
Abstract
Background:
The hand-assisted laparoscopic splenectomy (HALS) approach overcomes the difficulties experienced with conventional laparoscopic splenectomy (LS) with added advantages. In this study, we compared the HALS technique with standard LS based on the feasibility and intermediate postoperative outcomes in pediatric patients.
Methods:
We retrospectively investigated pediatric patients who underwent HALS or LS from October 2013 to May 2021 at the Children's Hospital, Chongqing Medical University. Potential parameters related to HALS or LS were explored, and the intermediate-term clinical outcomes were compared between the two groups. The quality of life and splenic regrowth data were followed up routinely for 12 months after the operation.
Results:
In total, 39 patients underwent splenectomy (11 for HALS and 28 for LS) and were eligible for this research. Patients who underwent HALS had a greater proportion of focal benign splenic lesions (P < .001) and partial splenectomy (P < .001). The HALS operative time was reduced compared with LS (P = .032). No operation conversion was noted in the HALS group, whereas 4 (14.3%) cases were converted to an open operation (P = .249). For partial splenectomies, favorable outcomes with HALS, including short operative time (P = .001) and reduced blood loss (P = .014), were noted compared with LS. No postoperative mortality was observed. During the follow-up period, a good quality of life and splenic regrowth were noted for most of the patients.
Conclusions:
Although another incision is necessary, HALS confers the advantages of a minimally invasive technique to manage the fragile spleen, especially in pediatric patients requiring partial splenectomy.
Introduction
With advancements in laparoscopic techniques, laparoscopic splenectomy (LS) has become more effective and secure for various diseases requiring splenectomy.1,2 LS offers several benefits, including minimal abdominal wall injury, short postoperative stay, reduced postoperative pain, and cosmetic outcome.3,4 However, due to the challenging laparoscopic skills required in LS and the complicated blood supply of the spleen, intraoperative bleeding is an essential barrier against the application of LS, especially for some situations involved in laparoscopic partial splenectomy (LPS).
In this situation, hand-assisted laparoscopic splenectomy (HALS) is proposed and advocated to control intraoperative bleeding with the advantages of both LS and open surgery (OS).5,6 The HALS could maintain the tactile features of OS, which are beneficial to bleeding control; furthermore, it is not necessary to expand the incision more than that noted for LS, which is associated with a low conversion rate and short operative time. 7 We have practical experience with the hand-assisted technique for a number of years to treat pediatric patients with the need for splenectomy. We have also performed temporary splenic artery occlusion to control intraoperative bleeding during LS for several years. However, there is still a lack of widely recognized evidence supporting this practice.
In this study, we performed a retrospective review of patients who underwent LS and HALS in our institution from October 2013 to May 2021. We aimed to compare the outcomes for the two approaches to share our experience with this minimally invasive technique.
Materials and Methods
Patient collection
LS and HALS were adopted in our institute in January 2010 and were subsequently applied to appropriate cases. Between January 2012 and May 2021, 62 patients underwent LS at Chongqing Children's Hospital, Chongqing Medical University. Indications for LS included benign splenic lesions for partial splenectomy and splenomegaly of various origins for whole LS. We retrospectively reviewed the detailed patient inpatient or outpatient medical records with institutional ethics committee approval and compared the demographic features and intraoperative details between the LS and HALS groups. Postoperative outcomes were further explored based on the two surgical techniques.
