
Abstract
Introduction:
Aberrant left hepatic artery (ALHA) can exist in up to 25% of the population. The presence of ALHA during lymph node (LN) dissection in gastric cancer may complicate the process. In this study, we aimed to evaluate the existence rate, management, and consequences of ALHA in our laparoscopic gastrectomy series.
Patients and Methods:
Demographical and clinical data of laparoscopically operated 158 consecutive gastric cancer patients were collected retrospectively. Study patients were divided into three groups according to absence, existence and preservation, and existence and sacrification of ALHA. Harvested LN numbers, operation time, and postoperative alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lactate dehydrogenase values on consecutive days were analyzed using Kruskal–Wallis and Mann–Whitney U tests. P < .05 is accepted as significant.
Results:
The median AST and ALT values of the ALHA-sacrificed group were higher than those of the group without ALHA and the ALHA-preserved group on the 1st, 3rd, and 5th postoperative days (P < .05). On the 10th day, liver enzymes returned to normal values.
Conclusion:
Adequate and appropriate dissection of LNs while preserving ALHA can be performed without prolonging the operation time. Sacrification of ALHA causes an increase in liver enzymes, with spontaneous recovery in most cases.
Introduction
Gastric cancer is one of the leading causes of cancer-related deaths. Nevertheless, the most effective treatment is surgery. Definitive surgery for gastric cancer requires adequate lymph node (LN) dissection in addition to negative surgical margins. 1 The extent of surgical intervention together with the stage of the disease is also related to survival for gastric cancer.
Aberrant left hepatic artery (ALHA) is described in ∼25% of the population in the literature, and it is stated that approximately half of it is an accessory left hepatic artery (acLHA) originating from the left gastric artery, whereas the other half is a replaced left hepatic artery (RLHA). 2 Preservation of aberrant hepatic arteries encountered during LN dissection may complicate the procedure. Ligation or preservation of these arteries is important in terms of liver functions and oncological surgical principles. Complete LN dissection around the left gastric artery is essential in gastric cancer surgery and usually requires root ligation of the left gastric artery.
In this study, we aimed to reveal the ALHA rate, treatment approach, and functional results in patients who underwent laparoscopic surgery for gastric cancer in our clinic in the past 5 years.
Materials and Methods
Patient selection
Between December 2015 and December 2020, 402 patients who were operated on for gastric surgery were evaluated in the study. Patients who underwent open gastric surgery and received neoadjuvant chemoradiotherapy were excluded from the analysis (n = 244).
This is a retrospective analysis of institutional board-reviewed data of 158 consecutive patients undergoing laparoscopic surgery for stage 1–3 gastric cancer who did not receive neoadjuvant chemoradiotherapy.
Data collection
Surgery reports, radiological imaging, and laparoscopic video records were reviewed. The presence of ALHA and how it was managed were recorded from the surgery reports and video records. The presence of ALHA was recorded by re-examining the radiological images and video records. The number of dissected LNs and the number of metastatic LNs were recorded by examining the pathology reports. Pathological staging was based on recommendations from AJCC 2018 (edition VIII) for TNM classification.
Pre- and postoperative alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) parameters on the 1st, 3rd, 5th, 7th, and 10th days were recorded. The postoperative enzyme elevations of the patient, as well as the changing metabolic status and developing hepatic complications, were recorded. Intra- and postoperative first 72 hours blood transfusions are accepted as perioperative blood transfusions.
Operation strategy
Patients' CT views and reports were analyzed before operation. The operation strategy was the same for all patients as described in previous studies of our clinic. 3 Nathanson retractor was used for left lobe retraction of the liver in all patients. After ligation of the right gastroepiploic vessels and right gastric artery, the pilor was transected with an endoscopic linear tristapler. LN dissection continued. Lesser sac was explored for ALHA. In the case of the existence or suspicion of ALHA, dissection of the LGA is extended up to the stomach to find the branching of the ALHA (Fig. 1).
