
Abstract
Objectives:
One lung ventilation (OLV) is the preferred ventilation technique for thoracoscopy as it provides a better exposure of the operative field and grants the protection of the healthy lung. Preoperative evaluation of lung exclusion is necessary and different methods are available. In recent years lung ultrasound (US) gained popularity and its use for monitoring the endotracheal tube position is widely reported. The existing evidence on adults addresses lung US as effective, yet only few data are available in children. Therefore, we present our experience with lung US as verification method for pediatric OLV.
Methods:
All patients undergoing OLV for video-assisted thoracoscopic surgery from January 2019 to May 2021 and for whom lung exclusion was confirmed through lung US were involved. Lung exclusion was considered effective when absence of lung motion and presence of lung pulse were encountered. When lung US did not match these criteria, repositioning of the endobronchial device followed by US verification was performed. When lung US met the exclusion criteria surgery was started and direct thoracoscopic observation was used to verify lung exclusion.
Results:
A total of 20 patients, accounting for 22 procedures, were involved. Absence of lung motion and presence of lung pulse were assessed in the operative-side lung for all patients. Lung exclusion was confirmed through thoracoscopy. Postoperative lung US proved the reappearance of lung motion in the previously excluded lung.
Conclusions:
In our center experience lung US resulted to be a safe, effective, and time-saving verification method for OLV. Further studies are needed to define its sensitivity and specificity.
Introduction
Video-assisted thoracoscopic surgery (VATS) is the gold standard approach for a wide range of pediatric diseases and congenital malformations. The main indications for VATS are lung congenital malformations, esophageal atresia, congenital diaphragmatic hernia, mediastinal or pulmonary cancer, diaphragm relaxation, and foregut duplication.1,2
Compared with thoracotomy, benefits of a minimally invasive approach are commonly accepted, such as less postoperative pain, faster recovery, lower rate of chest wall and spinal deformities, and better cosmesis.1,3,4
Integral with VATS is one lung ventilation (OLV), which provides a better exposure of the operative field and grants the protection of the healthy lung from contamination, while guaranteeing adequate blood oxygenation. 5
Studies on both adults and children provided evidence of a lower rate of conversion to open surgery when OLV is performed and confirmed feasibility and safety of this ventilation technique.6,7
After placing the endobronchial device, preoperative evaluation of proper lung exclusion is mandatory and it can be assessed through different confirmation methods, commonly divided into invasive and noninvasive.
The invasive methods comprehend fluoroscopy and bronchoscopy, both specific and sensitive but risk-exposing approaches. 8 The latter ones comprehend chest wall movements observation and pulmonary auscultation, both risk-free approaches but lacking in specificity and sensibility. 9
In recent years, lung ultrasound (US) gained popularity and its use in the monitoring of the endotracheal tube position is widely reported. Available evidence in children mostly refer to emergency intubations in an intensive care setting.10,11
Moreover, studies on adult patients undergoing VATS proved its effectiveness in the preoperative assessment of the position of the double-lumen tube. 12 This is because of distinctive sonographic signs, distinguishing a normal ventilating lung from a lung excluded from ventilation.13,14
The application of perioperative lung US in children is poorly described and only few reports outline it as verification method for OLV. 8
This study aims to report our experience with the point-of-care lung US as verification method for OLV in children undergoing VATS.
Materials and Methods
This series involves all patients undergoing OLV for VATS at the Pediatric Surgery Unit—Padova University Hospital, from January 2019 to May 2021. All patients for whom lung exclusion was preoperatively confirmed through lung US were included.
The patients' gender, age, and weight at intervention and pulmonary disease were collected.
Following the anesthesiologist's preference and after anesthesia induction, right lung exclusion was obtained by placing an Arndt Endobronchial Blocker in the right bronchus; conversely, left lung exclusion was performed through selective right mainstem intubation for all patients.
Preoperative lung US was performed to assess proper lung exclusion. A SonoSite M-turbo® US with a 6–13 MHz linear transducer was used. US examination was performed between the second and the fourth intercostal space in mid-clavicular line and between the fifth and the sixth intercostal space in the anterior axillary line, with the patient in supine position.
