospectively reviewed the results of a secondary procedure in 21 patients who had recurrent UPJO with a long proximal ureteral stricture, including 8 modified robotic flap pyeloplasty (mRFP) and 13 modified laparoscopic flap pyeloplasty (mLFP).
The hospital stays (5.0 ± 1.9 days versus 8.2 ± 3.1 days, P = .015) of mRFP were shorter than those of mLFP. There was no statistically significant difference in the total operation time (142.4 ± 43.6 minutes versus 179.1 ± 54.0 minutes, P = .122), anastomosis time (43.1 ± 19.3 minutes versus 61.0 ± 20.8 minutes, P = .093), estimated blood loss (66.3 ± 45.7 mL versus 58.5 ± 49.5 mL, P = .723), pararenal draining time (3.9 ± 1.1 days versus 5.2 ± 2.6 days, P = .175), and success rate (8/8 [100%] versus 11/13 [84.6%], P = .505) between the two groups. However, there are only two retrospective studies on the comparison of these two surgical procedures with small sample sizes, which need to be confirmed by more large sample sizes and prospective studies involving high quality.
Among the 15 studies21–35 included in our meta-analysis, the same conclusions as ours were 9 studies21–23,25,27,28,30,31,35 on the operative time, 6 studies22,24,30,33–35 on the estimated blood loss, and 9 studies23–25,27,29–31,34,35 on the length of hospital stays. Our study showed that the operative time in the primary MIP group was shorter than that in the secondary MIP group, estimated blood loss in the primary MIP group was less than that in the secondary MIP group, whereas there were no significant differences in length of hospital stays between the two groups. Subgroup analysis of our meta-analysis showed that robot-assisted pyeloplasty is superior to LP in controlling the amount of blood loss in the second operation; no significant difference has been found between robot-assisted pyeloplasty and LP in other aspects.
Recurrent
Of the 14 studies21–30,32–35 analyzing complications rate, 12 studies21–26,28,29,32–35 came to similar conclusions. There were no significant differences in the risk of hematuria, urinary tract infection, intestinal obstruction, stent complications, and overall complications between the primary and secondary MIP, while primary MIP has a lower risk of urinary leakage and injury of blood vessel than secondary surgery. Postoperative urinary leakage is a serious complication, as it may aggravate periureteral inflammation, stimulate a caustic reaction, and lead to restenosis.27,42
Seo et al. 43 also found that drainage is a risk factor for surgical failure (P = .024). Due to the shortening of the ureter after the initial operation and the fact that some patients with long-segment stenosis are prone to recurrence, the anastomotic tension in the secondary procedures is larger than that of primary procedures, and even tension-free anastomosis cannot be achieved in some patients, which resulted in a higher risk of urine leakage in secondary surgery. In the secondary operation, vascular injury is more likely to be caused by unclear local anatomical levels and heavy adhesion.
The success rate of the primary MIP was higher than that of the secondary MIP, whether laparoscopic, robotic, or overall. All the 15 studies21–35 included in our meta-analysis were inconsistent with our conclusion, which we believed was caused by the small sample size of secondary surgery. The tailor of pyeloplasty is the prerequisite, and the suture technique is the necessary guarantee of the success of the operation. The key point of the operation is to reconstruct the funnel-shaped ureteropelvic junction, ensure no distortion of the ureter, and achieve water-tight tension-free anastomosis. 44
The lower success rate of the secondary operation may be related to the following reasons. First, the exacerbation of local fibrosis after the initial operation led to incomplete anatomical separation during the operation, and the planned tailor of the pelvic and ureter flap was not as perfect as the primary procedure. An excessive tailor would be bound to excessive tension of the anastomosis, and the insufficient tailor would result in the difficulty of downward transmission of peristalsis wave. Second, the omission of crossing vessels in the initial surgery increased the difficulty of identifying and treating them in the secondary operation.
