
Abstract
Aim:
Laparoscopic inguinal hernia (IH) repair is an alternative to open surgery. A potential advantage of laparoscopic repair is prevention of contralateral metachronous hernia although some studies report higher recurrence rate. We aim to determine the cost-effectiveness of open versus laparoscopic IH repair taking into account metachronous and recurrence rates.
Methods:
Retrospective single-center study of children (<5 years) undergoing elective open or laparoscopic repair for a unilateral IH between February 2018 and October 2019. Ten cases in each of four groups were included (open day case, open overnight, laparoscopic day case, and laparoscopic overnight). Cases incurring a higher cost due to comorbidities or additional procedure were excluded. Patient-level information and costing system data were obtained from the hospital finance. Mean (standard deviation [SD]) procedural cost was compared for open and laparoscopic procedures. A financial model was created factoring metachronous and recurrent rates.
Results:
Cost of open day case repair was £1866.24 (SD: 311.15) compared with £2210.13 (SD: 391.36) for day case laparoscopic repair. For overnight repair, cost of open was £2442.82 (SD: 497.05) compared with £2585.35 (SD: 384.66) for laparoscopic. On calculating the cost-effectiveness point using the difference in metachronous and recurrence rate between the two procedures, laparoscopic is more cost-effective than open day case repair at 18.43%. For overnight repair, the difference rate is 5.84%.
Conclusion:
Our data suggest that based on metachronous and recurrence rates in the current literature, laparoscopic IH repair is more cost-effective than open repair for cases requiring overnight stay, whereas for day case procedures open IH repair is more cost-effective.
Introduction
Inguinal hernia (IH) repair is one of the most common pediatric surgery operations. For the past two decades laparoscopic IH repair has been offered by some surgeons as an alternative to open surgery. 1 A number of studies have compared outcomes between laparoscopic and open surgery, with differing reports on postoperative complications, operative time, and cosmesis. 2
A specific advantage of laparoscopic repair, to which many pediatric surgeons are attracted, is the prevention of contralateral metachronous IH3,4 through simultaneous closure of a contralateral, although asymptomatic deep inguinal ring. To realize the benefit of this, other aspects of the two procedures should be equal and in particular the recurrence rate, since the benefit of preventing contralateral metachronous hernia is primarily in avoidance of a further surgical procedure. It is relevant, therefore, that some studies report a higher recurrence rate with laparoscopic IH repair compared with open surgery 5 although this is not borne out in recent meta-analyses.6–8
One aspect that has not been investigated thoroughly is the cost-effectiveness of laparoscopic and open IH repair, taking into account both metachronous and recurrence rate. There is an assumption that laparoscopic repair is more expensive largely due to longer operating time. However, a cost-effectiveness analysis should also include need for further surgical procedures and, therefore, take into account any differences in metachronous and recurrence rate between the two techniques. Open IH repair may ultimately be less cost-effective since a child may require more than one IH repair dependent on rates of recurrence and metachronous contralateral IH. Given this paucity of information, we aimed to determine the cost-effectiveness of open versus laparoscopic IH repair.
Materials and Methods
We undertook a retrospective single-center study of children <5 years of age, the common age group for pediatric hernia repair, undergoing elective open or laparoscopic repair for a unilateral hernia between February 2018 and October 2019. Patients were included in reverse chronological order to provide accurate and contemporary cost until 10 patients in each group of interest were achieved.
Since IH in some children are undertaken as an overnight stay procedure as opposed to a day case procedure (for instance in small infants <50 weeks of corrected gestational age or due to anesthetic concerns) we predetermined there should be four groups—open day case, open overnight stay, laparoscopic day case, and laparoscopic overnight stay for a total of 40 cases. Patients who had an emergency repair, required critical care input, underwent an additional procedure or incurred higher costs as a result of medical comorbidities were excluded since these outliers may skew overall results.