Sonographic criteria for lung exclusion were the absence of lung sliding and presence of lung pulse in the operative-sided lung. Chest movements observation and pulmonary auscultation were used as complementary verification methods.
In the absence of the aforementioned criteria repositioning of the endobronchial tube or the bronchial blocker was performed and lung US was repeated.
When lung US met the exclusion criteria, surgery was started and direct thoracoscopic lung observation was used to confirm lung exclusion.
Intraoperative monitoring was assessed through serial arterial blood gas analysis, blood oxygenation values, and the MostCare® device (Pressure Recording Analytical Method).
At the end of surgical dissection, pulmonary reinclusion was carried out under direct thoracoscopic vision.
Postoperative lung US was performed to verify the reappearance of lung sliding in the operative-sided lung and demonstrate a proper restoration of the parenchymal atelectasis areas determined by previous exclusion from ventilation.
Results
Twenty patients were treated during the study period, for a total of 22 procedures. Four patients underwent VATS for left bronchopulmonary sequestration, 6 for left congenital cystic adenomatoid malformation (CCAM), 2 for right CCAM, 1 for right mediastinal bronchogenic cyst, 2 for spontaneous or pulmonary metastasis-related pneumothorax, 1 for left mediastinal lymphangioma, 1 for right congenital diaphragmatic hernia recurrence, 2 for left pulmonary tumor, and 1 for left posterior mediastinal tumor.
Median age and weight at intervention were 16 months and 11 kg, respectively. A resume of patients' demographics can be found in Table 1.
Summary of Patients' Characteristics
BPS, bronchopulmonary sequestration; CCAM, congenital cystic adenomatoid malformation; CDH, congenital diaphragmatic hernia.
The excluded lung was evaluated through lung US and the preoperative sonographic findings (absence of lung sliding and presence of lung pulse) were confirmed through thoracoscopic observation of complete lung exclusion in all patients. No patient required invasive verification methods (e.g., bronchoscopy) to be used. Only 1 patient of our series required conversion to open surgery due to the displacement of the endobronchial blocker and development of a poor responding hypoxia.
Discussion
One lung ventilation
Regardless of the well-described advantages, OLV comes with several technical challenges, especially in the pediatric field. Although is easier to perform in older children, OLV is viable starting from 6 months of age or 2.5 kg and becomes extremely helpful in case of small operative fields. 15
The exclusion of the operative-sided lung can be difficult in young children, first due to anatomical factors. The narrow and short airways expose children to a higher risk of mucosal damage and tracheal tube or bronchial blocker displacement. Moreover, a softer rib cage makes children more prone to hypoxia when lateral decubitus is required. 16
Several approaches are available for OLV and mainly depend on the child airways' size and the anesthesiologist's expertise and preference. 15
To reach lung exclusion, double-lumen endobronchial tubes or Univent tubes are generally used in children older than 8 years, as the smaller devices available correspond to a 26F or a 6.5 cuffed tracheal tube. 17
Conversely, OLV in small children is mainly obtained through selective mainstem intubation or placement of an endobronchial blocker. 5
The mainstem intubation usually require a single-lumen tracheal tube half a size smaller than the suitable endotracheal tube. 18 Right intubation might easily be performed blindly (although it is advisable to check the positioning), whereas left intubation often requires a fiber optical bronchoscopy guidance. 19 Disadvantages of the selective mainstem intubation are a less effective lung isolation and the difficulty to intraoperatively manage the tube in case of displacement or obstruction. 17
For the bronchial blocker placement our center's preference involves the use of an Arndt endobronchial blocker, a balloon-tipped catheter with a high volume, low pressure balloon, and a three-way adaptor, granting ventilation of the child during the device positioning.
The bronchial blocker is generally placed externally to the endotracheal tube and the balloon inflated under direct vision. Regardless of the technical challenges for its placement, main advantage of the bronchial blocker is the possibility to quickly switch from OLV to double lung ventilation if necessary. 16
OLV verification methods
Preoperative confirmation of lung isolation is fundamental to provide an adequate vision of the surgical field. To comply with this, the ideal OLV verification method should be at the same time safe and effective.
