
Abstract
Background:
The benefits of a valid pneumoperitoneum in laparoscopic surgery are counterbalanced by the possible negative effects of increased abdominal pressure and carbon dioxide (CO2) insufflation, which are crucial factors in causing postoperative pain. The purpose of this work is to evaluate the effectiveness of the valveless trocar (VT) insufflation system in decreasing postoperative pain and influencing operative time, compared to a standard insufflation system.
Methods:
A systematic research was performed using MEDLINE, EMBASE, Central Cochrane Library, and CINAHL Plus for studies published up to June 2020. Randomized controlled trials (RCTs) on adult population evaluating the effects of VT versus a standard insufflation system in laparoscopic surgery and reporting postoperative pain level and operative time were included in the analysis. Data and study quality indicators were extracted independently by 2 authors using a standardized form. Statistical analysis was based on a random effect model, using the inverse variance method.
Results:
We identified 3 RCTs for a total of 245 patients. The meta-analysis showed a statistically significant reduction in shoulder pain with the use of VT at 24 hours: mean difference (MD) −7.9% (95% confidence interval [95% CI]: −1.29 to 0.29; z = 3.08; P = .002) and a nonstatistically significant increase in operation time: MD 5.80 (95% CI: −8.93 to 20.54; P = .44).
Conclusion:
Our study suggests a better shoulder pain control at 24 hours postoperation using new-generation VT for laparoscopic surgery compared to standard insufflation system. Weak evidence of increased operating time with the VT was observed considering only two of the three RCTs.
PROSPERO registration number: CRD42020191835
Introduction
The use of minimally invasive surgery, compared with open surgery, allows to minimize surgical trauma and blood loss, 1 resulting in a rapid postoperative recovery of the patient,2,3 reduction of postoperative pain, 4 and a decrease in complications, such as wound infections and hypertrophic surgical scar.3,5
The success achieved by the laparoscopic and robotic assisted technique in the treatment of benign diseases and in the field of neoplastic pathology is closely linked to a clearer visualization of the surgical field, even in the most difficult anatomical spaces. This condition is obtained by creating an optimal pneumoperitoneum, through the insufflation of CO2 and the development of intraperitoneal pressures. Physiologically, however, the generation of the pneumoperitoneum is counterbalanced by hemodynamic and respiratory alterations due to high endo-abdominal pressures and prolonged absorption of CO2, which can lead to metabolic, cerebrovascular, and hemodynamic alterations,6–8 also exposing the patient to the risk of emphysema, embolism, and hypercapnia. 9
The new valveless trocar (VT) insufflation system has been proposed as an effective tool in minimizing CO2 insufflation effects during pneumoperitoneum, improving operative time 10 and intraoperative respiratory mechanics. 11
The VT insufflation system deflects the CO2 that comes out of the proximal end of the device, filters the gas, and recirculates it in the peritoneal cavity. By directing the gas at high speed toward the distal opening of the cannula, a stable pressure is created and maintained inside the abdominal cavity. Furthermore, the VT system activates a constant flow, which simultaneously evacuates the intra-abdominal gas (composed of CO2 and fumes), filters it, and puts it back without the need for cyclic detection and inflation, typical of conventional trocars. All of this results in an easier access to the abdominal cavity without valves, a more stable pneumoperitoneum, and a constant evacuation of fumes.
Although some studies have reported satisfactory results on the quality of surgical visualization, 12 patient's ventilator mechanics, CO2 consumption,11,13 and postoperative pain, 14 the real impact of VT on laparoscopic surgery is still under debate. Herrmann et al. reported a different composition of CO2 pneumoperitoneum generated with VT compared to standard trocar in an experimental and clinical setting, thus emphasizing the importance of conducting further studies on the influence of VT physiological effects on clinical outcomes. 15 Moreover, despite the positive evidence registered in some studies, Hillelsohn et al. warned that the use of the VT system may mask the physiological changes induced by pneumothorax during laparoscopic surgery, possibly delaying the identification of this rare complication until the postoperative period. 16
Finally, conflicting results have been published on the impact of VT on postoperative time, which have been reported as either decreased13,17 or comparable to standard procedures,11,17 and no cost−benefit analysis has been conducted up to now on this innovative system.
The overall objective of this review was to assess data regarding the impact of a VT system on the perioperative outcome of patients undergoing minimally invasive surgery, compared to a standard pneumoperitoneum insufflation system, with special regard to postoperative pain levels.
