
Abstract
Background:
Hydrocele of the canal of Nuck (HCN) is a rare cause of inguinal swelling in women. The optimal surgical procedure for HCN in children remains unclear. To assess the safety and efficacy of laparoscopic percutaneous extraperitoneal closure (LPEC) for HCN in a pediatric population, a retrospective study was conducted. In addition, to clarify the pathogenesis of HCN, we assessed the morphological findings of the internal inguinal ring (IIR).
Materials and Methods:
We retrospectively analyzed 10 consecutive female patients with HCN who underwent LPEC at our hospital between January 2010 and May 2020. Age, operative time, and complications were recorded. Concerning the findings of the IIR, we classified the morphological features as follows: Type 1 (flat), Type 2 (narrow patent processus vaginalis [PPV] with a peritoneal veil), and Type 3 (widely opening PPV).
Results:
The median age of patients who underwent LPEC was 3 (1–12) years. Although 2 patients showed contralateral inguinal hernia (IH), there were no cases of ipsilateral IH. All patients showed ipsilateral PPV, and the morphological features of the IIR were mostly classified as Type 3 (70%). In total, 6 of 8 HCN cases without preoperatively diagnosed contralateral IH had contralateral PPV (75%), and all were closed by LPEC. All operations were accomplished laparoscopically, and the postoperative course was uncomplicated, with no recurrences observed during the study period.
Conclusions:
LPEC is a safe and simple surgical approach to repair the HCN in children with minimal complications.
Introduction
The hydrocele of the canal of Nuck (HCN) is found in female patients, corresponding to cord or scrotal hydrocele in male patients. Hydrocele is a common entity in male patients, whereas HCN is relatively rare even in children. HCN accounts for <1% of inguinal swelling in female patients, and the cause of the discrepancy between the two genders is unknown.1,2
Although hydrocelectomy is recommended for HCN treatment in adults, the optimal management of HCN in children is still undetermined due to the limited number of reported cases.3–5 To date, the safety and efficacy of laparoscopic surgery associated with high ligation of the processus vaginalis have been widely acknowledged in the treatment of hydroceles in male patients.6,7 The pathogenesis of HCN may also be patent processus vaginalis (PPV) (canal of Nuck). Moreover, in a previous study, we adopted laparoscopic high ligation without hydrocelectomy for hydroceles in male patients and confirmed the safety and efficacy of this approach. 6
This study aimed to clarify the safety and efficacy of laparoscopic percutaneous extraperitoneal closure (LPEC) for HCN in a pediatric population. We further evaluated the morphological findings of the internal inguinal ring (IIR) in HCN cases to explore the pathogenesis of HCN.
Materials and Methods
We retrospectively reviewed 10 consecutive female patients (age <15 years) who underwent LPEC for HCN at the department of pediatric surgery, Osaka University, Osaka, Japan, between January 2010 and May 2020. Age, weight, symptoms, pre-/postoperative diagnosis, length of operation/pneumoperitoneum, and intra-/postoperative complications were recorded.
Complications were defined according to the Clavien–Dindo classification system, 8 and complications of grade 3b or above were recorded. In addition, the authors retrospectively evaluated the morphological features of the IIR (either the affected or contralateral side) on operative videos in every case. The findings of the IIR were classified into three groups, which included Type 1 (flat), Type 2 (narrow PPV with a peritoneal veil), and Type 3 (widely opening PPV), according to previous reports by Chin et al. and our group.6,9
The diagnosis of HCN was confirmed by pediatric surgeons based on clinical manifestations, physical examination, and ultrasound findings. The indications for surgery included age >12 months and concomitant inguinal hernia (IH) regardless of age. Inclusion criteria for this study were children with Nuck hydrocele diagnosed by physical examination and preoperative ultrasound and confirmed by intraoperative findings. Exclusion criteria included patients with intraoperative findings identified as other diseases and nonoperated patients.