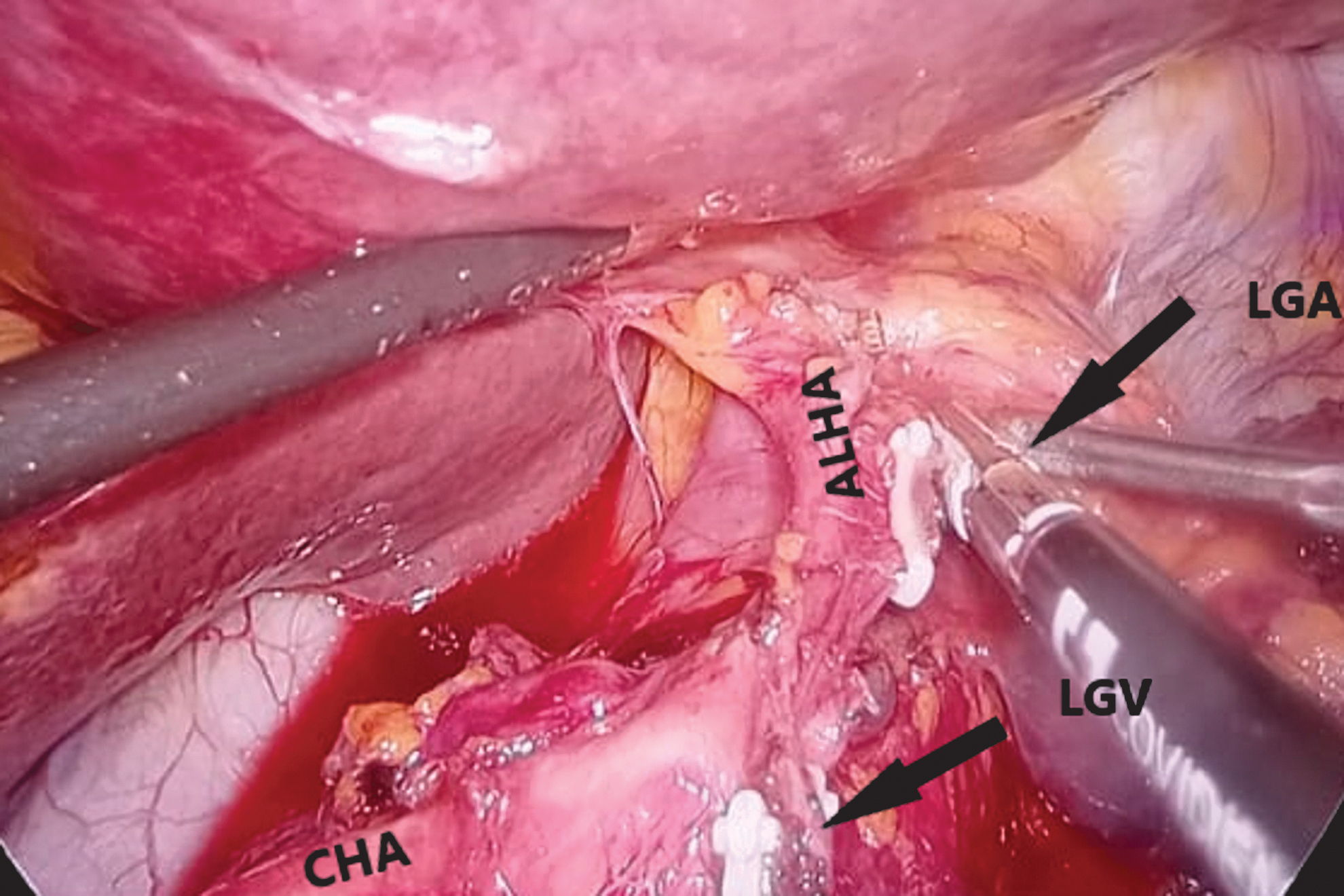
Laparoscopic view of ALHA preserved and LGA ligated after division of ALHA in a 62-year female patient. ALHA, aberrant left hepatic artery; CHA, common hepatic artery; LGA, left gastric artery; LGV, left gastric vein. Color images are available online.
