
Abstract
Introduction:
Gastric volvulus (GV) is a rare and life-threatening condition if not promptly diagnosed and treated. Extreme rotation can cause obstruction cutting off blood supply to stomach and distal organs, leading to ischemia and necrosis. It is a clinically significant cause of acute/recurrent abdominal pain and chronic vomiting in children. GV can be classified into the following: primary, secondary, organoaxial, mesenteroaxial, or combined, acute, or chronic.
Materials and Methods:
Six neonates (5 males-1 female) were admitted to our department for recurrent postprandial vomiting associated with paleness, hyporeactivity, transitory abdominal distension, failure to thrive, and respiratory infections (only-1). Median age: 6 months (range 2–9 months). Patients metabolic and neurological evaluations were normal. A barium-swallow-study (upper gastrointestinal [UGI]) allowed definitive diagnosis.
Results:
UGI and esophagogastroduodenoscopy (EGDS) showed a gastric abnormal dilatation (gastric fundus), hiatal hernia (HH) in 5 patients, a large/small curvature discrepancy in 3 patients. Four were chronic-organoaxial-GV, 2 chronic-mesenteroaxial-GV. All underwent Laparoscopic-Hill-Snow-gastropexy (LHSG) with HH correction. No intraoperative/postoperative complications were recorded. Refeeding started in first postoperative day. Average hospital stay: 6-days. At long-term follow-up, all patients were symptoms free (able to vomit/burp); 2 referred occasionally epigastric pain sometimes with vomit. At 10–12 years follow-up UGI and EGDS confirmed correct gastric position revealing gastroduedenitis.
Discussion:
GV is a rare clinical entity in children considering etiology and management with an important morbidity and mortality rate. Its diagnosis could be missed simply. Vomiting or HH on imaging studies should suggest GV regardless patient's stable appearance.
Conclusions:
Chronic GV can manifest with atypical chest, abdominal, and gastrointestinal symptoms. Early diagnosis and treatment reduce the risk of developing acute form. LHSG is a long-term effective and safe solution with a very low complication rate, and no symptoms correlated to Nissen procedure.
Introduction
Gastric volvulus (GV) is defined as an abnormal rotation of all or part of the stomach at least of 180° around one of its axes causing obstruction. More frequent in adults, it has been described as a rare condition in children and infants, but it could be a life-threatening condition if not immediately recognized. It must be differentiated from “gastric torsion,” a rotation of the stomach of less than 180° 1 .
GV can be classified considering the onset (acute, chronic, or recurrent), the etiology (primary or secondary), the axis of rotation (organoaxial, mesenteroaxial, or combined).
In acute form presentation, GV could appear with the classical symptomatology of an upper gastrointestinal (UGI) tract obstruction with nonbilious vomiting and abdominal pain.
Instead, a history of chronic vomiting, abdominal distension, associated with failure to thrive, and possible episodes of chest infection could lead physician to suspect a chronic GV.
GV could be primary (or idiopathic) or secondary. Primary GV is associated with congenital defects (as the absence or laxity of gastric ligaments) or with an anomalous gastric distension.
Secondary GV occurs when rotation of the stomach is due to the malformations of the contiguous organs, the spleen (wandering spleen), diaphragm (congenital diaphragmatic hernia), or by a malfunction or a disorder that could affect the stomach (congenital bands).
According on the rotation's axis, the stomach could rotate along its longitudinal axis, passing through the cardia and pylorus leading to an organoaxial-GV (OGV). With this rotation, the greater curvature lies above the lesser one, leading to an “upside-down” stomach involving two sites of obstruction, the cardia and the pylorus. This is the most common 1 form and occurs in the two/third of cases.
Mesenteroaxial-GV (MGV) happens if the stomach twists around its short axis leading on a misplacement of the pylorus and the antrum above the gastroesophageal junction (GEJ). A rotation on both axes, longitudinal and short, occurs in the combined or mixed type GV. 2
Diagnostic criteria are not standardized yet. The suspicion of GV could be strengthened with a plain abdominal X-ray 3 and confirmed by UGI study and esophagogastroduodenoscopy (EGDS).
The treatment depends on GV type. Acute form of GV often requires immediate surgical treatment, including correction of associated defect. Chronic-GV usually requires a gastropexi.1,3
In this article, we want to describe our experience on GV treatment focusing overall on surgical treatment.