Methods
Protocol and eligibility criteria
Objectives, methods of analysis, and criteria for inclusion of the revision were predefined and documented in the protocol registered on PROSPERO with registration number: CRD42020191835.
The study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A search on PROSPERO for upcoming studies was also conducted. All randomized controlled trials (RCTs) evaluating the effects of VT compared with a standard insufflation system in laparoscopic surgery on adult population were identified.
Search
A systematic and comprehensive search was performed using MEDLINE, EMBASE, Central Cochrane Library, and CINAHL Plus for studies published up to June 2020. In addition, the references of the identified trials and cross references were checked for additional eligible studies. No language restrictions were applied.
The search strategy involved the following search terms: “valveless trocar” OR “AirSeal®” AND “laparoscopic surgery” OR “pneumoperitoneum.” All studies reporting postoperative pain level (primary outcome) and operative time (secondary outcome) were considered for inclusion. Two authors independently confirmed the eligibility of the studies on the base of title and abstract; during the second time, a full-text revision was performed by the same authors. Any disagreement between the authors was resolved by discussion.
Data collection process
Data from the selected studies were extracted independently by 2 authors using a standardized form for data extraction. If consensus was not reached, a third author was consulted. From each study that was included, information about the authors, year of publication, study project, characteristics of the participants, intervention, and outcomes were collected.
Risk of bias assessment
Assessment of risk of bias in individual studies was independently determined by 2 reviewers, using the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) 18 regarding the primary outcome. Validity markers examined were appropriate generation of random allocation sequence, concealment of the allocation sequence, blinding of participants, health care providers, data collectors, and outcome adjudicators, and whether the analysis followed the intention-to-treat principle.
Statistical analysis and data synthesis
The primary outcome was the postoperative shoulder pain level, assessed postoperatively and after 24 hours; the pain level was analyzed using numerical rating scale (NRS) from 0 to 10 (with 0 = no pain and 10 = strongest pain imaginable). Data from studies that used a different score system were rescaled to be coherent with the range of values 0–10. The secondary outcome was the operative time, which was expressed in minutes.
For both outcomes, a meta-analysis was performed only if appropriate data were available (or inferable from the available data) from at least two studies among those selected. Statistical analysis was based on a random effect model and using inverse variance method. We considered mean differences (MD) as the main indicator of the VT effect (VT group mean less standard insufflation system group mean) at 95% confidence interval (95% CI). Heterogeneity was described using the I2-test. Data were analyzed using Review Manager software (RevMan Version 5.4; the Nordic Cochrane Centre, Copenhagen: the Cochrane Collaboration, 2020).
Results
Study selection and characteristics
The search strategy produced 106 bibliographic citations and 38 after the removal of duplicates. Of these, 31 were eliminated after reading titles and abstracts as they did not meet the eligibility criteria. The texts of the remaining studies were examined in detail: three studies were further excluded because they did not meet the inclusion criteria, while one was eliminated because it did not report outcomes regarding postoperative pain (flowchart in Fig. 1).

PRISMA 2009 flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
At the end of the revision process, we identified 3 studies that met inclusion criteria,12,19,20 with a total of 245 patients (Table 1). All studies that were finally selected for the review were RCTs published in English, evaluating the effects of VT compared with a standard insufflation system in minimally invasive surgery on adult population. These studies regarded both robotic assisted procedures and conventional laparoscopic procedures; the study of Bucur et al. 19 included patients undergoing renal surgery, while the remaining two studies12,20 regarded laparoscopic gynecological surgery.
Study Characteristics
LGS, laparoscopic gynecological surgery; LRS, laparoscopic renal surgery; MOT, mean operative time; NRS, numerical rating scale; ST, standard trocar group; VAS, visual analog scale; VT, valveless trocar.
Primary and secondary outcome assessment
In all the studies, the primary outcome assessed was shoulder pain at the end of surgery and at 24 hours postoperatively. The timing of the outcome first measurement was variable between one and six postoperative hours. Patients' reported evaluation of postoperative shoulder pain was assessed by NRS or visual analog scale (VAS); moreover, in their studies, Bucur et al. 19 also measured patients' morphine consumption and Sroussi et al. 20 presented the number of patients who required morphine, for pain evaluation.
In the study by Bucur et al. 19 there were no significant differences in postoperative global and shoulder pain between the 2 groups at every measured timepoint, both in the subjective evaluation or considering morphine equivalent consumption. In the article by Sroussi et al., 20 the incidence of shoulder pain was significantly lower in the VT group compared with the standard group and morphine consumption was significantly higher in the latter. In the last study 12 no statistically significant difference between groups was recorded in terms of distribution of pain scores across groups.
