
Abstract
Background:
This study aimed to create a consensus statement on the indications, applications, and limitations of robotics in pediatric urology.
Methods:
After a panel and interactive discussion focused on pediatric robotics, a televoting with 10 questions was administered to 100 pediatric surgeons/urologists attending the joint meeting of the French Group of Pediatric Laparoscopy (GECI)/Italian Society of Videosurgery in Infancy (SIVI) in 2021. The results of televoting were analyzed electronically using Mentometer software.
Results:
Ninety-four percent of participants stated that the cutoff weight for robotics should be >10–15 kg. A minimum of 20–30 procedures should be performed to become confident in robotics (74%). Pediatric urology is the main field of application (73%) and pyeloplasty is the best indication for robotics (63%). Technical problems may happen intraoperatively in 1/10–15 cases (64%). The mean duration of robotic procedures ranges from 150 to 200 minutes (72%). The main drawbacks of robotics are high costs and limited development of miniaturized instruments (74%). Ninety-five percent believed that the costs of robotics may significantly drop with the availability of more robotic brands. The main advantages of robotics over laparoscopy include improved dexterity, easier suturing, and better ergonomics (100%), whereas the main disadvantage of sharing the robot with other specialties is the wearing out of instruments (100%).
Conclusions:
This is the first consensus statement, endorsed by the GECI and SIVI societies, on the use of robotics in pediatric urology. The need to introduce more robotic brands on the market to lower the costs and to develop miniaturized instruments to be adopted in infants less than 10 kg emerged. Pediatric urology is the main field of application of pediatric robotics, and robotic pyeloplasty is the most common procedure performed. Proctorship is needed for the first 20–30 procedures and technical problems may occur intraoperatively in 1/10–15 cases. The main advantages of robotics over laparoscopy are improved dexterity, easier suturing, and better surgeon ergonomics.
Introduction
Laparoscopic surgery revolution in the 1990s changed completely the field of surgery in adults and also in pediatrics.1–3 However, after 30 years of minimally invasive surgery (MIS), intracorporeal suturing and knotting in laparoscopy remain still challenging. 4 More recently, the robotic platform has been introduced, providing improved dexterity with 7 degrees of freedom of movement of the robotic arms.5–8 In the last 10 years, robot-assisted laparoscopic surgery using the da Vinci surgical system (Intuitive Surgical, Inc., Sunnyvale, CA, USA) has increasingly been adopted also in pediatric patients.9–12
As reported in adults, the robotic platform's advantages in children include stable magnified three-dimensional view, tremor filtering, better ergonomics, and motion scaling allowing for more precise intracorporeal exposure and easier suturing also in narrow spaces.13–15 Common drawbacks include the larger diameter of trocars (8 mm) compared with the smaller laparoscopic ports (3 mm) adopted in children, the size of robotic platform that limits its use in newborns and in small infants, and above all the huge costs of acquisition of robot and robotic instruments that have a limited life span. 14
Analyzing the international literature published over the last 5 years, several articles focused on pediatric robotics have been published.—16–21 However, most of them are small series of single-center experience or multicentric reports, but no consensus statements are available regarding the use of robotics in the pediatric population.
For this reason, during the 2021 joint meeting of the French Group of Pediatric Laparoscopy (GECI) and the Italian Society of Videosurgery in Infancy (SIVI), a panel on pediatric robotic surgery was formed among the main European experts. Based on the results of interactive discussion and televoting, a consensus statement on the indications, applications, and limitations of robotics in pediatric urology was created and endorsed by these two organizations.
Materials and Methods
After 2 years of the COVID-19 pandemic, when all the educational activities were performed using webinars, a joint meeting between GECI and SIVI was held in Naples, Italy, in July 2021. During this meeting, 100 pediatric surgeons/pediatric urologists, mostly coming from the European countries such as France, Italy, Switzerland, Luxembourg, Spain, Belgium, and United Kingdom and also from extra-European countries, met to discuss together about MIS. A panel that focused on the applications and indications of pediatric robotic surgery was formed among the main European experts of robotics. After an interactive discussion, a televoting was performed using Mentometer software.