Materials and Methods
During the last 10 years, from 2008 to 2020, 6 patients were admitted to our Department of Pediatric Surgery at San Bortolo Hospital in Vicenza, Italy, with a diagnosis of chronic GV.
The data of all neonates with GV were retrospectively analyzed considering gender, onset symptoms, radiological imaging results, and treatment. Clinical characteristics of our patients are described in Table 1; five males and 1 female. Average age was 6 months (range 2–9 months); average weight 5500 g (3500–9000 g). Onset symptoms were a history of recurrent postprandial nonbilious vomiting (6 patients) associated with epigastric distension (6 patients), episodes of paleness, hyporeactivity to most stimulation (4 patients), and feeding intolerance (3 patients). Only one presented history of respiratory difficulties. Metabolic investigations were normal; neurological examinations resulted adequate to the age. Gastroesophageal reflux was documented in all patients. Research data have been approved by IRB.
Neonatal Gastric Volvulus Patients Clinical Characteristics
F, female; M, male; MA, mesenteroaxial; OA, organoaxial.
Imaging included abdominal plain radiographs and UGI contrast series. Diagnosis was confirmed in all patients by UGI.
Results
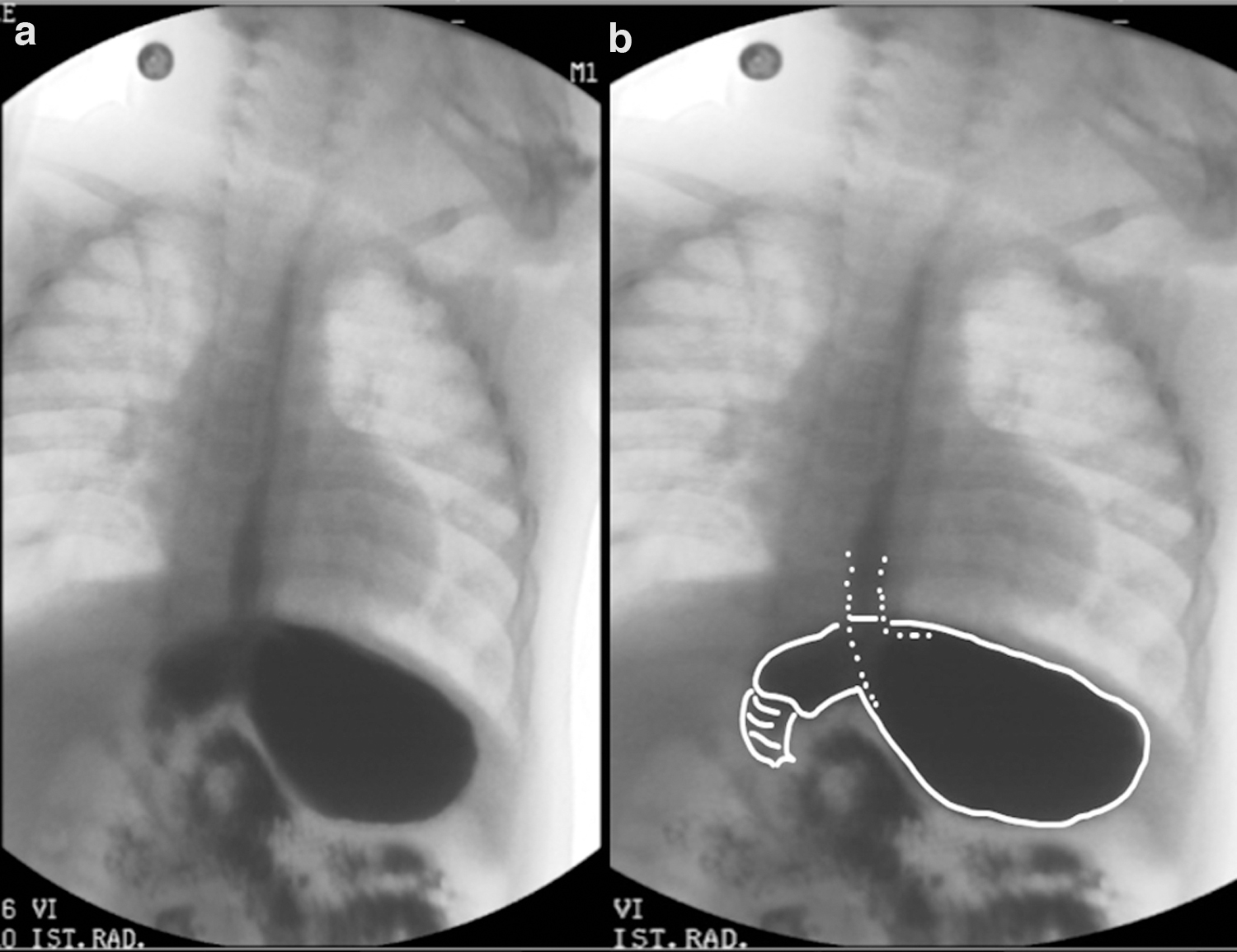
The first radiological finding in abdominal X-ray suggesting GV is the gastric double bubble, resulting from the overlap of two large bubble in epigastrium (Fig. 1), and anomalous gastric distension in all patients. UGI showed in 4 cases a gastric organoaxial twist along the longitudinal axis with the lesser curvature lying under the greater one (OGV; Fig. 2a, b), while in 2 cases, a rotation of the stomach along its horizontal axis (MGV). UGI series showed also in 3 patients a discrepancy between the greater and the lesser gastric curvatures (Fig. 3 ) and a distended horizontal stomach in 3 patients (Fig. 4a, b).