Patient-level information and costing system (PLICS) data were obtained from the hospital finance system. This novel but detailed approach to recording hospital costs is regarded as the actual cost of admission (and is used to calculate national tariffs in the United Kingdom) and accounts for ward cost, theatre time, anesthesia, medication, and staff costs. PLICS uses activity-based allocation that ensures all interventions and events during a patient episode are accounted for thorough clinical coding. It traces resources used by an individual patient in diagnosis and treatment and calculates the expenditure of those resources using the actual costs incurred by the organization. 9
Mean (standard deviation [SD]) cost for the entire patient journey from admission to hospital discharge was compared for open and laparoscopic procedures. A theoretical construct was created to allow comparison of costs between groups that accounts for both metachronous and recurrent hernia rates combined (Table 1). As current literature suggests recurrence rates between the two surgical approaches are similar and there is a lower metachronous rate with laparoscopic IH repair, the percentage difference favors a laparoscopic approach. For example, if the metachronous rate was 5% in open and 1% in laparoscopic with a rate of recurrence of 1% in open and 2% in laparoscopic, then the difference would be 3% (Table 2(A)).
Theoretical Construct for Calculating Difference in Combined Rate of Metachronous Hernia and Recurrent Hernia Between Open and Laparoscopic Procedures
Illustrative Examples of Combined Difference Rate of Metachronous Hernia and Recurrent Hernia Between Open and Laparoscopic Procedures
Other example scenarios are illustrated in Table 2. The rate provides an indication of how many further operations per one hernia, if performed open rather than laparoscopic, is required in the population across a range of metachronous and recurrent hernia rates. For example, at 3% it indicates 3 more hernia repairs (either recurrent or metachronous) are required for every 100 hernia repairs completed. Therefore, it would cost 1.03 times more for an open IH repair compared with a laparoscopic IH repair (Table 3). For example, if the cost of a laparoscopic IH repair was £1000, at a 3% difference rate, the total cost per infant for an open IH repair would be £1030. We assumed that the cost of recurrent hernia repair and metachronous hernia repair are the same as the index hernia repair.
Financial Construct Used for Comparing Costs Between Open and Laparoscopic Approaches
To explore which components of the care journey may contribute to difference in cost between open and laparoscopic approaches we also obtained data on duration of procedure for each case.
Demographic data were compared using Fisher's exact test and Mann–Whitney U test as appropriate using SPSS.
Results
Forty patients were included in the study with 10 cases in each of the four predefined groups. Demographic data between the groups were similar (Table 4).
Comparison of Demographic and Clinical Data for Cases in This Series—Day Case Procedures (A) and Overnight Stay Procedures (B)
Data presented as median (range) or number of cases (%).
Mann–Whitney U test and Fisher's exact test as appropriate.
The mean cost for an open IH repair day case was £1866.24 (SD: 311.15). The average cost for laparoscopic IH day case was £2210.13 (SD: 391.36). The average cost for open IH repair with overnight stay was £2442.82 (SD: 497.05), whereas the average for laparoscopic IH repair overnight was £2585.35 (SD: 384.66).
On calculating the cost-effective point using the difference of metachronous and recurrence rate between laparoscopic repair and open repair, the difference rate at which laparoscopic is more cost-effective than open IH repair for day case hernia repairs is 18.43% (Fig. 1). For overnight IH repair cases, the difference rate is lower at 5.84% (Fig. 2). Thus, for overnight stay procedures in situations when the difference in combined recurrence/metachronous hernia rate exceeds 5.84%, a laparoscopic approach to initial IH repair is likely to be more cost-effective than the open approach. However, for day case IH repair, a laparoscopic approach only becomes cost-effective when the difference in combined recurrence/metachronous hernia rate exceeds 18.43%, a situation that is unlikely given reported rates of recurrence and metachronous IH.