Statistical analysis
Study groups consisted of a patient group without ALHA, a patient group in which ALHA was found and sacrificed, and a patient group in which ALHA was present and preserved. Mean, median, standard deviation, and quartile deviation values were calculated for each variable of the patient groups. In the analysis of differences between groups, nonparametric tests were used due to the low sample size, unbalanced between-groups, and the inability to provide parametric test assumptions. 4 The Kruskal–Wallis H test was used to compare the measurements of the patient groups.
To determine which groups the difference was between, the Mann–Whitney U test was used, which is a post hoc pairwise comparison test. When a difference between groups was detected in a measurement, the impact assessment suggested by Cohen was applied to determine the magnitude of this difference. 5 Accordingly, r = 0.10 reflects a low, r = 0.30 medium, and r = 0.50 large effect. Statistical analyses were performed in the SPSS.26 program and the P < .05 significance level was taken into consideration.
Results
The study was carried out on 158 patients. The age range of the patients ranged from 22 to 86, with a median age of 62. Sixty-two percent of the patients were male (n = 98), and 38% were female (n = 60). Laparoscopic total gastrectomy was performed in 29.1% of the patients (n = 46), and laparoscopic subtotal gastrectomy was performed in 70.9% of the patients. ALHA was present in 17.1% (n = 27) of the patients. Of these patients, 7.6% (n = 12) were in the preserved group and 9.5% (n = 15) were in the ligated group.
When the data obtained from the reports were evaluated, it was determined that ALHA was sacrificed for the appropriate dissection of conglomerated LNs in 6 patients, and for bleeding control from the LGA root in 7 patients, and ALHA was noticed after sacrification in 2 patients. In 7 patients, operations were converted to laparotomy due to bulky tumors and adhesions (in 5 of ALHA absent group, in 1 of ALHA preserved group, and in 1 of ALHA-sacrificed group; P = .307). Table 1 demonstrates demographical and clinical parameters of study patients. Age, gender, localization of tumors, harvested LNs, operation times, perioperative blood transfusion, and BMI did not differ significantly between groups.
Demographic and Clinical Variables of Study Patients
Data are presented as median (IQR).
ALHA, aberrant left hepatic artery; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; IQR, interquartile range; LDH, lactate dehydrogenase; LN, lymph node.
The median ALT values of the ALHA-sacrificed group were higher than those of the group without ALHA and the ALHA-preserved group on the 1st, 3rd, and 5th postoperative days and statistically significant (χ 2 = 35.757, P < .05; χ 2 = 27.698, P < .05; χ 2 = 18.892, P < .05, respectively). On the 10th day, the difference was not found to be statistically significant (χ 2 = 3.989, P > .05) (Fig. 2). Between which groups the difference was significant was examined with the Mann–Whitney U paired comparison test.