Plain abdominal radiograph showing double gastric bubble (star shows one bubble, arrow shows the other).
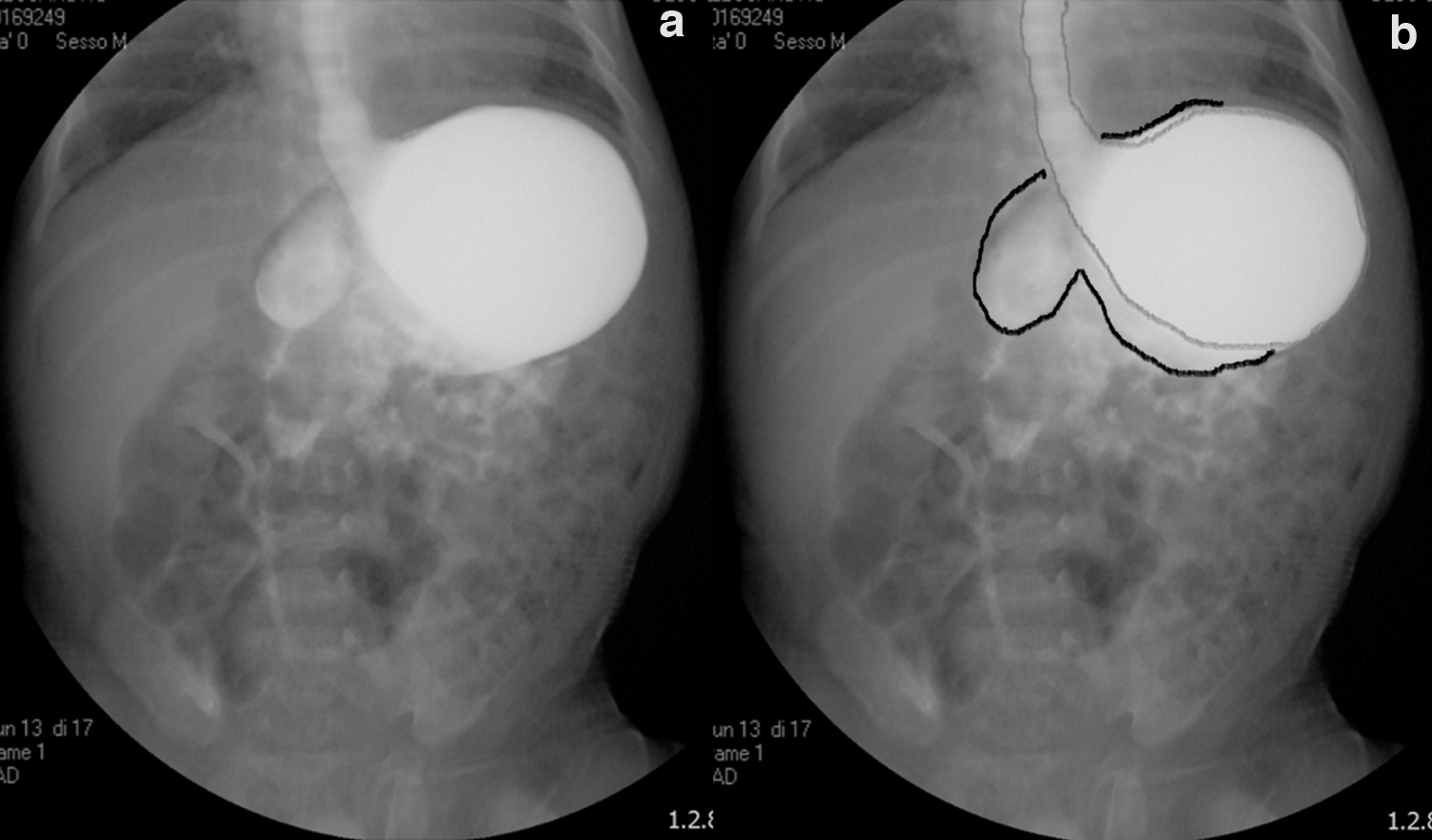
