
Abstract
Background:
This study aims to review laparoscopic repair techniques of Morgagni hernias at a tertiary referral center.
Methods:
This retrospective study includes pediatric patients who underwent laparoscopic repair of Morgagni hernia between March 2004 and March 2021. The patients' demographics, presenting symptoms, operative approach, and postoperative outcomes were recorded.
Results:
Fourteen patients underwent laparoscopic repair of Morgagni hernia. The mean age at the time of operation was 24.7 months. Defect closing techniques were intracorporeal knot tying (n: 2), extracorporeal knot tying, and subcutaneous knot placement (n: 10), combination with intracorporeal continuous suturing and several extracorporeal intermittent sutures (n: 2). Different approaches were used during removal of the needle from the insertion point in the extracorporeal knot tying: intracorporeally, using a laparoscopic needle holder (n: 6), with an 18-gauge injector tip (n: 1), and extracorporeally with suture passer forceps (n: 3). In the intracorporeal knot tying technique, the mean operation time was 127 minutes (range 90–180 minutes). In the extracorporeal knot tying technique, the mean operation time was 75 minutes (range 30–180 minutes). The mean operation time in the technique that used suture passer forceps for removing the needle from the same point of insertion was 40 minutes. There was no intraoperative complication.
Conclusions:
In the laparoscopic repair of Morgagni hernia, full-thickness anterior abdominal wall repair with interrupted sutures that are tied extracorporeally in the subcutaneous tissue by separated minor skin incisions is the easy approach. Using suture passer forceps during removal of the needle facilitates this technique and shortens the operation time.
Introduction
Morgagni hernia is an extremely rare disease defined as the congenital herniation of abdominal contents into the thoracic cavity through a retrosternal diaphragmatic defect. It has a prevalence of 1:5000 in live births and comprises 3%–5% of all surgically treated congenital diaphragmatic hernias. 1 Surgical options include open repair (transabdominal or transthoracic route) or laparoscopic repair. In 1997, Georgacopulo et al. described the first successful laparoscopic repair of Morgagni hernia in a 4-year-old child. 2 Various laparoscopic techniques to repair Morgagni hernia, including primary closure with continuous or interrupted intracorporeal suture and full-thickness anterior abdominal wall repair by subcutaneous knot placement and closure with mesh, have been described since then.3–5
Intracorporeal suturing for closure of the defect is technically challenging because it is difficult to pass the needle through the anterior abdominal wall and because the anterior diaphragmatic wall is very thin for repair. Likewise, in extracorporeal suturing, although the transabdominal insertion of the needle is easy, removal of the needle from the same point of insertion during the full-thickness anterior abdominal wall repair can be difficult. 6 Due to the rarity of Morgagni hernia and lack of data on laparoscopic surgical treatment, there is no standard technique for its treatment. The purpose of this study was to review the laparoscopic repair techniques of Morgagni hernias at our institution and look for possible improvements in laparoscopic repair.
Methods
This retrospective study includes pediatric patients who underwent laparoscopic repair of Morgagni hernia between March 2004 and March 2021. Institutional ethics committee approval was provided for the study (Approval No.: 2021-8/7). The patients' demographics, presenting symptoms, operative approach, and postoperative outcomes were recorded. During the postoperative period, all patients were followed up with chest X-rays on postoperative 1st and 12th month outpatient visits.
Operative techniques
Under general anesthesia, the patient was placed in supine and reverse Trendelenburg position. The surgeon was positioned between the patient's legs. The three-port technique was preferred. A 5- or 10-mm camera port was introduced through the umbilicus incision through the open method, and a 30° telescope was used. Two 5-mm working ports were introduced from the right and left upper quadrants, lateral to the rectus muscles under direct vision. The hernia sac was excised, or if the hernia sac was not to be excised, the edges of the defect were cauterized before suturing. The falciform ligament was resected if better visualization would be provided.