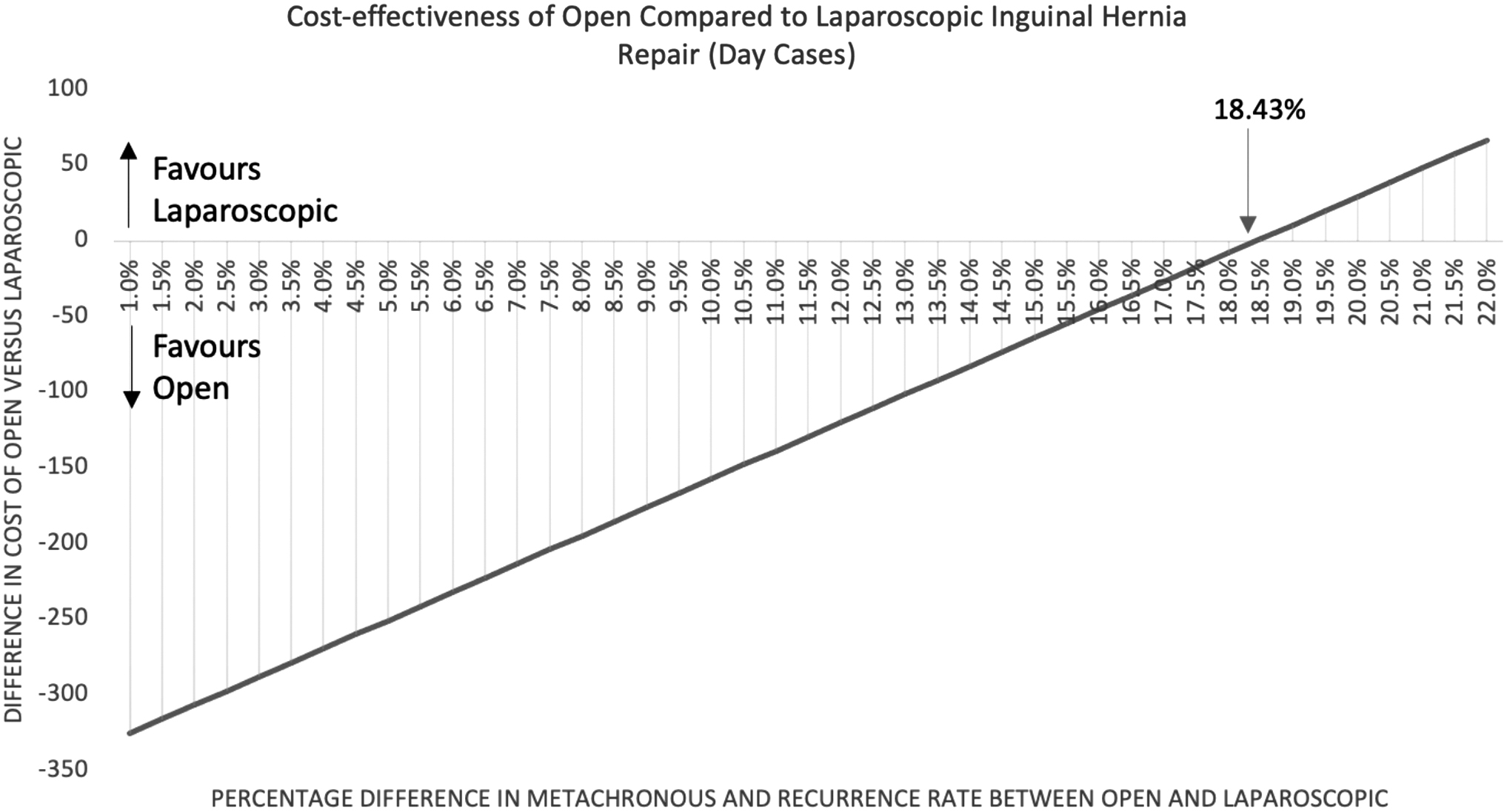
Cost-effectiveness of open compared with laparoscopic IH repair (day cases). IH, inguinal hernia.