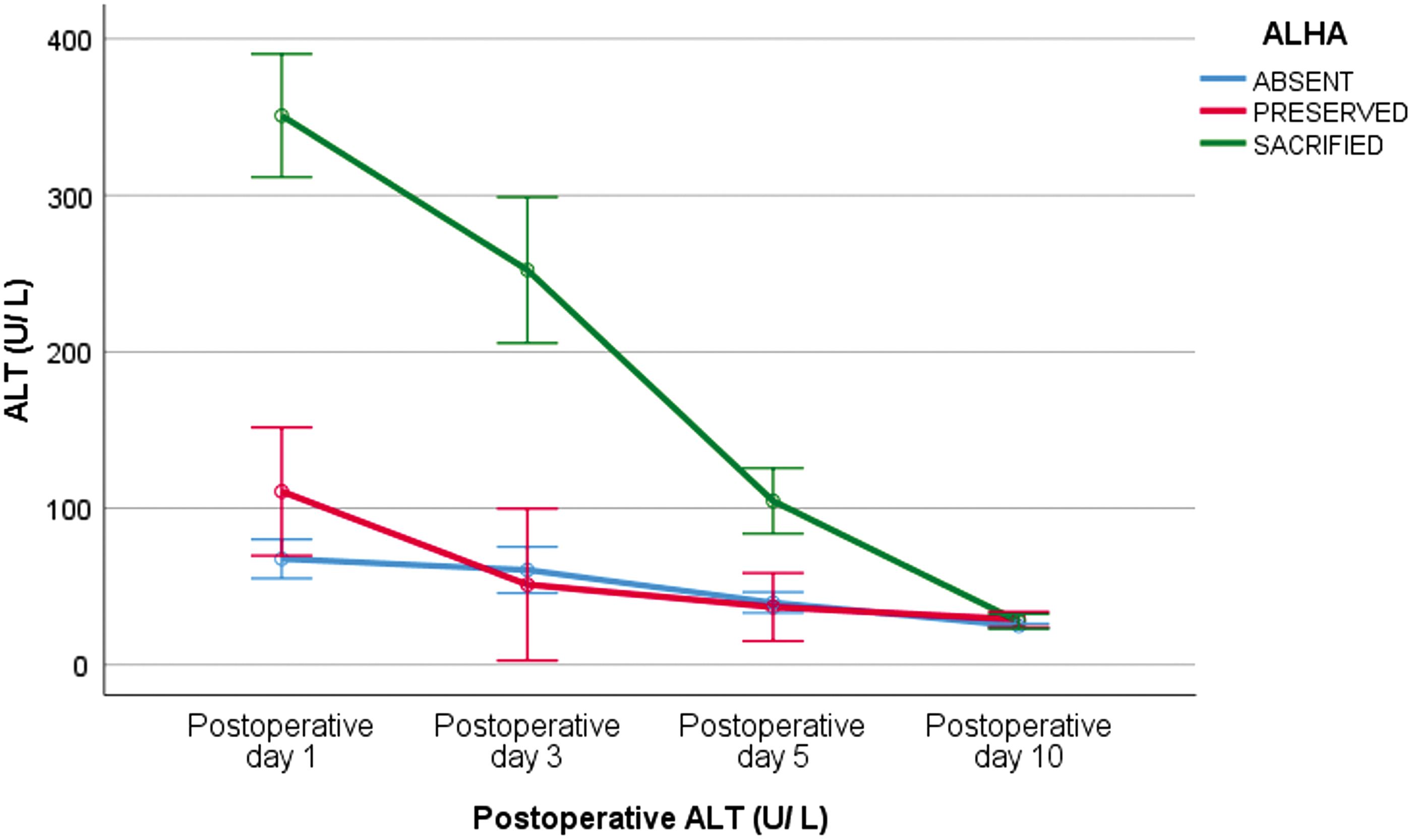
Changes in ALT values in postoperative consecutive days. ALT, alanine aminotransferase. Color images are available online.
Accordingly, postoperative ALT measurements were statistically higher in the group in which ALHA was sacrificed on the 1st, 3rd, and 5th days than in the group in which ALHA was detected and preserved (U1.day = 5.000, P < .000, r = 0.79; U3.day = 3.000, P < .000, r = 0.81; U5.day = 13.500, P < .000, r = 0.7), and ALHA was not present (U1.day = 24.500, P < .000, r = 0.48; U3.day = 111.500, P < .000, r = 0.43; U5.day = 249.500, P < .000, r = 0.35). The effect of the difference between the mean rank of the group in which ALHA was sacrificed and the group in which ALHA was detected and preserved was large (r > 0.5). The effect of the difference between the mean rank of the group in which ALHA was sacrificed and the group without ALHA was medium (r > 0.3).