Surgical technique
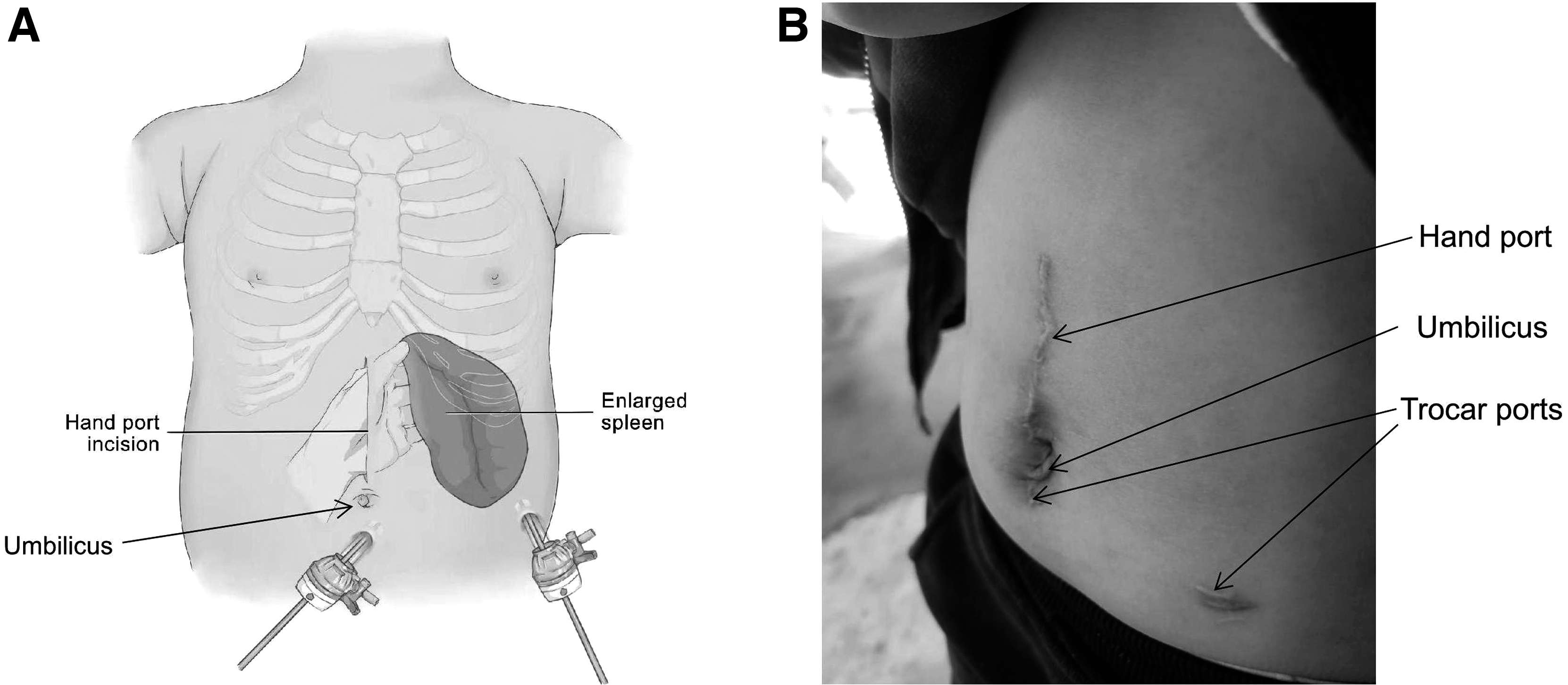
The patient was subjected to general anesthesia and slightly tilted in a reverse Trendelenburg position with 20°–30° elevated for the patient's left side with the camera holder and operator on the patient's right side. A nasogastric tube was routinely utilized for all the involved patients. The camera pole (usually 5-mm trocar) was placed in the lower umbilicus. The working port trocar was located according to the inferior splenic margin at the left midclavicular line. The supraumbilical hole near the splenic pedicle, which could be expanded upward to 6 cm in length incision, was used for the operating port in LS or for the hand port in HALS (Fig. 1). Pneumoperitoneum was maintained under a carbon dioxide pressure of 8–10 mm Hg (1 mm Hg = 0.133 kPa). For HALS, we exclusively performed this procedure in patients 7 years or older with sufficient space within the abdominal cavity. The operator should insert the left finger into the abdominal cavity to help complete the surgery through the hand port.
The surgeon's left hand could guide and help to temporarily occlude the splenic artery and vein near the splenic hilum using a laparoscopic bulldog clip. Afterward, the well-defined cyanotic demarcation line on the splenic surface should be clearly presented. Then, with the help of the surgeon's finger, an ultrasonic dissector was used to dissect splenic attachments and ligaments. The splenic parenchyma was incised using an ultrasonic scalpel according to the demarcation line. After these steps were completed, the temporarily occluded splenic artery was subjected to recanalization, and the blood supply was observed to be adequate for the remnant spleen. The resected specimen was extracted using a retrieval bag through the hand-assisted incision.
Statistical analysis
The data were assessed utilizing SPSS 17.0 for Windows (SPSS, Chicago, IL, USA). Continuous parameters were expressed as the median (range) or mean ± standard deviation as appropriate and were tested using Student's t-test or the Mann–Whitney U test, respectively. Categorical parameters are presented as numbers (percentages) and were analyzed utilizing the χ 2 test or Fisher's exact test. P < .05 was considered statistically significant.
Results
Patient demographics and surgical intervention features
During the study period between January 2012 and May 2021, a total of 62 patients who underwent LS or HALS were considered eligible. In total, 23 cases were excluded due to incomplete information, and 39 cases were included in the final analysis. Eleven cases were managed using the HALS technique (performed by the same surgeon), and 28 patients were managed using LS. The patients were between 6 and 11 years with an average of 8 years and 3 months. Patient demographic and clinical data are presented in Table 1.
General Information for the Involved Patients
HALS, hand-assisted laparoscopic splenectomy; IQR, interquartile range; LS, laparoscopic splenectomy.