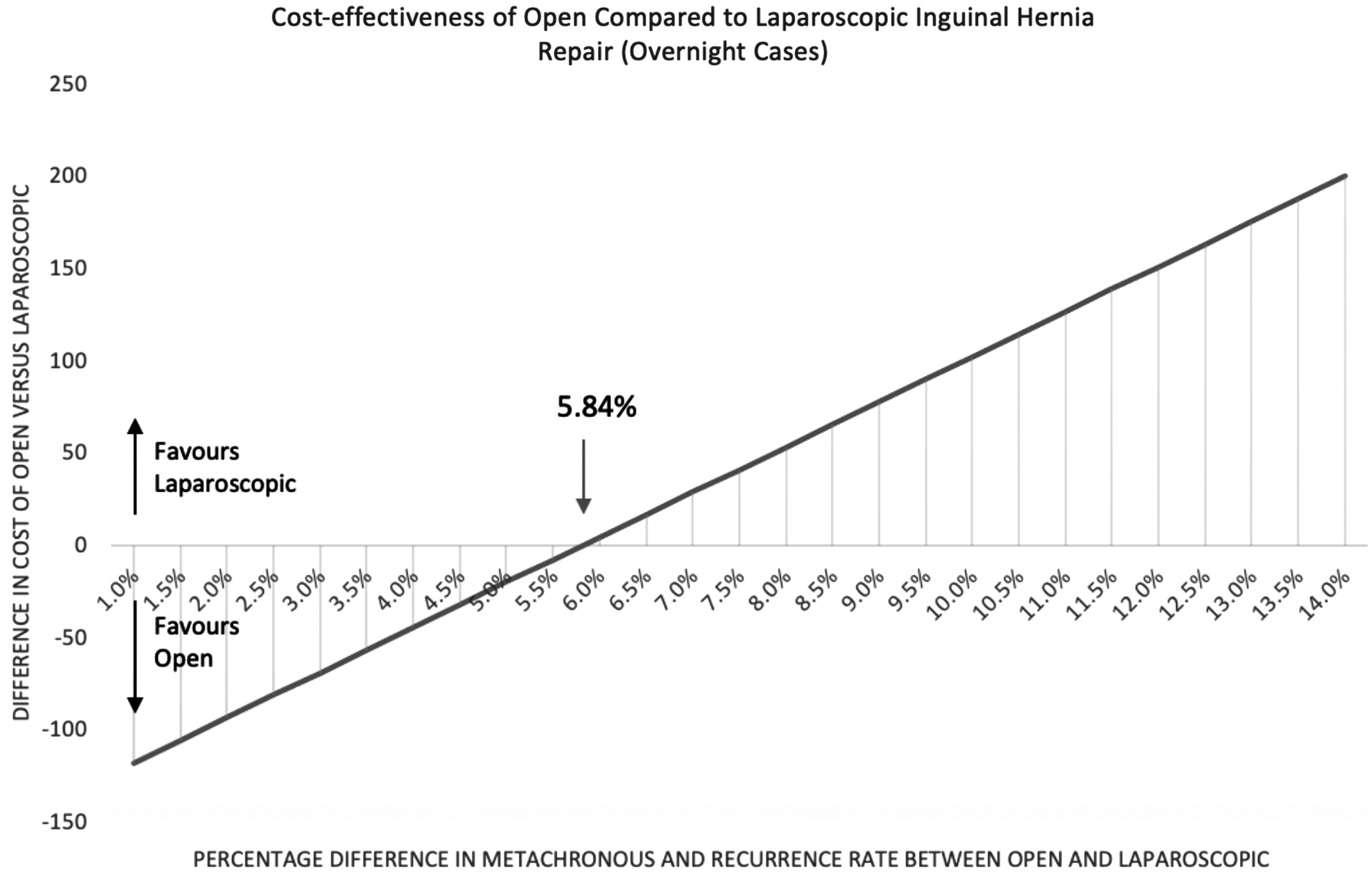
Cost-effectiveness of open compared with laparoscopic IH repair (overnight cases). IH, inguinal hernia.
There was no statistically significant difference between the operating time between the two groups in either day case or overnight groups (Table 5).
Comparison of Operative Time Between Open and Laparoscopic Procedures for Day Cases (A) and Overnight Stay Cases (B)
Data are median (range).
Data unavailable for 1 case.
Discussion/Conclusion
In this study of the comparative cost-effectiveness of open and laparoscopic IH repair in children we have established cutoff points in the combined rate of recurrent and metachronous hernia at which we can anticipate that one approach becomes more cost-effective than the other.