Suturing the defect technique included using extracorporeal or intracorporeal knot tying or a combination with nonabsorbable sutures. Nonabsorbable suture such as 2/0 polyester, polypropylene, or silk was used.
Defect closing techniques
Intracorporeal knot tying: defect closure was performed intracorporeally with continuous or interrupted suturing (Fig. 1a and b).
Extracorporeal knot tying and subcutaneous knot placement: a full-thickness anterior abdominal wall repair was performed with interrupted sutures that were tied in the subcutaneous tissue by separated minor skin incisions. Sutures were passed into the abdomen through small 2-mm skin incisions in the anterior aspect of the abdominal wall, and then the needle was passed through the posterior rim of the defect with a laparoscopic needle holder and was retrieved back out through the same small skin incision (Fig. 2). During removal of the needle from the same entry site, the needle was passed from the inside to outside by using a laparoscopic needle holder, or an 18-gauge injector tip and suture passer forceps were passed from the outside to inside through the abdominal wall, through the same skin opening, grasped, and pulled to the outside (Fig. 3a–c). The sutures' knots were embedded in subcutaneous tissue. The defect was closed with U-shaped interrupted sutures (Supplementary Video S1).
Combination of intracorporeal knot tying and extracorporeal knot tying: intracorporeal continuous suturing was used to repair the defect and several extracorporeal intermittent sutures were applied for strengthening (Fig. 4).
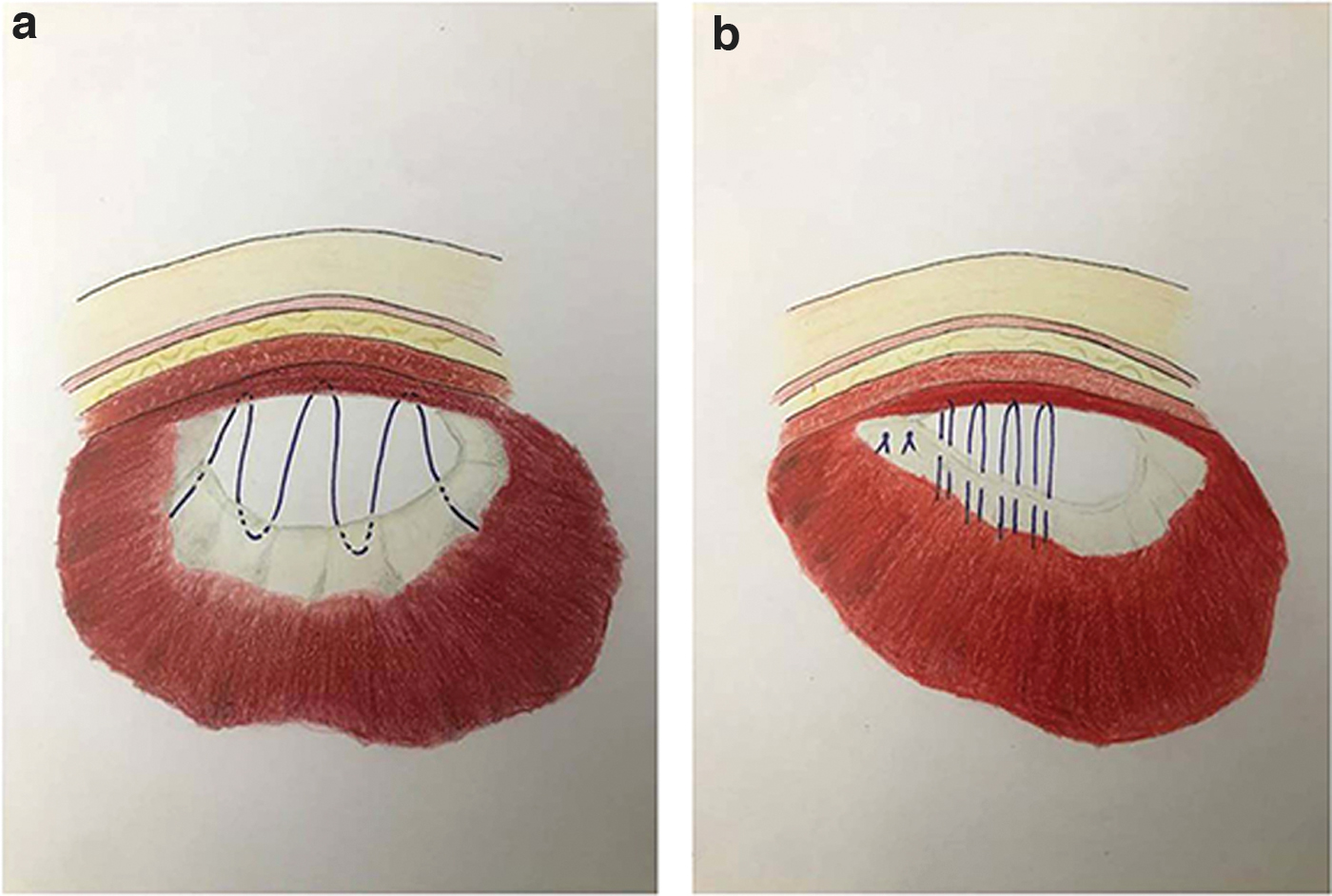
Intracorporeal knot tying with continuous suturing

Extracorporeal knot tying and subcutaneous knot placement. Color images are available online.
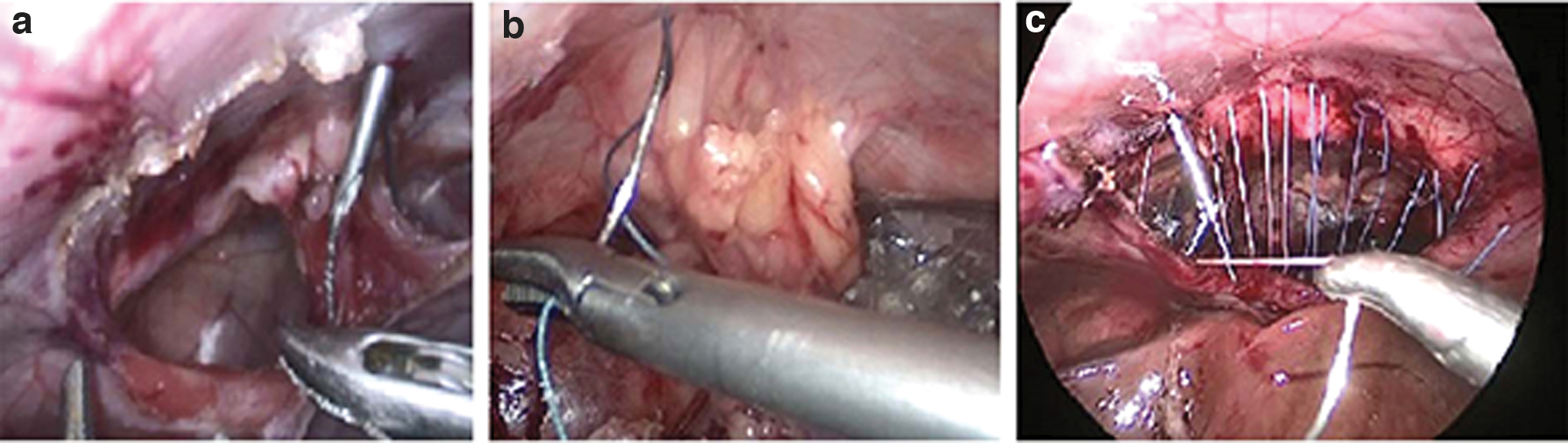
Techniques of removal of needle: 18-gauge injector tip was inserted through the skin incision and removed by passing the tip of the needle to the injector tip
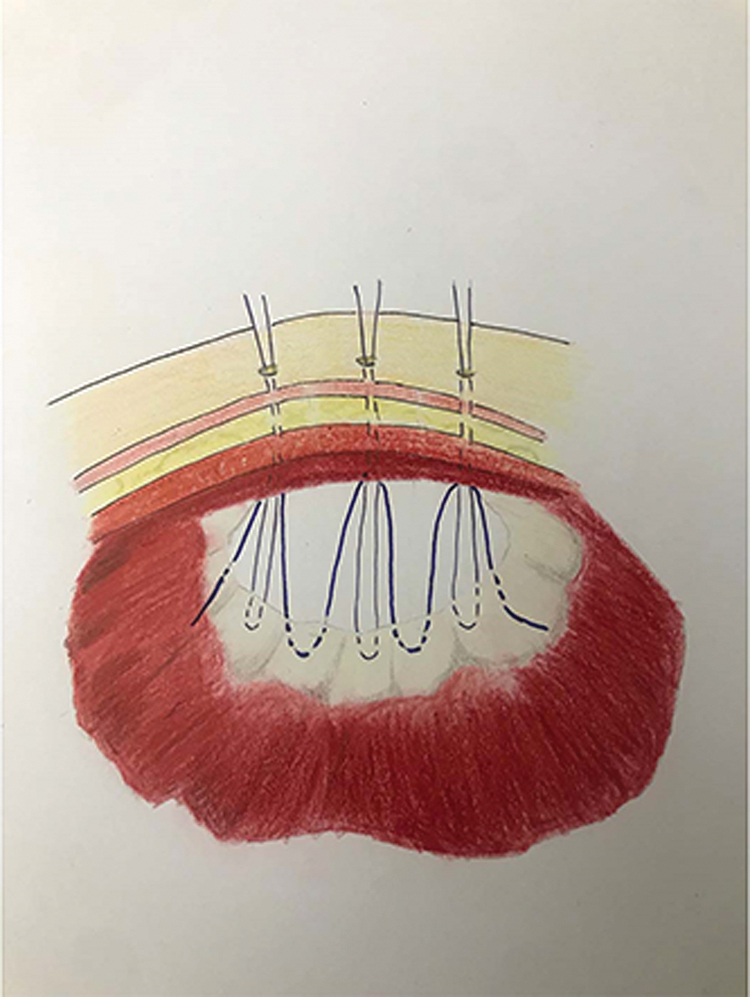
Combination of intracorporeal knot tying and extracorporeal knot tying. Color images are available online.
Results
Fourteen patients (seven males and seven females) underwent laparoscopic repair of Morgagni hernia. The mean age at the time of operation was 24.7 months (range: 3 months to 6 years).
Five patients (36%) were symptomatic and 9 (64%) were asymptomatic at presentation. Asymptomatic patients were diagnosed incidentally by chest X-ray that was performed during evaluation for upper respiratory tract infections (n: 4) or other conditions (n: 5). Symptomatic patients presented with pneumonia (n: 4), vomiting (n: 1), thoracic intestinal sounds (n: 1), and respiratory distress (n: 1). Comorbidities included trisomy 21 (n: 5), congenital heart disease (n: 5), pectus carinatum (n: 1), gastroesophageal reflux (n: 1), Alagille syndrome and cystinosis (n: 1), brachiocephalic, and ectopic right kidney with pelvic localization and right hemihypertrophy (n: 1). In all patients, Morgagni hernia was diagnosed by chest X-ray, but additional CT was performed in 5 patients (Table 1).
Patients Characteristics
Diagnosed incidentally by chest X-ray, which were needing during evaluation of upper respiratory tract infections.
CT, computed tomography; CXR, chest X-ray; F, female; L-RTI, lower respiratory tract infection; M, male.