The following 10 questions with multichoice answers were administered to all participants: (1) The cutoff weight of children to be operated in robotics; (2) the duration of learning curve for pediatric robotics; (3) the main field of application of robotics in pediatric age; (4) the best indication for pediatric robotics; (5) the frequency of intraoperative technical challenges found in robotics; (6) the mean duration of robotic procedures in pediatrics; (7) the main drawbacks of pediatric robotics; (8) do you think that by increasing the number of robotic brands, the cost of robotics will be lower? (9) the main advantages of robotics compared with laparoscopy; and (10) the main disadvantage of sharing the robot with other specialties.
The 10 questions of televoting are reported in Table 1.
The 10 Questions of Televoting
3D, three dimensional; GI, gastrointestinal.
One hundred pediatric surgeons/pediatric urologists participated in the panel and televoting. The results of televoting assessed electronically by Mentometer software were analyzed by the experts of pediatric robotics involved in the panel with the aim to create a consensus document on the use of robotics in pediatric urology. Appropriate Institute Review Board (IRB) approval was received for this study.
Results
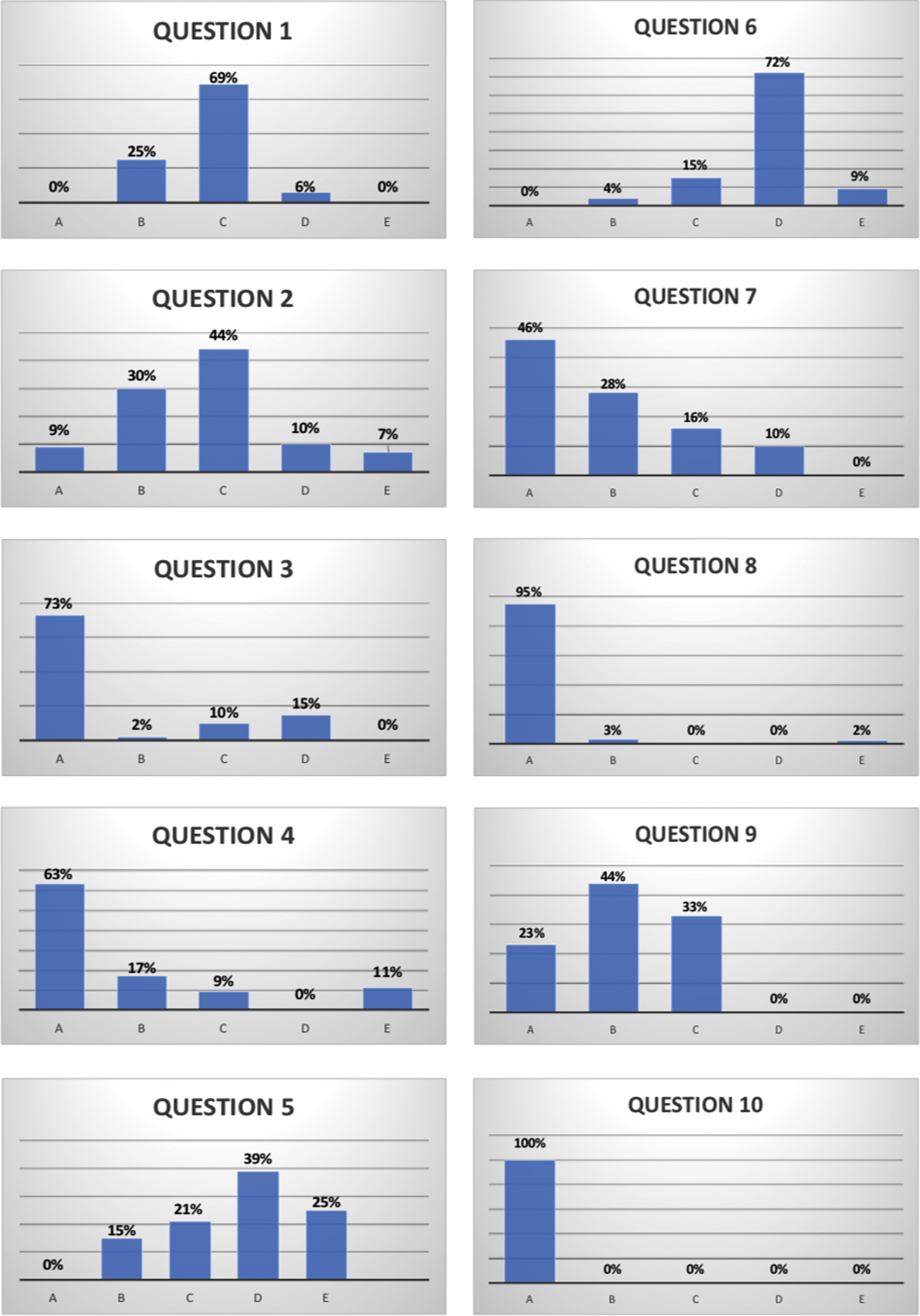
Regarding patient weight, 94% of the participants stated that the patient's cutoff weight for robotics should be >10–15 kg. Regarding the learning curve, 74% of the pediatric surgeons believed that at least 20–30 procedures should be performed under the supervision of a proctor to become confident in robotics. Pediatric urology is the main field of application of pediatric robotics according to 73% of voters, and pyeloplasty for uretero-pelvic junction obstruction was considered the best indication for robotics by 63% of voters. Sixty-four percent of participants stated that technical problems using a robot may happen intraoperatively in 1/10–15 cases. The main duration of robotic procedures ranged from 150 to 200 minutes according to 72% of voters.
Seventy-four percent of participants stated that the main drawbacks of robotics are the high costs and the limited development of miniaturized instruments. Ninety-five percent of pediatric surgeons believed that the cost of robotics may significantly drop with the availability of more robotic brands on the market. The totality of voters stated that the main advantages of robotics compared with laparoscopy include improved dexterity, easier suturing, and better ergonomics for the surgeons. Finally, 100% of pediatric surgeons stated that the main disadvantage of sharing the robot with other specialties is the wearing out of robotic instruments that become malfunctioning after seven to eight consecutive uses.