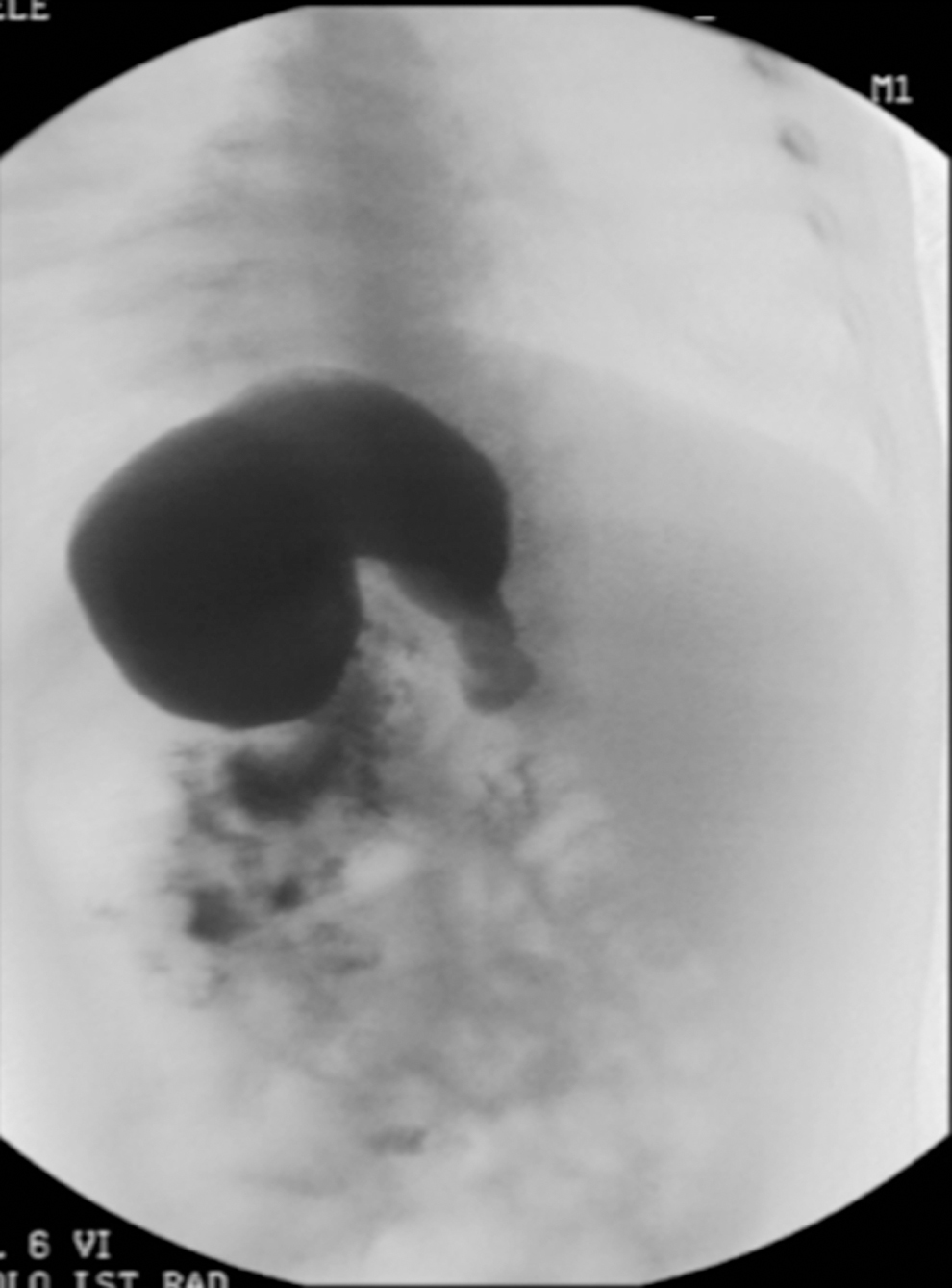
UGI showing a gastric reversal and discrepancy of the greater and lesser curvatures. UGI, upper gastrointestinal.