Pulmonary auscultation and chest movements observation are simple techniques and do not require a special equipment (Supplementary Video SV1). Nevertheless, they cannot be considered reliable methods as both approaches lack in sensibility and specificity, eventually leading to an inaccurate evaluation of lung ventilation.9,20
Bronchoscopy and fluoroscopy are fairly accurate to assess the position of the endobronchial device, even though both procedures are time consuming and expose the child to mechanical and radiological risks, respectively. 8
At present, fiber-optic bronchoscopy is the gold standard procedure to confirm OLV (Supplementary Video SV2). Disadvantages of this method are the potential risk of desaturation (due to children low oxygenation reserve), risk of mucosal damage and difficulties to define the anatomy of children's airway.7,21
Fluoroscopy is scarcely used, especially in the pediatric population, to avoid X-ray exposure. 22
The use of lung US relies on characteristic signs that distinguish a normally ventilated lung from an excluded one.
The lung sliding, deriving from the slippage of the pleural sheets, is present in the well-ventilated lung, whereas is absent in the excluded one (Supplementary Videos SV3 and SV4); it varies depending on the compliance and the tidal volume, which makes it a good continuative monitoring method for ventilation. 13
In addition, the application of Motion-mode in a well-ventilating lung determines the appearance of multiple horizontal lines below the pleural sheets, resulting in the seashore sign (Fig. 1). 23 Conversely, the lung pulse, consisting of a heartbeat-synchronous movement transferred to the pleural line, is commonly appreciated in the excluded lung (Supplementary Video SV5). Lung pulse was proved to have a 93% sensitivity and a 100% specificity in the identification of lung collapse. 14
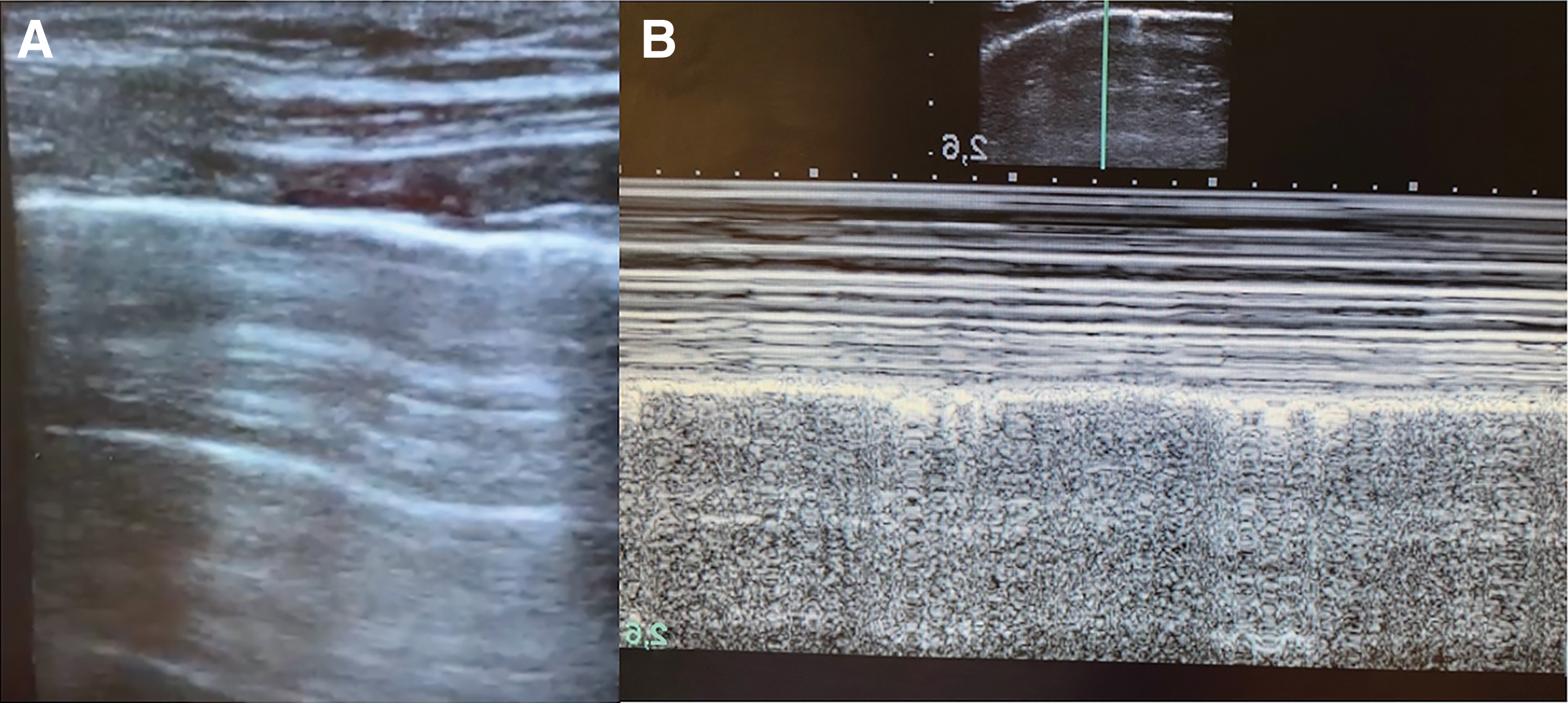
Seashore sign in Brightness-mode
Through the demonstration of lung pulse in the operative-sided lung and lung sliding in the contralateral, functional isolation and correct positioning of the bronchial blocker or the endotracheal tube can be assumed. 14
In recent years, some studies evaluated these ultrasonographic signs to assess the regional distribution of ventilation and concluded that lung US is a noninvasive and simple technique.12,24
The use of lung US to preoperatively confirm lung exclusion can be effective and less time consuming compared with the currently used methods. In addition, even though it is a point-of-care specialist technique, the presence of two well-established signs, distinctive for lung ventilation, might increase its accuracy.