The operative time was reported in minutes in all studies12,19,20 and showed no significant difference between patients operated with VT and those who underwent standard trocar.
Study quality assessment and risk of bias
Assessment of the methodological quality of studies according to the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) is reported in Table 2.
Risk of Bias Assessment
L, low risk of bias; SC, some concerns.
In all examined studies, some concerns for risk-of-bias were detected, essentially related to possible deviations from the intended interventions, due to the lack of operative team blindness. While in all studies participants were not aware of their assigned intervention, obvious challenges existed in blinding the operators. Indeed, the laparoscopic device requires an insufflation system with a large touch screen display that enables the team to monitor key readouts; therefore, blinding the team during surgery is not feasible. However, authors did not exclude studies from the review based on the risk of bias.
Meta-analysis results
Shoulder pain
The meta-analyses related to shoulder pain measured immediately and 24 hours after surgery included data from all the studies (Table 3).
Results of Meta-Analysis
The effect size is calculated as MD and corresponding 95% CI.
Significance values.
95% CI, 95% confidence interval; MD, mean difference; ST, standard trocar group; VT, valveless trocar.
The following adjustments were made to allow for intrastudy data comparison: (i) Bucur et al. 19 and Sroussi et al. 20 present VAS mean values according to NRS assessments, while Madueke et al. 12 present their results comparing median values.
To make data comparable, we use results (median value, interquartile range, mean rank) reported by Madueke et al. 12 to estimate mean value and standard deviation (SD), using procedures elaborated by Luo and colleagues 21 and Shi et al., 22 which approximate the value of the mean starting from value of the median, its distance from the extreme value and mean value; (ii) with regards to data from Madueke et al., 12 who presented data relating to two subsamples for each insufflation system according to different level of intra-abdominal pressure, we calculated the mean and SD of each sample by weighting the means of the subsamples by their consistency, without taking into consideration the difference between intra-abdominal pressure; (iii) since Sroussi et al. 20 did not present values for SD related to shoulder pain, we estimated the SD as follows: starting from the P value we obtained the t statistic value, from the ratio between the difference of the means reported and the value of t we obtained the standard error.