EGDS showed in 5 of 6 patients a hiatal hernia (HH), without mucosal alterations; in 1 case, we found at the retroverted view a peculiar mucosal fold that leads us to suspect a laxity of the ligamentous structures that usually fix the stomach to the abdominal wall (Fig. 5 ). All patients underwent laparoscopic-modified Hill-Snow posterior gastropexy. Neither intraoperative nor postoperative complications were recorded. All patients had a complete and very long follow-up: mean 60 months (2–12 years). They were evaluated with clinical examinations, barium swallow study at 6 and 12 months, and UGI endoscopy at 12 months. We had no relapse. All patients were symptoms-free. They started gradually oral intake (both liquid and solid) reaching the correct amount according to the age and weight of the patient without chronic episodes of vomiting.

Endoscopic view: at the retroverted view a peculiar mucosal fold expression of the laxity of the ligamentous structures that usually anchor the stomach to the abdominal wall.
In the first days in 2 patients, we recorded occasionally some episodes of regurgitation, while in 3 patients some episodes of vomiting spontaneously resolved. At long-term follow-up, all referred the ability to vomit, being able to burp. No gas-air-bloat and dumping were recorded and all the patients were symptoms free; 2 patients who referred occasionally epigastric pain sometimes had associated vomit. They had at 10 and 12 years after surgery a contrast study (UGI) and gastroscopy confirming the correct gastric position and anatomy but a gastroduedenitis; they were successfully treated with Proton pump inhibitors.
Operative technique
We performed a laparoscopic-modified Hill-Snow posterior gastropexy, to which we will refer in this article as Laparoscopic-Hill-Snow-Repair (LHSR). The goal of that procedure was to restore the normal anatomy of the “anti-reflux zone” by lowering the position of the cardia that causes the closure of the His angle rebuilding a continent but not stenosing hiatus. The Hill technique, born for surgical correction of HH and gastroesophageal reflux disease, represents a calibration of the cardia and a posterior gastropexy fixing the GEJ to the median arcuate ligament. It aims to restore the gastroesophageal valve system closing the esophageal hiatus reducing the HH with GEJ posterior fixation.2,4,5
In LHSR, we modified the Hill technique placing two-three sutures between the GEJ and the right crura just near the confluence of the two diaphragmatic pillars to support the maintenance of the cardias. This variation makes safer and less demolitive operation, in fact, the dissection down to the aortic arcuate ligament is not necessary. The patient was placed on the operating table in a 20°–45° supine frog-leg anti-Trendelenburg position allowing abdominal organs, in particular, the transverse colon and small bowel, to slide down toward the pelvis freeing the operative area. Instruments and trocars size depended on child-size. We used 3–5 mm instruments of 18–20 cm length and a 5 mm 30°angled laparoscope. Camera port was placed in the umbilicus through an open access incision.
After creating a pneumoperitoneum (4–6 mmHg) according to patient age, four trocars were placed (Fig. 6). Monopolar hook was used to open and split the gastrohepatic ligament preserving the bundle (hepatic branch of the vagus nerve), which runs in the “pars flaccida.” The peritoneal reflection overlying the anterior esophagus was opened exposing the right crura of the diaphragm. The dissection continues until the left pillar is identified. With the GEJ moved toward patient's right, dissection of the hiatus continues down the left crus until the confluence of the right and left crura is visualized and released. Then the GEJ is moved to the left side and lifted anteriorly allowing esophagus posterior dissection. The posterior vagus nerve is identified and mobilized with blunt and cautery dissection.

Trocar position: 5 mm camera port was placed in the umbilicus (red point); four 3–5 mm trocars site (yellow point).