LPEC is characterized by an extraperitoneal high ligation of PPV with a straight hollow needle (Lapa-Her-Closure™; Hakko Medical Co., Tokyo, Japan; Fig. 1), which has a built-in wire loop within the lumen that allows the suture thread to be held and released. The details of the procedure have been described in our previous report. 6 In brief, a 3.5-mm trocar for laparoscopy was placed through an umbilical incision. The pneumoperitoneum was established with CO2 insufflation, and the patient was placed in the Trendelenburg position. A 2-mm trocar was placed in the right lower abdomen. A Lapa-Her-Closure with a 2-0 nonabsorbable suture thread was inserted at the level of the IIR.

Schemes of the special needle for laparoscopic percutaneous endoperitoneal closure (Lapa-Her-Closure™; Hakko Medical Co., Tokyo, Japan). A straight hollow needle incorporates a built-in wire loop within the lumen that allowed the suture thread to be held and released.
A half-circuit suture was placed extraperitoneally on the lateral side. Once the needle completely passed behind the round ligament, the operator allowed the tip of the needle to penetrate the peritoneum and release the suture material into the abdominal cavity. The medial half circumference was also advanced extraperitoneally, and the suture material was withdrawn with Lapa-Her-Closure. Finally, the circuit suture was tied extracorporeally. Before ligation, the ipsilateral inguinal region was compressed extracorporeally to reduce the fluid content within the processus vaginalis (canal of Nuck).
When the encysted HCN was confirmed laparoscopically, the wall was opened using electrocautery for intracorporeal drainage. Percutaneous aspiration of the hydrocele was performed only if the hydrocele remained significant at the end of the operation. The contralateral PPV was simultaneously closed, regardless of its size. Postoperative follow-up was conducted for 1 year after surgery, involving mainly physical examinations with additional ultrasound as needed.
All statistical analyses were performed using GraphPad Prism (version 9.00; GraphPad Software, San Diego, CA, USA). Continuous variables were expressed as medians and interquartile ranges (IQRs). Statistical significance was calculated using the Mann–Whitney U test. Statistical significance was set at P < .05.
This study was approved by the institutional review board of our hospital (IRB 20567).
Results
During the study period, 15 patients with HCN underwent definitive surgery at our institute. Two patients who underwent repair using the open inguinal approach (open repair [OR]) and 3 patients who had a prior ipsilateral inguinal operation were excluded from this study; therefore, the remaining 10 cases were analyzed. Patient demographics are given in Table 1. Although all patients complained of inguinal swelling, only 1 patient experienced significant pain. There was no significant laterality in the HCN. Although contralateral IH was confirmed preoperatively in 2 (20%) patients, no associated IH was observed on the side of hydrocele in this series.
Patient Demographics
Data are median (IQR) values.
IQR, interquartile ranges.
Surgical outcomes are summarized in Table 2. Contralateral PPV was confirmed in 6 out of 8 preoperatively unilateral HCN cases (75%), resulting in only 2 HCN cases who underwent unilateral repair. The median length of operation and pneumoperitoneum were 39 and 26 minutes for unilateral cases, and 54.5 and 33.5 minutes for bilateral cases, respectively. Simultaneous repair of umbilical hernia was performed in 3 patients. There were no intraoperative complications, and no conversion from LPEC to OR was observed. The median follow-up period was 42 months (IQR: 19.5–60.5). All participants completed our postoperative follow-up, and no major postoperative complications, including recurrence, were observed.
Surgical Outcome of Hydrocele of the Canal of Nuck
Data are median (IQR) values.
Cases with a simultaneous surgery are excluded from analyses.
IH, inguinal hernia; IQR, interquartile ranges; PPV, patent processus vaginalis.
Laparoscopic morphological findings of IIR of HCN are given in Table 3. The IIR features of the affected side were classified as Type 3 (70%) and Type 2 (30%). All HCNs showed PPV. Two showed the absence of fluid drainage to the abdominal cavity during surgery and required percutaneous drainage, suggesting the existence of a distal cyst or check valve within the canal of Nuck. Both IIR types were classified as Type 3.
Morphological Findings of the Internal Inguinal Ring in Hydrocele of the Canal of Nuck
HCN, hydrocele of the canal of Nuck; IIR, internal inguinal ring.