The median AST values of the ALHA-sacrificed group were higher than those of the group without ALHA and the ALHA-preserved group on the 1st, 3rd, and 5th postoperative days and statistically significant (χ 2 = 30.441, P < .05; χ 2 = 22.441, P < .05; χ 2 = 9.654, P < .05). On the 10th day, the difference was not statistically significant (χ 2 = 0.042, P > .05) (Fig. 3). Between which groups the difference was significant was examined with the Mann–Whitney U paired comparison test.
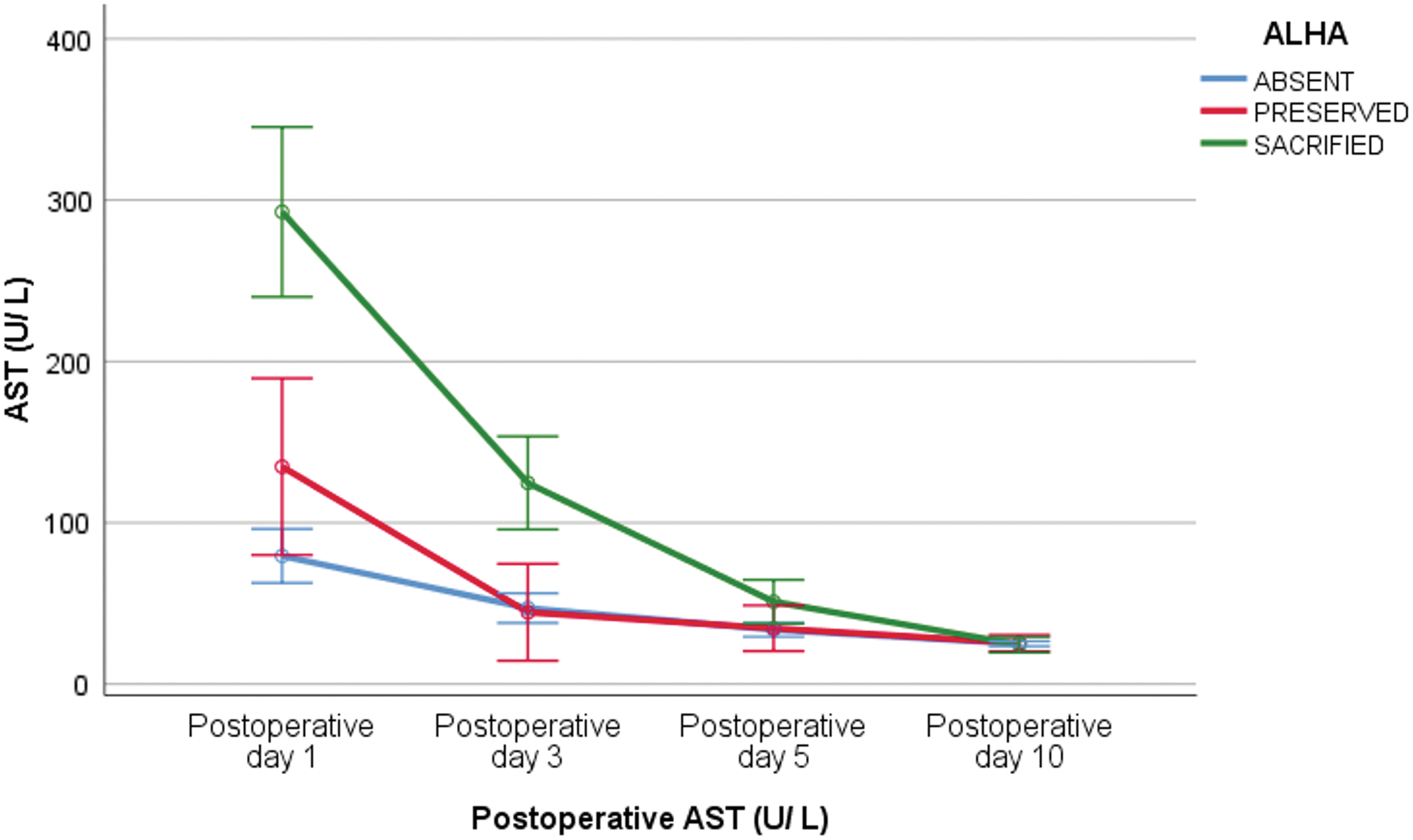
Changes in AST values in postoperative consecutive days. AST, aspartate aminotransferase. Color images are available online.