Freed circumferentially, the esophagus is created a window behind the GEJ. A ribbon is placed to easily pull and move the esophagus and the GEJ facilitating the dissection. Esophageal dissection ends when a complete reduction of the HH, (if present) is obtained. Freeing the edge of the left crus is important to identify the anterior vagus nerve preserving it during dissection, so it remains with the esophagus. All vagus nerve branches were identified and preserved. Short gastric vessels, when present, were preserved too. The left and right crura were approximated using one to three interrupted 2/3–0 nonabsorbable sutures (according to the age and weight of the patient; Fig. 7).

The crura was approximated using one to three interrupted 2–0 nonabsorbable sutures.
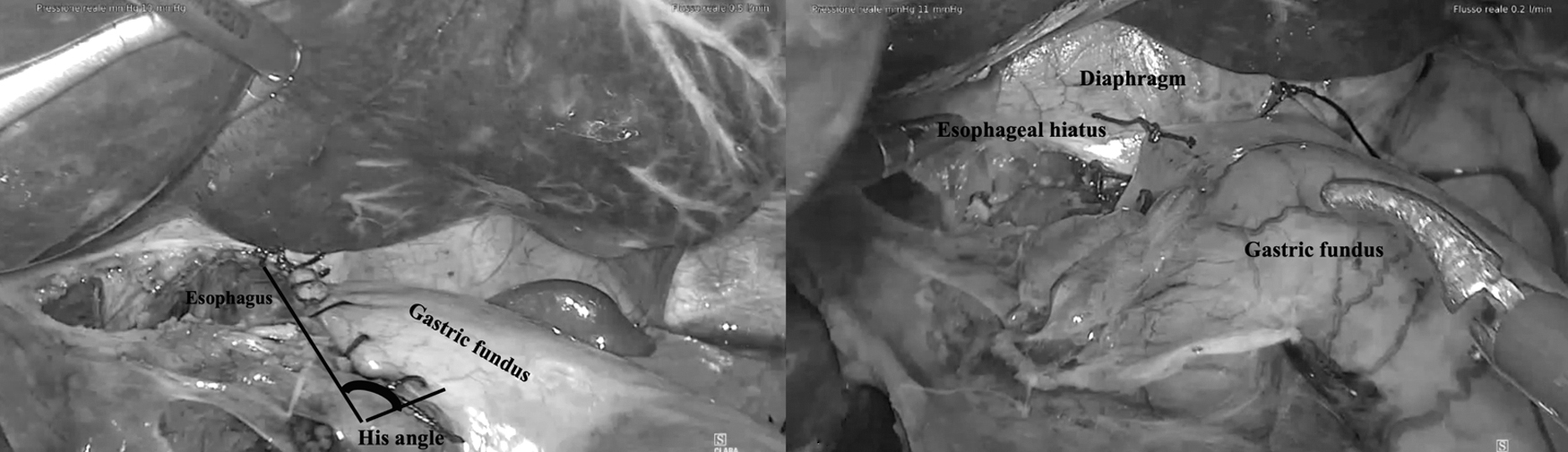
In the original surgical technique described by Hill, preaortic fascia was carefully identified to the emergence of celiac axis and 2/3 stitches were applied between the seromuscular layer of posterior gastric wall, the left crus and the left side of the preaortic fascia, preserving the posterior vagus nerve. We instead put two-three stitches between the GEJ and the right crura, just near the confluence with the left one (Fig. 8). Next step was to restore the His angle. Some not-absorbable stitches were applied between the apex of the gastric fundus and the diaphragm proximal to the esophageal hiatus followed by a not-absorbable suture (with continuous or separate stitches) between the gastric fundus and esophagus.

Posterior gastropexy: 1–2 stitches between the GEJ and the right crura to anchor posteriorly the stomach. GEJ, gastroesophageal junction.
To secure GEJ position and to avoid an intrathoracic sliding, two-three sutures were then placed among the fundus and the diaphragm and the esophagus and the diaphragm (at the hiatus; Fig. 9a, b). Correct position of the stomach is confirmed by the air gas filling test, inflating the stomach ascertaining the absence of torsion/rotation. In all patients, a nasogastric tube was placed inside the stomach during the procedure to help the dissection and was left in place after surgery for 1–2 days. Oral intake began in first postoperative day. Children were discharged on average at postoperative day. 6
Discussion
Although a rare condition in the pediatric population, GV is a potential life-threatening condition that, if not promptly recognized and treated, could be fatal. Early presentation in neonatal age is estimated to be around 26% of all cases. 6 It is very important to be aware of that condition since the prognosis of the patient depends on opportune diagnosis. 7 In fact, an immediate diagnosis and treatment will reduce the risk of developing acute GV from a chronic form. Acute GV in children is frequently associated with anatomic defects,2,3 while usually, chronic GV is idiopathic and only in a small number of cases is associated with or functional anomalies or anatomic malformations of other organs. 1 The clinical diagnosis of neonatal GV is very difficult and complicated. Several reports described a missed or delayed diagnosis caused by the presence of aspecific clinical symptoms.