SD was calculated as the ratio between standard error and square root of the sum of the inverse of the consistency of the patient groups of each study.
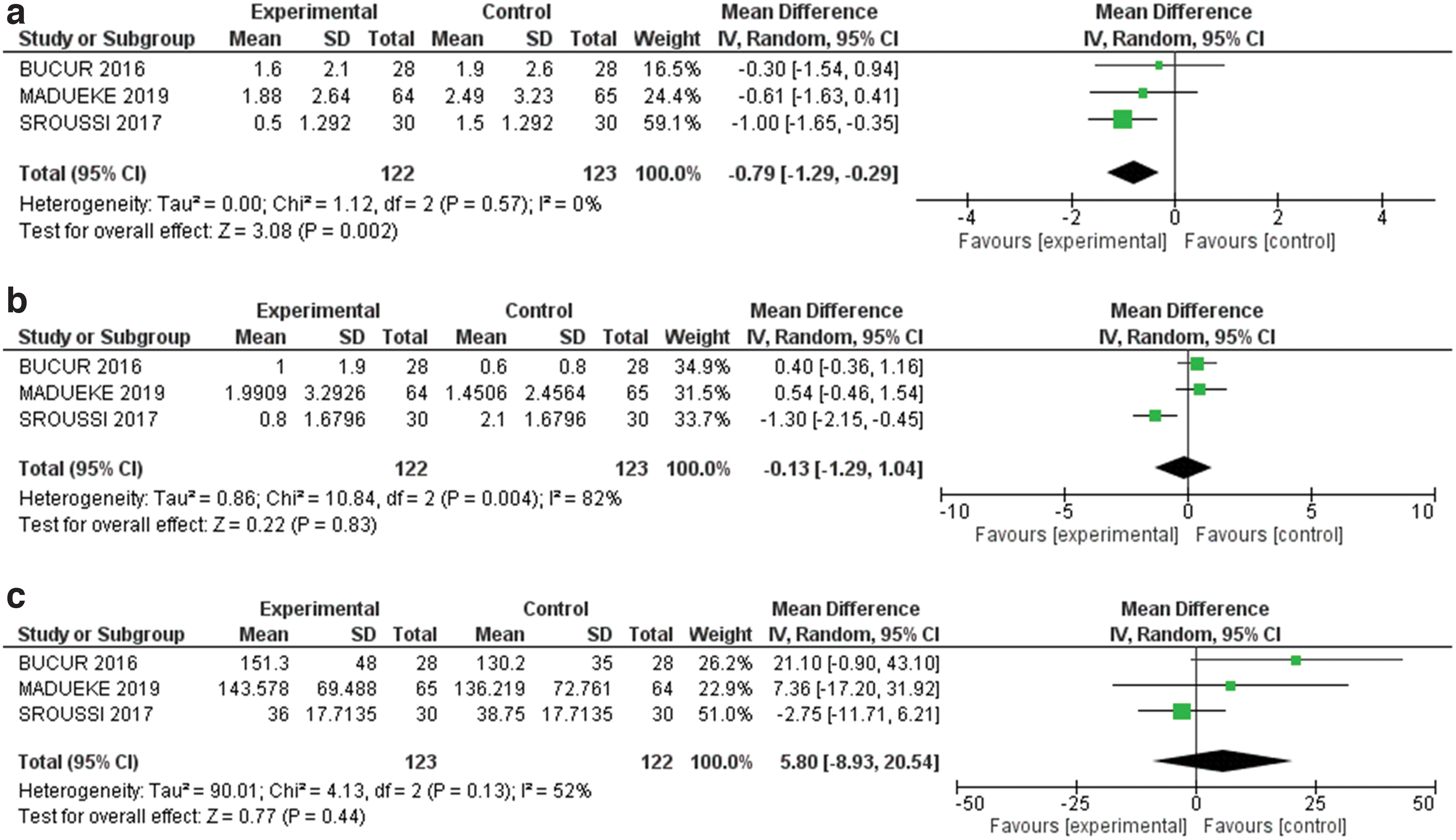
The meta-analysis results showed that the use of VT reduced pain at 24 hours compared to standard pneumoperitoneum insufflation system with a MD of −0.79 (95% CI: −1.29 to −0.29); reduction in pain assessment was statistically significant at 1% (z = 3.08; P = .002). Between-study heterogeneity was 0% (Fig. 2a). For shoulder pain at first postoperative time, MD was −0.13 (95% CI: −1.29 to 1.04), the result was not statistically significant (P = .83), and between-study heterogeneity was 82% (Fig. 2b).
Main results for Shoulder pain at 24 hours (panel
Operative time
The meta-analysis on operative time included data from all studies (Table 3): Bucur et al. 19 and Madueke et al. 12 presented the results as mean duration in minutes (and relative SD), while Sroussi et al. 20 reported for each technique median value and range of operative time in minutes. To compare data from Sroussi et al. 20 with the other studies, also in this case we estimated mean values using the statistic tool elaborated by Luo and colleagues 21 and Shi et al. 22
The results of the meta-analysis showed a not statistically significant increase in operative time with the use of VT: MD was 5.80 (95% CI: −8.93 to 20.54; P = .44), between-study heterogeneity was 77% (Fig. 2c).
Additional analysis
We present a second set of estimates without data based on median values to test the influence of these elements on our analysis. This implies to exclude Madueke et al. 12 from analysis on shoulder pain at day 1 and at first postoperative time and Sroussi et al. 20 from analysis on operative time (Table 4).
Results of Meta-Analysis Excluding Data Estimated by Median Values
The effect size is calculated as the MD and corresponding 95% CI.
Significance values.
95% CI, 95% confidence interval; MD, mean difference; ST, standard trocar group; VT, valveless trocar.