There were 4 patients whose defect was closed with intracorporeal knot tying. Continuous suturing was used in 3 of those, while interrupted suturing was used in 1. Several extracorporeal intermittent sutures were applied for strengthening in 2 out of 3 patients with continuous suturing. Ten patients underwent extracorporeal knot tying and subcutaneous knot placement for a full-thickness anterior abdominal wall repair.
Different approaches were used during removal of the needle from the insertion point in the extracorporeal knot tying: intracorporeally, using a laparoscopic needle holder (n: 6), with an 18-gauge injector tip (n: 1), and extracorporeally with suture passer forceps (n: 3). The mean of defect diameters was 4 × 5 cm. There was no need for a prosthetic patch. In the intracorporeal knot tying technique, the mean operation time was 127 minutes (range 90–180 minutes). In the extracorporeal knot tying technique, the mean operation time was 75 minutes (range 30–180 minutes). The mean operation time in the technique that used suture passer forceps for removing the needle from the same point of insertion was 40 minutes. Operative repair, findings, and outcomes are shown in Table 2.
Operation Technical Details
Intracorporeal continuous suturing was used to repair the defect and several extracorporeal intermittent sutures were applied for strengthening.
The needle was taken out from intra-abdomen with a laparoscopic needle holder by intracorporeally.
By using 18-gauge injector tip and Suture Passer Forceps, mini-incision sites in the epigastric region were entered into the abdomen transabdominal and extracorporeally, and the needle was removed from the same place.
There were no intraoperative complications. Fever (n: 2), postoperative need for oxygen therapy (n: 1), atelectasis (n: 1), and urinary tract infection (n: 1) were seen postoperatively. Postural drainage was not adequate in the case with atelectasis and bronchoscopy was required in 1 patient. One patient died on the postoperative eighth day due to cardiac failure, pneumonia, and sepsis. In 1 patient whose sac was excised incompletely, fluid collection into the residual sac was observed postoperatively for 2 months. The other patients had uneventful postoperative follow-ups. There was no evidence of recurrence during the follow-up period. The follow-up range was 1 month to 4 years.
Discussion
The studies in the literature have described various techniques for repairing Morgagni hernias, including open repair, laparoscopic, thoracoscopic, and robotic techniques. 5 The laparoscopic approach is preferred due to shorter operation time, less analgesia, early oral feeding time, shorter hospital stay, and better cosmesis compared to open surgery. 7 In addition, the laparoscopic technique is superior to thoracoscopy due to easy reduction of the hernia, better visualization for bilateral hernia, and bilateral repair. 5
In Morgagni hernia, a standard laparoscopic technique has not been accepted because of differences in the removal of the sac and repair of the defect with extracorporeal or intracorporeal suture techniques. It is believed that full-thickness abdominal wall repair with the extracorporeally tied interrupted sutures is sturdier and easier to perform.
Hernia sac excision is controversial in Morgagni hernia repair. Most surgeons avoid it because of the risk of injury to the pleura, pericardium, and phrenic nerve. 5 However, leaving the sac as it is can lead to recurrence or fluid collection in the residual cavity. In the majority of our cases, we preferred to remove the sac. We did not see any complication in cases where the entire sac was removed. In 1 case, the sac was not removed completely due to adhesions of the sac to the pleura. In this case, postoperative fluid collection into the residual sac was observed. In the literature, in cases where sac removal is not preferred, cauterization of the edges of the defect is recommended to induce scar tissue and to reduce the incidence of recurrence, as well as closing the defect with the stitches that include the sac to avoid the formation of a residual cavity in the thorax.5,8
A variety of repair techniques, including primary closure with a continuous suture, interrupted suture, or using a mesh, have been described.3,4,9
The laparoscopic interrupted or continuous suture techniques in particular, if done intracorporeally, are not simple and are time-consuming. In addition, because the diaphragm muscle at the anterior edge of the diaphragmatic defect is not well developed or not developed at all, crossing the anterior edge of the defect intracorporeally poses a risk for recurrence. Moreover, it is difficult to pass the suture from there. In some cases with continuous sutures, we applied a few supporting sutures with extracorporeal full-thickness and extracorporeal knotting. This was done to prevent tension and separation in the continuous suture line. Similarly, Esposito et al. used a transparietal stitch to suspend the diaphragm intraoperatively and to reduce the tension on the two muscular edges during the closure of the defect. 8
The preferred technique for most surgeons is extracorporeal tied interrupted sutures.5,8 We used percutaneous sutures through the abdominal wall to the abdominal cavity. Sutures were passed into the abdomen through small 2-mm skin incisions, which ensured less scarring. The needle passed the posterior rim of the defect and was returned back out of the anterior abdominal wall through the same incision site, but not the same entry point of the anterior abdominal wall. The needle was returned back out of the anterior abdominal wall at a distance of about 0.5 cm and a U-suture was formed. Each suture was approximated to the abdominal wall without an angle due to small 2-mm skin incisions and separate entry and exit points of the needle on the anterior abdominal wall.