Crossing vessels resulted in exogenous obstruction. 45 Studies have confirmed that the improper treatment of crossing vessels is one of the important causes of reobstruction.15,46 In addition, the lower success rate is associated with a higher incidence of postoperative urinary leakage in patients who underwent secondary surgery. Considering that the initial intervention failure will affect the long-term efficacy of secondary surgery, we believe that the need for further postoperative intervention should be avoided as much as possible during the initial operation. During the operation, the UPJO should be dissected carefully, the periureteral sheath containing blood supply to the ureter should be retained, and water-tight tension-free anastomosis should be achieved.
Lucas et al. 47 conducted a study, which showed that the probability of not undergoing repeat surgery at 1 and 2 years after surgery in patients who underwent preoperatively endopyelotomy and those who did not undergo endopyelotomy was 90% ± 4.5% and 81% ± 7.3% versus 97% ± 1.0% and 93% ± 1.8%, respectively (P < 0.001), and the counterpart probability in patients with and without intraoperative crossing vessels was 95% ± 1.7% and 88% ± 3.4% versus 97% ± 1.7% and 95% ± 2.1%, respectively (P = .028). In a multivariate analysis, previous endopyelotomy (hazard ratio [HR] 4.35) and intraoperative crossing vessels (HR 2.73) markedly affected the success rate of surgical intervention.
Therefore, special attention should be paid to not miss the crossing vessels. In addition, we suggest that it would be more prudent to perform a more definitive procedure with pyeloplasty instead of endopyelotomy for primary
Limitations
There are a few limitations of our study. First, all relevant studies that met the inclusion and exclusion criteria were included in this systematic review, but the quality of the included literature was relatively low, only 1 of the 15 studies was a retrospective combined prospective study, and the sample size included in the study was small, especially in the second surgery group, which had a significant impact on the results of the systematic review.
Second, the heterogeneity of the main indicators (operative time, estimated blood loss, and length of hospital stays) was noteworthy high. Heterogeneity may be due to differences in surgical methods or other aspects. We used the random effects model to reduce the bias caused by high heterogeneity.
Third, so far, there are few articles about the comparison of various types of complications (urinary leakage, hematuria, urinary tract infection, intestinal obstruction, injury of blood vessel, and stent complications), so the number of literature that can be included in this study is small, which may have a great influence on the conclusion.
In addition, the clinical application of robotic surgery is later than laparoscopic surgery, and its technology is not fully mature in some hospitals and regions, so we can only compare the differences between robotic and LP to a certain extent indirectly in the subgroup analysis. Although we found differences in blood loss control between the two procedures, it cannot be ruled out the possibility that these differences may be due to the experience of the surgeon. A sufficient amount of literature on the direct comparison of robotic versus laparoscopic secondary surgery is scarce and demonstrates divergent consequences. Therefore, in future studies, a larger sample size, longer follow-up time, and high-quality prospective studies are required to precisely verify our results.
Conclusions
The secondary MIP is associated with longer operative time, more estimated blood loss, higher rates of urinary leakage and injury of a blood vessel, and lower surgical success rate than the primary MIP. Considering that the initial intervention failure will affect the long-term efficacy of secondary surgery, we believe that the need for further postoperative intervention should be avoided as much as possible during the initial operation. Special attention should be paid to not miss the crossing vessels. In addition, we suggest that it would be more prudent to carry out a more definitive procedure with pyeloplasty instead of endopyelotomy for primary
Footnotes
Authors' Contributions
T.D. and P.S. contributed to the idea and formed the study design. T.D. and P.Q. undertook to screen articles, data extraction, and quality assessment. L.H. analyzed the data. T.D., S.Y., and B.Z. contributed to the drafting. T.D. and P.S. critically reviewed the article. All authors contributed to drafting the article and approved the final version. All the authors agree to be responsible for all aspects of the study, and they all have read and approved the final article.
Acknowledgments
Thanks to all authors for contributing to this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.