Accordingly, postoperative AST measurements were significantly higher in the group in which ALHA was sacrificed on the 1st, 3rd, and 5th days than in the group in which ALHA was detected and preserved (U1.day = 23.000, P = .003, r = 0.59; U3.day = 14.000, P < .000, r = 0.7; U5.day = 13.500, P < .000, r = 0.7), and ALHA was not present (U1.day = 93.500, P < .000, r = 0.44; U3.day = 189.000, P < .000, r = 0.38; U5.day = 249.500, P < .000, r = 0.35).
The effect of the difference between the mean rank of the group in which ALHA was sacrificed and the group in which ALHA was detected and preserved was large (r > 0.5); it is seen that the effect of the difference between the mean rank of the group in which ALHA was sacrificed and the group without ALHA was medium (r > 0.3).
When the LDH results were examined, the mean rank of the LDH measurements of the group in which ALHA was sacrificed on the 1st day, was higher than the mean rank of the LDH measurements of the groups without ALHA and in which ALHA was detected and preserved. In the measurements taken on other days, the LDH rank average of the group in which ALHA was detected and preserved was higher than that of the other groups.
These differences between the mean rank of postoperative LDH measurements were statistically significant between the groups on the 1st and 3rd days (χ 2 = 19.347, P < .05; χ 2 = 6.538, P < .05); on the 5th and 10th days, they were not found to be statistically significant (χ 2 = 5.753, P > .05; χ 2 = 3.895, P > .05) (Fig. 4). Between which groups the difference was significant was examined with the Mann–Whitney U paired comparison test.