Based on our data, arising from the UK National Health Service health care system, we have established that for IH repair performed as an overnight stay, a laparoscopic approach is more cost-effective than the open approach in situations where the difference in combined recurrent/metachronous hernia rate is >5.84% (i.e., 1 in 17 or more open hernia repairs would be followed by a further procedure). For IH repair performed as a day case procedure, a laparoscopic approach is more cost-effective than the open approach in situations only where the difference in combined recurrent/metachronous hernia rate is >18.43% (i.e., 1 in 5 or more open hernia repairs would be followed by a further procedure).
Using real-world data of reported recurrent and metachronous hernia rates based on recent meta-analysis (metachronous rate of 6–12% and similar recurrence rates between laparoscopic and open IH repair4,6–8,10–13) our data suggest that laparoscopic IH repair is a cost-effective alternative to open repair for procedures requiring an overnight stay, whereas an open approach is more cost-effective for procedures performed as a day case.
To our knowledge there are only two previous studies examining the cost-effectiveness of laparoscopy in IH repair in children. Unlike our study, both studies look at performing laparoscopy at the time of open hernia repair to look for contralateral hernia repair and completing open repair rather than laparoscopic repair alone. Although with a different method, both the American and German study show that the added benefit of laparoscopy to identify contralateral hernia was more cost-effective than returning for an open contralateral metachronous hernia repair at a later stage.14,15
Our study has a more contemporary outlook as both studies were published 10 years ago and in current practice, most surgeons would opt either to do laparoscopic repair or open repair rather than a hybrid as described in these studies. In addition, as not every open hernia repair requires a contralateral metachronous hernia repair, our study considers a more realistic outlook by factoring in potential metachronous and recurrence rate to determine when laparoscopic IH repair is more cost-effective. Our study is the first to examine the cost-effectiveness between the two procedures.
Laparoscopy is generally considered more expensive due to the equipment and operating time. 16 Certainly using a micro-costing technique at our institution, laparoscopic IH repair was associated with greater cost than open IH repair across both day case and overnight stay procedures. We are not able to determine which aspect of the patient journey contributes to this increased cost but of note operative time (knife to skin to skin close) was similar between open and laparoscopic procedures (Table 5). This is similar to larger studies that have found no significant increase in operating time between open and laparoscopic surgery for inguinal hernia.2,12,17 The relative difference in cost between open and laparoscopic procedures directly contributes to the cost-effectiveness of each approach across the range of recurrence and metachronous hernia rates.
There are some limitations to our study. First, since our cases were gathered in reverse chronological order and overnight laparoscopic IH repair was less frequently performed in our institution than open repair, this group contains cases over a slightly longer time period (2018–2019) than the other groups (2019). However, it is unlikely a difference of a year would account for a large increase in costs. Second, this is a single-center study with a relatively small number of cases. Although it is likely that our findings are generalizable across the United Kingdom they may not be across all jurisdictions; in particular, attention should be paid to differences in how hospital costs are attributed across different health care systems.
Finally, our analysis has only considered cost related to need for further surgical intervention and not included the cost of treating other complications after surgery such as wound infection, or the cost impact of other patient-related outcomes such as testicular atrophy. However, studies have indicated that the complication rate between laparoscopic and open hernia repair are similar; therefore, the difference in technique should not alter the cost of these aspects. 7
The strengths of our study are in the use of a detailed micro-costing approach to assigning costs of each procedure on an individual case basis rather than relying on national tariffs, and the distinction between day case procedures and cases performed as an overnight stay. Since IH repair is frequently performed on young, sometimes ex-preterm infants, overnight stay after surgery may be indicated and it is important to understand the impact this has on relative cost-effectiveness of each surgical approach.
Ultimately, most recent data suggest equivalent clinical outcomes between open IH repair and laparoscopic IH repair.6–8 In an era where health costs are becoming increasingly scrutinized, surgeons should consider factoring cost into their decision making, and may in the future be required by their institutions. Future larger studies into the cost of laparoscopic and open IH repair in multiple centers across the United Kingdom and other health care systems would be beneficial in creating a more generalizable financial model. Furthermore, if a generalizable financial model were to be created, it could be used to determine which procedure is more cost-effective based on each institution or surgeon's individual metachronous and recurrence rate.
Footnotes
Acknowledgments
We thank Matthew Connell and Briony James who contributed to PLICS data collection.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding received.