Limitations of this verification method must be taken into account and mainly derive from the impossibility to evaluate the lung sliding in cases of pneumothorax, pleural adhesion, and subcutaneous emphysema.13,25,26 Subsequently, a complete preoperative ultrasonographic evaluation of both lungs is required to verify the presence of lung sliding before the exclusion.
In our center experience point-of-care lung US resulted to be an effective, safe, and time-saving technique to verify OLV. In our series, sonographic signs defining lung exclusion were always present after the placement of the endobronchial device. As a result we avoided our patient a second bronchoscopy, diminishing the risk of hypercapnia and mucosal damage.
To the best of our knowledge this is the first series focusing on the use of lung US for OLV in a perioperative setting and a pediatric population. Anyhow, the existing literature on lung US for the verification of the endobronchial tube position proved lung sliding to have a high positive predictive value for lung ventilation, mostly in emergency intubation.10,27
Based on our findings a combined use of lung US and noninvasive verification methods (chest movements observation or auscultation) should be effective to verify preoperative lung exclusion and postoperative lung reinclusion.
Further prospective trials are needed to assess lung US sensibility and specificity with reference to OLV.
Main limit of this study is the lack of a control population.
Other weaknesses are represented by the small sample size and the limited presence of parenchymal lung disease in the included patients. Finally, lung US was only performed by an expert anesthesiologist (C.T.). In this scenario, the effectiveness of the technique might be overestimated.
Conclusions
The ideal perioperative verification method for OLV should be at the same time safe and effective. Existing methods either lack in sensibility and specificity or expose the patient to mechanical and radiological risks.
In our center experience lung US proved to be an effective, safe, and time-saving technique to identify correct lung exclusion. Further prospective comparative studies evaluating lung US effectiveness and the accuracy of lung sliding and lung pulse as ventilation indicators are needed.
Footnotes
Authors' Contributions
C.T. and R.P. provided study conception and design, data collection, data analysis and writing—first draft and revised versions. P.G. provided study conception and design, writing—first draft and revised versions. S.P., G.C., and C.E. provided data analysis and writing—revised versions. All authors read and approved the final version of the article.
Disclosure Statement
All authors declare no conflict of interest.
Funding Information
All authors declare that no funding was received for this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.