When the sutures are inserted through a 1-cm incision made in the epigastric region to avoid a larger incision, the suture line can shrink and become angled.4,6,10 Since we did not pass sutures from a single point, the suture line can remain straight without any angulation because the sutures correspond to the abdominal wall. We believe that the suture line will be sturdier when done with intermittent U sutures by passing the needle through the abdomen, with small incisions in the skin to close the defect.
In the extracorporeal knot tying and subcutaneous knot placement technique, sutures are passed into the abdomen extracorporeally, then the needle is passed through the posterior of the defect's rim and is retrieved back out of the abdomen. Removing the needle from the point of entry could be difficult for the surgeon. Thus, researchers have come up with modifications for this technique such as a transabdominal wall closure with loop suture held by an 18- or 20-gauge catheter needle,6,11 an 18-gauge epidural needle, 12 or a Reverdin needle. 13 These devices can be directly maneuvered under visualization. However, using a straight and long needle can pose difficulty in manipulating, while passing the needle through the defect edge.
We retrieved the needle by using a laparoscopic needle holder, or an 18-gauge injector tip and suture passer forceps. The needle is easily removed from the abdomen by inserting the suture passer forceps through the same skin incision into which the needle was inserted. Using suture passer forceps was the easiest technique to remove the needle from the abdomen and this technique also reduced the operation time. The length of the procedure with three trocars and full-thickness abdominal wall repair in expert hands was reported to be about 60 minutes. 8 In our study, this meantime was 75 minutes. However, using suture passer forceps for removing the needle reduced operation time to 40 minutes. In addition, extracorporeal suture tying is easier than intracorporeal tying.
Surgeons prefer using mostly nonabsorbable materials for faster extracorporeally tied knots and to avoid the risk of recurrence.5,8 We used nonabsorbable sutures such as 2/0 and polyester, polypropylene, and silk. We preferred polyester sutures in extracorporeal knot tying and subcutaneous knot placement technique, in particular, because subcutaneous knot placement with polypropylene sutures gave patients a feeling of discomfort.
In this study, there are some limitations due to unequal distribution in the number of cases. The reason for this is that, while we used intracorporeal techniques in the repair of Morgagni hernia in the first years, we later preferred extracorporeal repair due to the difficulty of the intracorporeal technique.
We tried different methods for closure of defect in the laparoscopic repair of Morgagni hernia. We suggest full-thickness anterior abdominal wall repair with interrupted sutures that are tied extracorporeally in the subcutaneous tissue by separated minor skin incisions is a simpler approach. Using suture passer forceps during removal of the needle from the same point of entry in the extracorporeal knot tying is easy for the surgeon. Moreover, this technique has a shorter operation time compared to other approaches.
Compliance with Ethical Standards
Ethical approval
All procedures performed on human participants were by the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from parents of all patients before all procedures. Numerous minimally invasive methods have been introduced to try to overcome both the short- and long-term disadvantages and morbidity of open techniques.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.