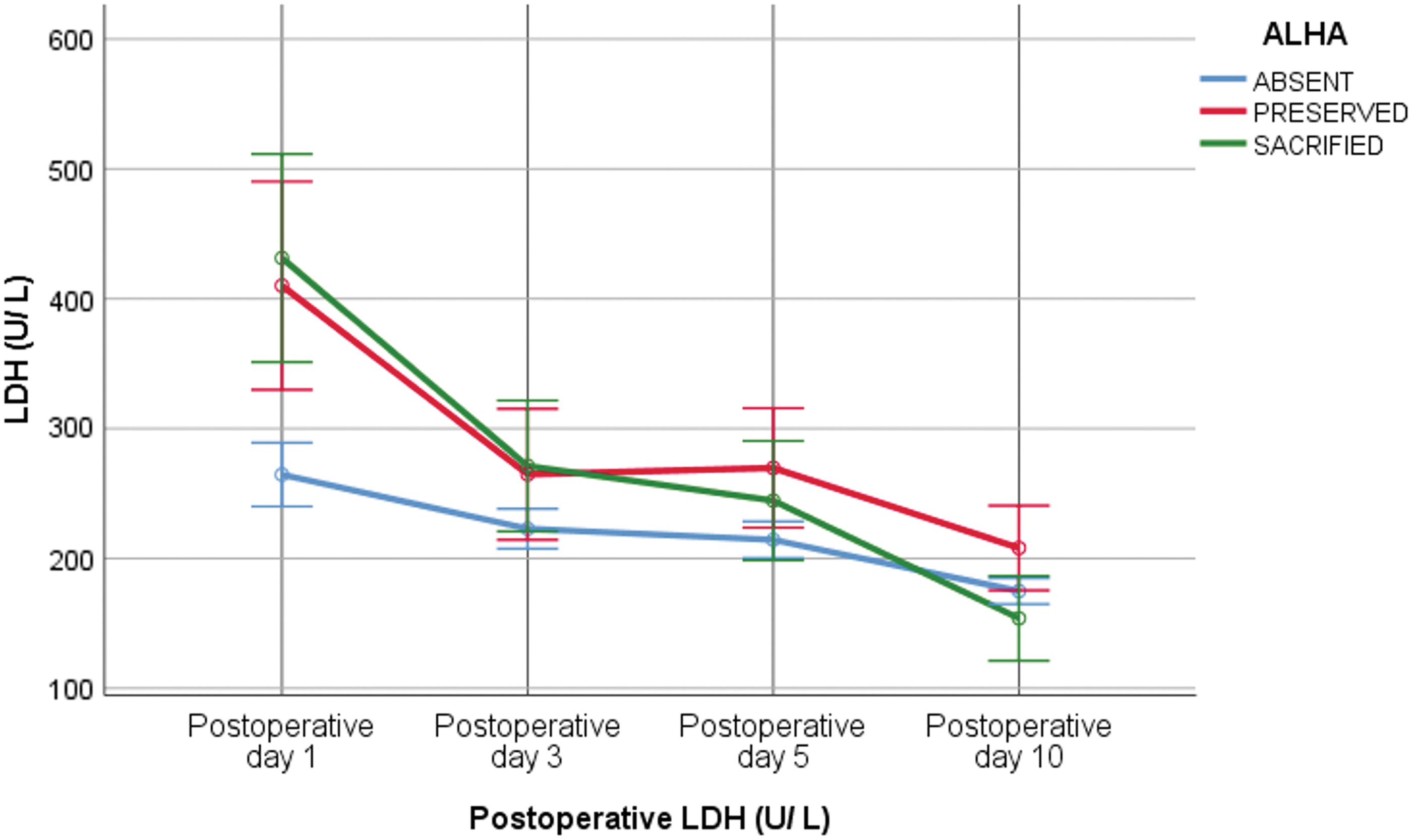
Changes in LDH values in postoperative consecutive days. LDH, lactate dehydrogenase. Color images are available online.
Accordingly, postoperative LDH measurements were significantly higher in the groups in which ALHA was detected and preserved on the 1st and 3rd days compared with the group without ALHA, (U1.day = 374.000, P = .003, r = 0.25; U3.day = 469.000, P = .026, r = 0.19), and the effect of the difference was low, r < 0.30 (Cohen 1992). Another difference was the LDH value measured on day 1 between the groups in which ALHA was sacrificed and the group without ALHA. Accordingly, the LDH value measured on the 1st day of the group in which ALHA was sacrificed was significantly higher than that of the group without ALHA, (U = 297,000, P < .000, r = 0.30). The effect of this difference is moderate. 5
Discussion
It has been reported that laparoscopic total/subtotal gastrectomy and LN dissection can be safely performed in early-stage gastric cancer. 6 The laparoscopic approach for the surgical treatment of gastric cancer is increasing and developing worldwide. This development is because laparoscopic treatment centers gain experience and become widespread, and the reliability of laparoscopic treatment has been demonstrated in the literature. 7 Anatomical vascular variations are common in the upper gastrointestinal tract.