The indications for splenectomy included splenomegaly of various origins in 21 (53.8%) patients and focal benign splenic lesions in 18 patients (46.2%), which are summarized in Table 2. The pathological outcomes for the focal benign splenic lesion were local splenic cyst (n = 7), lymphangioma (n = 6) and hemangioma (n = 5). There were eight lesions located in the lower pole of the spleen, five in the upper pole of the spleen and four in the splenic hilum.
Indications and Pathological Features for the Patients Undergone Splenectomy
Perioperative outcome
As shown in Table 3, patients who underwent HALS were found to have more favorable outcomes than those with LS. For HALS, the operative times (108 [78–215] versus 131 [93–263], P = .032) were significantly decreased compared with those managed with LS. Accordingly, less intraoperative blood loss was noted, and fewer blood transfusions were needed for the patients who underwent HALS. However, no significant differences were obtained. A lower conversion rate (0/11 versus 4/28) was noted for the patients who underwent HALS compared with those who underwent LS. No intraoperative conversion occurred from the HALS to the open operation. No significant differences in hospital stay or complications were noted between the two groups. There was no incidence of perioperative mortality, splenic infarctions, or any vein thrombosis in the involved pediatric patients.
Postoperative Outcome Between the Two Surgical Approaches
HALS, hand-assisted laparoscopic splenectomy; IQR, interquartile range; LS, laparoscopic splenectomy; SD, standard deviation.
The operative variables and clinical outcomes in terms of partial splenectomies were further compared between the two groups (Table 4). More favorable outcomes were noted for HALS compared with LS for partial splenectomies, including short operative time (P = .001) and less blood loss (P = .014).
Comparison for Partial Splenectomies Between the Two Surgical Approaches
HALS, hand-assisted laparoscopic splenectomy; IQR, interquartile range; LS, laparoscopic splenectomy.
Follow‑up data
Based on the general follow‑up strategy, all patients were evaluated utilizing upper abdominal computed tomography (CT) scan or ultrasound check at 1, 3, and 12 months postoperatively at the outpatient ward or clinic. Most of the patients reported improvements in quality of life with resolution of previous symptoms, and splenic regeneration was noted in most of the patients with partial splenectomy through the 12-month follow-up. There was no disease recurrence for the involved patients.
Discussion
For pediatric patients, partial splenectomy is preferred to preserve splenic function in selected cases. Furthermore, the minimally invasive surgical approach of HALS technique is more appropriate for these situations. In this study, we summarize our experience with a series of 39 pediatric patients managed utilizing HALS or LS. In this study, we provided convincing evidence supporting the benefit of HALS. While retaining the benefits of LS, such as improved cosmetic results and less postoperative discomfort, HALS can overcome the limitations of this approach through reduced blood loss, long operation time, and a high conversion rate to and open procedure.
As a bloodless technique modification, HALS has been adopted in many institutes as a minimally invasive operation using a left-handed approach into the abdominal cavity with the pneumoperitoneum present.8–10 The benefit of HALS predominantly involves hand-eye coordination and tactile feedback to improve the accuracy of manipulation, which could be useful for difficult laparoscopic procedures. 11 In the early stage, some partial splenectomy procedures were performed exclusively using the LS approach. The indications for these patients included nonparasitic cyst, lymphangioma, and angioma/hemangioma.
Splenic transection in partial splenectomy is time-consuming, and increased blood loss is noted for the laparoscopic approach. This finding was reasonable given the shorter operation time and lower blood loss for HALS compared with LS, as noted in this research. After all, during the operation, the hand can control and encircle the splenic vascular pedicle with his fingers at any time, which will provide a safeguard for the security of manipulation and dissection.9,10 With the assistance of the left hand, bagging the large resected spleens was also easy to accomplish, which should also reduce the operation time.
The abdominal volume of children is relatively small. In this study, a 5-cm long accessory incision was required for a successful operation for both the HALS and LS procedures. The difference was that the incision was made for spleen retrieval at the end of the operation in LS, whereas it was performed for a hand-assisted port at the beginning of the operation in HALS. HALS is generally considered only when patients are >6 years of age. In fact, this age is young. In addition, the spleen volume is relatively small, and the overall operation is more convenient. Of course, the age may be too young, and the incision is relatively large, which cannot reflect the advantages of minimally invasive surgery. According to the current results, HALS achieves the perfect combination of the advantages of LS and OS and avoids the disadvantages of LS and OS.