The results of televoting are reported in Figure 1.
Results of televoting. Color images are available online.
Discussion
Pediatric urology is one of the surgical fields that mostly benefit from technical facilities provided by the robotic platform,10–15 and many studies have demonstrated the advantages of robotic technology to treat bladder, ureteral, and renal pathologies.8,19–22
However, robots are designed for adults and robotic instruments have a diameter of 8 mm compared with the smaller diameter (3 or 5 mm) of laparoscopic instruments usually adopted in children. Moreover, several other limitations to the widespread adoption of robotic technology in pediatrics have emerged such as the high costs of robotic procedures, the large size of the robot itself, and the lack of large case series and randomized controlled trials in pediatric patients.23,24
Analyzing the international literature of the last 5 years, no international consensus about the use of robotics in pediatric urology has been established until now. For this reason, we caught the occasion to meet some of the main European experts of pediatric robotics, who attended the joint GECI/SIVI Meeting in July 2021, to organize a panel on this topic and to create a consensus statement using the televoting system. After the panel's expert lectures and a long interactive discussion, a televoting was performed based on 10 multiple choice questions. The questions asked assumed objective answers, based on data rather than on individual participant opinions. The survey was intended as a means to collect the experience derived from the daily practice of different surgeons, report it as objective data, and to convey it into a consensus statement that was endorsed by the two societies of pediatric MIS, GECI and SIVI.
Important considerations on the advantages and limitations of pediatric robotics emerged from the analysis of the televoting results.
First, the use of robot is currently limited to patients >10–15 kg, due to the huge dimension of the robotic platform and the size of robotic instruments (8 mm). In infants and small babies, we do not have the object space to place a minimum number of three 8-mm robotic ports and eventually a 5-mm accessory port. So, there is the real need to develop miniaturized robotic instruments to make robotics feasible also in infants and patients less than 10 kg.