Another reason of missed or delayed diagnosis often could be the unawareness of pathology; usually an incidental diagnosis of GV is obtained with UGI contrast-study performed for other diseases (as reflux).8,9 While in the acute form the symptoms are clear with nonbilious vomiting combined with abdominal pain; in chronic GV, symptoms are very often mistakable making the diagnosis very difficult. Chronic vomiting, abdominal distension and failure to thrive are typical symptoms of the chronic form of GV, but are nonspecific to make diagnosis resembling other conditions and leading to delay. Usually, in our experience, the diagnosis after suspicion of GV comes from the combination of plain X-rays, UGI contrast series, and EGDS.
Tanner in 1968 described various methods of surgical repair for GV, 10 which included gastrostomy, simple gastropexy, or other techniques. Many of them nowadays have been replaced with minimally invasive procedures. Endoscopic derotation of the stomach or PEG tube placement has also been reported to have success.11,12 Laparoscopic anterior gastropexy is reported in treatment of GV with success. Although the report of laparoscopic approach in correction of GV has recently come to be seen (essentially in adults), there are no standardized procedures described.13,14 However, recurrent GV are reported after endoscopic or surgical gastrostomy tube positioning or anterior gastropexy. There are no reports underlining the need of surgical antireflux correction during surgical repair for both primary or secondary GV.
An association between GERD and chronic GV has been described, although there are no reported cases of gastroesophageal reflux disease in pediatric age with acute GV, Cribbs reported radiological signs of GERD at the time of GV diagnosis in 44 (13%) of 329 children with chronic GV. 2 Conservative solutions for chronic GV are also reported: antacid therapy with proton pump inhibitors, proper diet with thickening of meals, and modifications of posture (with patient in upright position during feeding and modifying the position with right side down ore prone after feeding). 14 No follow-up and outcome data of this condition are reported. 15 In this article, we show the Hill-Snow technique (a posterior gastropexy), and it could be a real asset in treatment of GV. Its goal is to recreate the His angle, to anchor posteriorly the GEJ guaranteeing a fixation system that avoid any twist of the stomach.
LHSR is a feasible technique that represents also a physiologic correction of reflux restoring the normal anatomy and physiology. This procedure is characterized by a great long-term durability and a significant improvement on postoperative quality of life comparable with the open Hill repair (85% good to excellent results with a median follow-up of 19 years and a reoperation rate under 10%). Hill fixation of GEJ to the preaortic fascia can ensure a structural integrity compared to other repairs. 3 In our experience, we obtained similar results avoiding the fixation to the preaortic fascia and fixing GEJ to the right pillar of the diaphragm near the crus confluence. Minimally invasive correction is an effective and safe procedure with a reduced complication rate, rapid resumption of feeding and excellent aesthetic results.
Preferred surgical approach for GV includes variations of gastropexy. Esophageal stenosis is the most common complication after GV management. 16 According to our experience, this surgical approach is even more indicated for long-term results; a 14-year follow-up in our series with correct gastric position at UGI and absence of symptoms and morbidities.
Conclusion
GV is an extremely rare disorder that could lead to life-threatening consequences if not recognized and well treated. The chronic form is challenging to identify and need a strong knowledge and awareness of the pathology. Symptoms' resolution represents the target to be achieved after surgical correction. Conservative management can be successful if the warning signs as weight loss, abdominal pain, and worsening of symptoms are not present. We must consider that acute GV is characterized by a mortality rate more than twice of chronic form. Overall mortality rate reported for chronic GV is 2.7%, including 0.8% mortality rate of patients treated conservatively. For this reason, surgery, according to us, LHSR, could be considered an effective procedure in treatment of GV. Although no data are reported by literature about the follow-up of these patients, reduction or resolution of symptoms with an improved nutritional status could represent the main prognostic factors.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.