Bleeding is the focus of LS. Under the guidance of the intraperitoneal left hand, injury to the spleen or splenic vascular pedicle should be controlled easily in a faster and safer manner,12–14 thereby reducing the conversion rate. 15
In this research, all the involved HALS could be freely accomplished without conversion. Robotic-assisted partial splenectomy has also been proposed to reduce intraoperative hemorrhage.16,17 However, the expensive costs of robotic procedures have impeded its generalization. In addition, a reduced learning curve is needed for HALS, whereas the incision was the same or slightly longer than that of LS. Based on these advantages, HALS has been preferred by many experienced surgeons as a feasible and optimal approach to preserve the spleen.11,12,15 Another option to control hemorrhage in LS is intraoperative radiofrequency ablation and selective splenic embolization, which have been adopted by some researchers.18–20 However, this technique can only be accomplished in hemodynamically stable patients, which makes this approach less applicable. Furthermore, postembolization abdominal pain limits its utilization.
The reduced immune-competency and risk of overwhelming postsplenectomy infection (OPSI) and thrombocytosis are well-defined conditions, which are major concerns for asplenic patients.21,22 Whenever possible, a spleen-preserving procedure, namely, partial splenectomy, is preferred given the crucial role of the spleen. In particular, for pediatric patients with certain benign lesions, partial splenectomy is appropriate to preserve splenic immunological function. In addition, the residual splenic tissue was observed to grow again within 1 year after resection.
At least 25% of the remaining splenic parenchyma is required to reduce the incidence of thromboembolic events and maintain normal immune function. 23
LPS can be performed in several situations, including splenic cysts, splenic abscess, hemangioma, and lymphangioma, although less frequently.24,25 In some cases, we obtained the intraoperative pathological diagnosis of a benign lesion under the frozen sample, which allowed us to select the LPS. In 1994, Uranüs et al. reported the first partial splenectomy case series for localized nonhematologic splenic diseases. 26 Laparoscopic deroofing has been used for splenic cyst treatment, but the recurrence rate is very high at up to 33%. In this research, this type of recurrence was not noted because we have completely cut off the cysts.
Teperman advocated that splenic artery blocking for no more than 1 hour of warm ischemic time did not induce splenic infarction. 27 The HALS technique is a useful and feasible alternative for splenic artery block that is time-consuming when exclusively using the laparoscopic approach. In our cases, we isolated and controlled the trunk of the splenic artery and temporarily achieved blocking with Bulldog clips, which can be conveniently removed, under guidance from the left hand. The safety of selective splenic hilum ligation or temporary arterial occlusion has been proposed in several studies to reduce bleeding. 28 In this research, partial splenectomies could be safely performed with reduced blood loss and a shorter operative time, and these advantages favored the HALS operation. The 12-month follow-up data supported the safety of our procedure, as it indicated that no pseudoaneurysms and any embolic events were noted in the postoperative upper abdominal CT scan or ultrasound evaluation.
Some potential limitations should be kept in mind when interpreting the current data. First, the retrospective nature of this study with a relatively small population of heterogeneity groups might represent confounding factors regarding the preference of therapy or the surgeon's personal choice with an inherent risk of selection bias. In addition, investigators from a single center were not blinded to the purpose of this study. Second, although the follow-up time was as long as 38 months, OPSI events do not completely occur within this period. Owing to these limitations, the potential utility of our approach should not be arbitrarily interpreted as a conclusion and needs to be validated with an optimal sample size by other investigators.
In summary, HALS with occlusion of the splenic hilum is a feasible, effective, and safe procedure for splenic diseases. HALS can be applied as a useful bridge for an inexperienced surgeon to maximize the advantages of LS with better exposure of the splenic hilum while maintaining a tactile sense of OS. In addition, this technique maintains the benefit of minimal access features and potentially retains some splenic function, although an additional incision is needed.
Footnotes
Authors' Contributions
R.Z., and C.G. designed the study and analyzed the data. C.Y., and B.C. evaluated the article. C.G. performed the statistical measurements and analyzed the data. C.G. analyzed the data and wrote the article. All authors have read and approved the final article as submitted and agree to be accountable for all aspects of the study.
Acknowledgments
The authors thank Prof. Siqi Yang for providing technical assistance and for insightful discussions during the preparation of the article and Dr. Xiaoyong Zhang at the Wistar Institute for help with the linguistic revision of the article.
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or National Research Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Availability of Data and Material
The data set analyzed during this study is available from the corresponding author on reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the grants from the National Natural Science Foundation of China (Nos. 30973440 and 30770950) in the design of the study and collection, analysis, and interpretation of data, the Key Project of the Chongqing Natural Science Foundation (CSTC, 2008BA0021, cstc2012jjA0155) for collection, analysis, and interpretation of data and Chongqing Health Planning Commission of Research Fund (No. 2016MSXM044) in writing the article. The funding agency paid for the scholarship of students involved in the research.