There is no consensus on whether it is safe to ligate ALHA originating from the left gastric artery during laparoscopic gastric cancer surgery; however, it has been reported in the literature that there is no significant difference in the number of LNs dissected in cases where ALHA is preserved and ligated.8,9 Therefore, there are studies reporting that there is no significant difference in terms of oncological results in patients in whom ALHA is preserved, transient liver dysfunction develops as a result of ligation of ALHA, and ligation is completely safe, and there are also studies reporting serious complications such as an abscess, cholangitis, liver failure, and ischemia.10,11
Previous studies have shown that ALHA ligation results in transient elevation of ALT and AST, and spontaneously returns to normal within ∼2 weeks after surgery. 2 Hepatic necrosis has not been reported when ALHA was sacrificed, even in patients with liver disease, and this has been explained by the development of collateral arterial flow from the intrahepatic and phrenic arteries after ligation.12–14 It has been reported that preservation of ALHA does not reduce oncological safety, laparoscopic feasibility, or the scope of lymphadenectomy.15,16
In the analysis of patients undergoing laparoscopic surgery for gastric cancer in this study, no significant difference was found in terms of age, gender, BMI, tumor location, operation time, and the number of LN dissected. The ALHA rate was found to be 17.1%, which is consistent with the current literature. 9 In the group in which ALHA was sacrificed, we observed that the ALT and AST values of the patients started to increase from the 1st postoperative day, although they were not at the same level in all patients, and generally tended to improve within the 1st week and returned to normal on the 10th day.
Although ALT and AST values were moderately high in the early postoperative period in the group in which ALHA was preserved and in the group in which ALHA was not detected, it was not statistically significant. We think that this moderate increase may be due to the Nathanson retractor used for left lobe retraction of the liver. In previous studies, it has been reported that transient liver dysfunction develops in cases where retractors are used. 17
Since the Nathanson retractor was used in all of our patients and they were all affected in a similar way, the liver enzyme elevations found to be very high in the group in which ALHA was sacrificed cannot be explained by the retractor effect. In this study, all patients had normal preoperative ALT and AST values, and it was observed that patients who underwent ALHA ligation reached normal liver functions on the 10th day.
In previous studies, when ALHA was sacrificed, LDH was found to be elevated and it was observed that LDH returned to normal values in ∼10 days. 8 In our study, in the presence of ALHA, it was observed that LDH increased significantly on the 1st postoperative day in the groups in which ALHA was both preserved and sacrificed. It was observed that the high course of LDH continued in the group in which ALHA was preserved on the 3rd postoperative day. It was observed that it returned to physiological value on the 10th postoperative day. It is thought that LDH elevation may be related to manipulations and stresses during the preservation of ALHA.
In this study, it was observed that there was no statistically significant difference between the groups in terms of perioperative blood transfusion, operative times, or overall survival. There was no significant difference between the groups in the follow-up of liver enzymes on the 10th day.
As it is difficult to distinguish between intraoperative ALHA and RLHA or acLHA, preoperative angiographic evaluation can be informative and contribute to the preservation of RLHA. 14 The limitations of this study were that it was single-center, the total number of patients was small, and the ALHA groups included a small number of patients.
Since the preoperative routine angiographic evaluation was not performed in our study, and the presence of ALHA in our patients was mostly observed intraoperatively, the distinction between the RLHA and the accessory left hepatic artery (acLHA) could not be made clearly. In patients who developed very high enzyme elevations in their postoperative follow-up, there is a possibility that the ALHA that was ligated was RLHA, but even so, it was observed that they returned to normal liver functions in the follow-ups.
Conclusion
In conclusion, the existence of ALHA is not rare, and adequate and appropriate dissection of LNs by preservation of ALHA can be performed without increasing the operation time. Although sacrification of ALHA increases liver enzymes, resolution occurs spontaneously in 10 days. In addition to gastric cancer surgery, the possibility of ALHA should be kept in mind in all surgical processes involving the lesser curvature and adjacent region. To the best of our knowledge regarding literature, ligation of ALHA causes limited damage, and resolves in ∼2 weeks. An overlooked presence of ALHA may cause bleeding or unexplained hepatic enzyme elevation in the early postoperative period.
Ethical Declaration
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the study to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the Journal of Laparoendoscopic & Advanced Surgical Techniques.
Acknowledgment
All authors thank Gözde Sırgancı for her statistical studies.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.