The main field of application of robotics in pediatrics is represented by urological indications, and pyeloplasty is the most common procedure performed robotically, although extravesical ureteral reimplantation and bladder reconstruction are further excellent indications. In fact, pyeloplasty represents the procedure in which the technical advantages of robot technology, allowing easier intracorporeal suturing and dissection in difficult cases, such as redo-procedures or complex anatomy, are more evident [21]. Although the learning curve reported for robotics is shorter compared with laparoscopy and is mainly related to the possibility of training on a robotic simulator, a proctorship period seems to be mandatory in the clinical practice for at least 20–30 consecutive robotic procedures, to learn more rapidly the tips and tricks of this technology.
Based on their personal experience, most of participants answered that technical problems with robotics may happen intraoperatively, with a frequency of 1/10 or 1/15 cases. Thus, another advice is to have a robot staff member in the operating room during the early robotic experience, to receive technical assistance in case of intraoperative challenges with the docking or instrument manipulation.
Regarding the length of robotic operations, the mean duration of robotic procedures was about 150–200 minutes for most pediatric surgeons. The duration of robotic procedure was intended as the entire time spent in the operating room, from the initial phase of preparation and installation of the robot, called docking, that may range between 45 and 60 minutes during the early experience, till to the removal of surgical drapes. For this reason, not only the console surgeons but also all the members of the robotic team, including nurses and anesthesiologists, should be well trained to optimize the operating times.
According to 74% of participants, the main drawbacks of robotics are represented by the high costs of robot and limited availability of miniaturized robotic instruments. They believed that the one main limitation of robotics compared with laparoscopy is also the limited number of robotic instruments. In general, few instruments are adopted in each robotic procedure (scissor, needle-driver, Maryland bipolar forceps, grasping forceps) and the repeated change of the instruments during the procedure may be time-spending. For this reason, a useful trick is to place an accessory laparoscopic trocar for the bedside surgeon in all robotic procedures. However, the position of the assistant port, sometimes very close to the robotic ports, may limit the movements of the bedside surgeon, who is often conflicting with the robotic arms.
This challenge can compromise the performance of the assistant surgeon, who plays a key role during the procedure, such as to introduce and remove sutures, to cut stitches, to position clips, or to help in tissue retraction.
One of the main limitations to the widespread diffusion of robotic surgery in the pediatric population is the monopoly of a unique robotic brand in the marketing. In fact, most of experts agreed with the need to introduce more robotic brands on the market to lower the costs of robotics.
The main advantages of robotics compared with laparoscopy include easier suturing, better surgeon ergonomics, and improved dexterity.
Considering that the exclusive use of a robot for pediatric patients in a single institution is not a cost-effective solution for the hospital, in most centers, the same robotic platform is shared between different surgical specialties (urology, general surgery, gynecology, pediatric surgery). The major disadvantage of sharing the robotic platform with other specialties is the wearing out of robotic instruments that have a life span of 10 uses. Some surgeons observed in their practice that robotic instruments became already malfunctioning after seven to eight consecutive uses.
Conclusions
After 20 years of experience of pediatric robotics (2001–2021), this is the first consensus statement that focused on the use of robotics in pediatric urology and endorsed by two societies of pediatric MIS, GECI and SIVI. New interesting data about the indications, applications, and limitations of pediatric robotics have emerged, such as the need to introduce more robotic brands on the market to lower the costs and to develop miniaturized instruments to be adopted in infants less than 10 kg. Pediatric urology seems to be the main field of application of pediatric robotics, and robotic pyeloplasty is the most common procedure performed. Proctorship is necessary for the first 20–30 procedures and technical problems may occur intraoperatively in 1/10–15 cases.
The main advantages of robotics over laparoscopy are improved dexterity, easier suturing, and better surgeon ergonomics. However, robotics is a very dynamic field and with the development of new technologies such as virtual reality, artificial intelligence, and 5G technology, robotics will have further development and larger application also in pediatric surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.