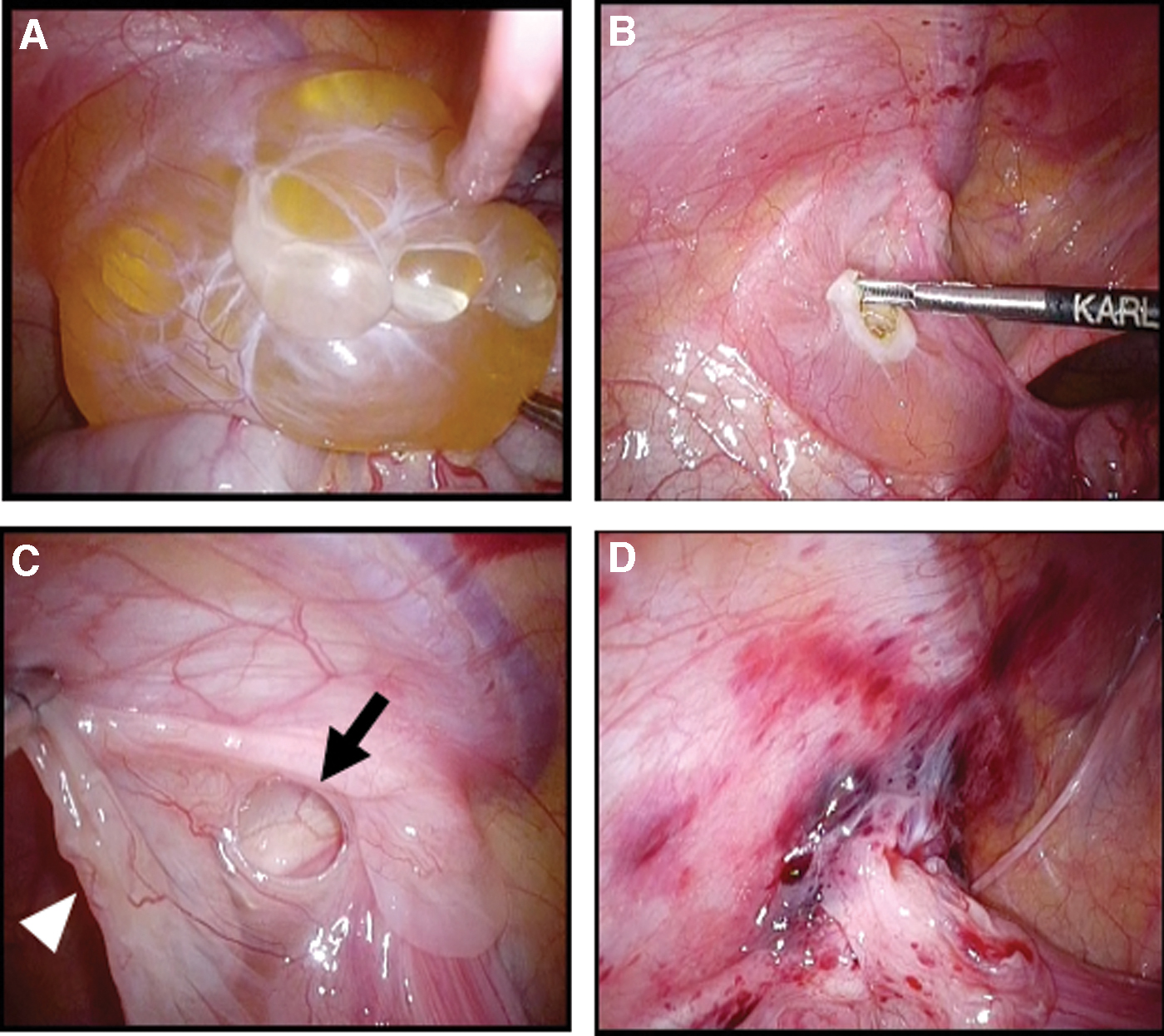
One patient had an extensive hydrocele mimicking an abdominoscrotal hydrocele (ASH) in a male patient (Fig. 2). In this case, after laparoscopic drainage of the hydrocele with electrocautery, the IIR (Type 2) was closed with LPEC. In patients with HCN, contralateral IIR manifested Type 3 in 5 patients (50%, including 2 contralateral IHs), Type 2 in 3 patients (30%), and Type 1 in 2 patients (20%).