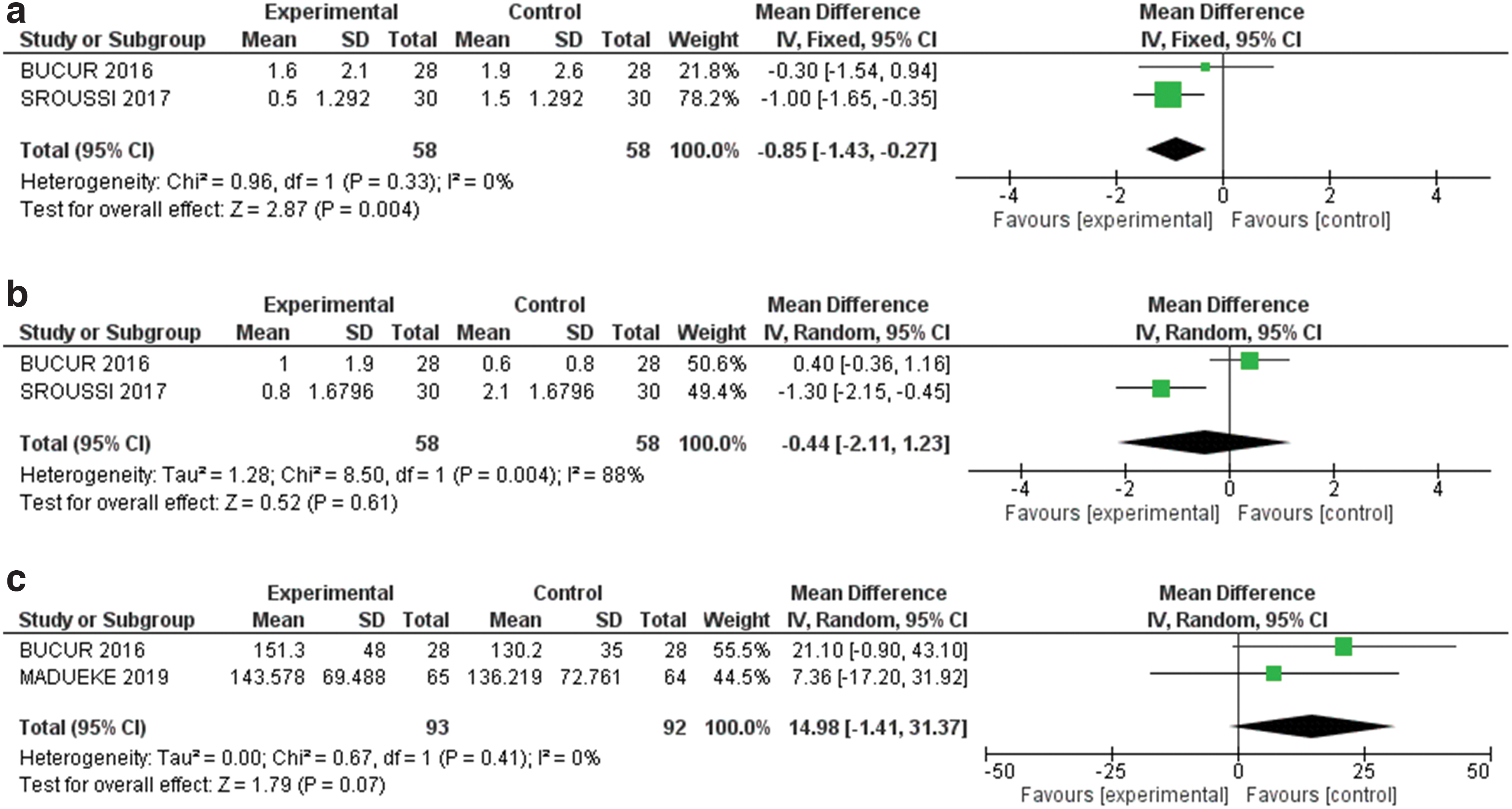
Removing Madueke et al., 12 improvement in shoulder pain at 24 hours is confirmed: MD was −0.85 (95% CI: −1.43 to −0.27), the result was still statistically significant at 1% (z = 2.87; P = .004), and between-study heterogeneity was 0% (Fig. 3a). Results for shoulder pain at first postoperative time: MD was −0.44 (95% CI: −2.11 to 1.23), still not statistically significant (P = .61), and between-study heterogeneity was 88% (Fig. 3b).
Additional analysis for Shoulder pain at 24 hours (panel
Removing Sroussi et al. 20 increased MD to 14.98 (95% CI: −1.41 to 31.37) and result was statistically significant at 10% (z = 1.79, P = .07), between-study heterogeneity was 0% (Fig. 3c).
Discussion
Although the minimally invasive technique, compared to open surgery, has reduced the severity of the surgical traumatism and postoperative pain, the common effort is still oriented to further improve this outcome that is associated with severe complications and among the first causes of prolonged hospital stay. 23
The etiology of postoperative pain following laparoscopic surgery is a multifactorial phenomenon that includes the insufflation of the abdominal cavity with CO2, which in turn causes distension of the abdominal tissues and abdominal cavity acidification.23,24 In addition, distension-induced neuropraxia of the phrenic nerve determines the typical painful shoulder localization, which can persist up to 24–72 hours after the end of the intervention. 25
Our review shows some acceptable evidence on the comparison of VT and standard trocar pneumoperitoneum insufflation system, suggesting a slight improvement in shoulder pain control at 24 hours postoperative using new-generation VT for laparoscopic surgery.