Discussion
The safety and efficacy of laparoscopic surgery for IH and hydrocele in male patients have been well acknowledged in children.6,7,10 However, there is a paucity of information available on laparoscopic treatment of HCN. 11 This study reported consecutive 10 pediatric patients with HCN treated with LPEC.
The typical presentation of HCN is a painless, translucent, and irreducible inguinal mass.5,12 In our series, all but 1 patient complained of painless inguinal swelling, in agreement with previous findings. Although one-third of adult HCN cases have been reported to be associated with concomitant ipsilateral IH,13–15 there was no IH on the affected side in our pediatric series.
Hydrocelectomy through inguinal incision or laparoscopy is the standard procedure for HCN in adults. 5 To date, there has been only one study on laparoscopic surgery for pediatric cases of HCN. 11 We employed LPEC for HCN based on our experience with LPEC without hydrocelectomy for hydrocele in boys. 6 We believe that high ligation with or without fluid drainage could be a definitive treatment for pediatric cases of HCN. Although difficulties were sometimes experienced in complete drainage of the fluid contents either intraperitoneally or extracorporeally, the residual contents usually diminished within months postoperatively.
Although hydrocelectomy is recommended in adult cases due to the possibility of ectopic endometriosis within the canal of Nuck, dissemination of endometrial cells into the HCN and resultant ectopic endometriosis occur after puberty. A literature review on endometriosis within the canal of Nuck showed that the youngest occurrence was at 20 years of age, with a median age of 36 years. 16 Furthermore, the prevalence of endometriosis within the canal of Nuck is extremely rare, with only 36 cases reported to date. Therefore, cyst excision is thought to be unnecessary, especially in prepubertal patients. Considering the risk that asymptomatic PPV would be complicated with ectopic endometriosis in the future, contralateral PPV should be treated regardless of the symptoms.
Counselor and Black 17 classified HCN into three categories: the encysted type, which is the most common and does not communicate with the peritoneal cavity, the communicating type, which has persistent communication between the hydrocele and the peritoneal cavity, and the hour-glass type, which has a constriction at the IIR so that the upper sac is located in the abdominal cavity, whereas the lower sac is in the inguinal canal. 17 However, laparoscopic observation of HCNs has never been reported. All of our HCN cases showed opening of the IIR, namely, communicating HCN.
Laparoscopic examination is useful for investigating the patency of the processus vaginalis with direct visualization of the IIR. Our laparoscopic examination identified a constriction of the processus vaginalis proximal to the HCN in 4 cases. Among the remaining 6 cases, 3 cases were identified with a drainage of accumulating fluid toward the abdominal cavity, 2 cases had a nondrainable cyst, and 1 case featured HCN mimicking ASH in male patients. Such “undrainable” cases may be clinically diagnosed as “noncommunicating hydrocele.”
Interestingly, our study showed that all of our pediatric HCN cases presented PPV, where Type 3 (wide opening PPV) was the most common category, followed by Type 2 (narrow PPV with peritoneal veil). Our HCN finding resembles the previously reported features of IH in male patients, which almost all patients displayed Type 3 features, rather than hydrocele in male patients in which Type 2 (narrow PPV with a peritoneal veil) was the most common characteristic. 6 These results may be helpful in understanding the pathogenesis of HCN.
The limitations of this study include the small patient population arising from the rarity of HCN. The laparoscopic examination performed in this study had potential limitations owing to the restricted view of the scope from the abdominal cavity. Further investigations on the correlation between laparoscopic examination and the conventional classification of HCN in a larger cohort with long-term results are necessary.
Conclusions
LPEC is a safe procedure for treating pediatric cases of HCN. Complete excision or opening of the hydrocele may be unnecessary, at least in prepubertal female patients. The morphological findings of the IIR in cases of HCN showed a wide opening PPV in most cases.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: study conception and design were by K.D., R.S., and H.O.; data collection was carried out by K.D.; analysis and interpretation of results were done by K.D., R.S., M.N., K.M., M.W., M.K., T.U., and Y.T.; and draft article preparation was carried out by K.D., R.S., and H.O. All authors reviewed the results and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.