This result could be explained in the light of some features of the novel valveless insufflation system: it enables a stable pneumoperitoneum with continuous smoke evacuation and CO2 recirculation. 26 Conversely, standard trocars restore suitable pressures following repeated leaks using rapid insufflations that may cause overstretching of the diaphragmatic muscle fibers and postoperative shoulder pain, irritating factors that can be presumably limited thanks to the VT system characteristics.
According to Myles et al., 27 which aim to identify the minimal clinically important difference of postoperative pain by considering a large number of chirurgical interventions, the pain reduction found (0.79 point on NRS) falls within the range of moderate pain improvement (between 0.68 and 1.51) and on the edge of the large improvement range (between 0.8 and 2.16) identified by the article. Furthermore, our results, compared to the mean pain value of all the treated patients, equal to 2.12, represent a reduction in pain over than 37%. The clinical relevance of the mentioned results may be inconclusive and, even considering that for some authors a 33% decrease in pain value represents a reasonable standard to effect a relevant change in pain perception, 28 it seems clear to us that the choice to use a VT, also considering its high costs, requires further evaluations with complete and targeted trials.
There are many studies that aim to identify factors that can limit abdominal and shoulder pain after these types of surgery. Different levels of pneumoperitoneum (high versus low pressure values), the stability of the pressure curtain inflated, and the amount of CO2 absorbed by the patient were investigated as possible modifiable factors.
Numerous studies have shown better control of postoperative pain maintaining low levels of intra-abdominal pressure,29,30 but the quality of surgical vision and operative safety with the use of low-pressure pneumoperitoneum still needs to be established. 31
Considering the possible advantages with the use of a VT, in their nonrandomized trial, Shahait et al. 14 found a minor incidence of postoperative pain after robot-assisted radical prostatectomy performed with VT, but they interpreted this result strictly as correlated with shorter operative time, rather than to a reduced CO2 consumption. Notably, in our review, on the contrary, we observed weak evidence of an increase in operating times with the use of the VT, although this result was significant only when two of the three randomized trials were considered.
Even in the studies of Annino et al. 32 and Herati et al. 13 mean operative time was significantly shorter in the VT group, in contrast with our result. A possible interpretation can be given considering the different experience of the operators with the new VT system. This is an important factor considering that our counterintuitive data derive from the analysis of different type of operations, performed by different surgeons with their respective skills, while in the Annino et al. 32 and Herati et al. 13 studies the interventions were all conducted by the same experienced surgeon. In contrast, the lack of a rigid randomization process could have affected the operative times reported in the cited studies. In fact, other randomized studies that compared VTs and standard trocars confirmed overlapping operating times between the groups of patients.11,30
One limitation of this systematic review regards the lack of data about CO2 patient's consumption and absorption. Given the close correlation between CO2 insufflation and the development of postoperative pain in laparoscopy, it would be important to define whether the better pain control was linked with a lower environmental acidification.
One further weakness concerns the fact that the primary end point was assessed through a subjective parameter (pain reported by patients on NRS). Postoperative consumption of morphine could have been a more objective and widely accepted method for assessing pain after surgery, but data were lacking or insufficient, since only two of the three analyzed articles report data on postoperative morphine consumption, using two different units of measurement. However, in the study by Bucur et al. 19 there were no significant differences between the groups considering morphine equivalent consumption, and in the article by Sroussi et al. 20 morphine consumption was significantly higher in the standard group. We can reasonably infer that the available data on morphine consumption do not contradict the results obtained.
A valid project for a more accurate assessment of the validity of the valveless system use could be a well-structured randomized trial evaluating the postoperative consumption of opioids in relation to patient's intra-abdominal pressures and CO2 consumption.
Footnotes
Authors' Contributions
C.C.: This author conceived and designed the systematic review, screened studies for inclusion and assessed the risk of bias, extracted and interpreted the data from the articles, performed the data analysis, and wrote the article.
L.M.: This author helped design the systematic review, extracted and interpreted the data from the articles, performed the data analysis, and helped write the article.
G.T.: This author helped design the systematic review, screened studies for inclusion and assessed the risk of bias, and extracted the data from the articles.
G.T.: This author interpreted the data and reviewed the analysis of the data.
M.C.: This author screened studies for inclusion and assessed the risk of bias, extracted the data from the articles, and reviewed the analysis of the data.
This author performed a critical revision of the article.
E.F.: This author helped design the study and interpreted and analyzed the data.
All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.