
Abstract
Objectives:
To evaluate perioperative and functional outcomes of clampless laparoscopic tumor enucleation for completely endophytic renal tumors with the guide of intraoperative ultrasonography.
Methods:
We analyzed patients with clinically completely endophytic tumors, renal tumors, who underwent clampless three-dimensional (3D) retroperitoneoscopic laparoscopic tumor enucleation between January 2012 and January 2021. Patients with exophytic tumors were excluded. Intraoperative ultrasonography was used to map out the mass in all surgeries.
Results:
Overall, 57 patients underwent clampless 3D retroperitoneoscopic laparoscopic tumor enucleation. Mean surgical time was 131 minutes, and mean estimated blood loss was 202 mL. Mean hospital stay was 4.7 days. Major and minor postoperative complications occurred, respectively, in 3 and 10 cases. Only a patient had a positive surgical margin. One-year renal function did not differ from baseline.
Conclusion:
Our study showed that clampless laparoscopic enucleation guided by laparoscopic ultrasonography ensured satisfactory outcomes for completely intrarenal tumors, with excellent renal function preservation 1 year after surgery.
Introduction
According to the current European Urology Association (EAU) Guidelines, nephron sparing surgery (NSS) is the recommended treatment for cT1 renal cell carcinoma, both for oncological safety and preservation of the renal function. 1 Moreover, it is mandatory in selected clinical conditions requiring the maximum preservation of healthy renal parenchyma, such as chronic kidney disease, solitary kidney, or bilateral multifocal renal masses.2–4 NSS can be performed, by open-, pure laparoscopic-, or a robot-assisted approach, based on the surgeon's expertise and skills. 1
Nowadays, the use of warm ischemia is usually reserved for highly complex renal tumors to reduce intraoperative bleeding, and a selective or superselective clamping should always be considered, if feasible. 5 Hilar vessel clamping time is not to exceed 25 minutes, to minimize the significant loss of kidney function. 6
Furthermore, endophytic tumors are more challenging to resect, even for experienced surgeons, especially with laparoscopic techniques due to the lack of palpatory identification and tactile feedback. The use of intraoperative ultrasonography with a dedicated probe is recommended to overcome these drawbacks, providing details regarding the size, location, and blood supply of the renal mass. 7
This study aims to evaluate the outcome of three-dimensional (3D) clampless laparoscopic NSS of totally endophytic compared with exophytic renal tumors.
Materials and Methods
Patients
We retrospectively analyzed our prospective maintained database of all patients undergoing NSS from January 2012 to January 2021 in our unit. Inclusion criteria were a single intrarenal kidney tumor deemed feasible for NSS. Patients with a single renal unit or with cystic lesions, multiple renal masses, and tumors with an exophytic component were excluded.
All patients were evaluated preoperatively by a contrast-enhanced computed tomography scan of the abdomen. One author (C.G.) estimated the radius exophytic/endophytic nearness anterior/posterior location (R.E.N.A.L.) nephrometry score for each lesion. 8
We gathered the following intraoperative data: operative time (OT), estimated blood loss (EBL), and conversion to open or radical nephrectomy. Early postoperative complications were considered within 30 postoperative days and scored according to the Clavien–Dindo (CD) classification system. 9 Renal function impairment ratio, the positivity of surgical margins, and oncological follow-up were also collected. Renal function was compared 1 month and 1 year after surgery. To assess the “quality” of NSS, the margin, ischemia, and complications (MIC) score, defined by the absence of CD complication grade higher than 2, no positive surgical margins, and ischemia time less than 20 minutes, was used. 10 Data collection followed the principles of the Declaration of Helsinki and its amendments.
This study was conducted retrospectively, collecting data obtained for daily clinical practice, and all the procedures were performed as part of routine care. Consequently, our study did not require formal ethical approval. All patients signed an informed consent agreeing to share their anonymous information for the study.
Surgical technique
All procedures were performed by a single experienced laparoscopic surgeon, with the placement of three trocars, through a retroperitoneal approach. The patient is placed in the lithotomy position for the insertion of a retrograde mono J ureteral stent. This procedure is deemed mandatory to verify the integrity of the collecting system with the injection of physiological solution after tumor enucleation. Subsequently, the patient was placed in a flank position for better exposure of the Petit triangle, at the subcostal level. Two 10 mm trocars are placed under digital guidance: the first one is positioned 3 cm medially to the anterior axillary line, and the second one positioned laterally on the posterior axillary line. Then, the 12 mm optic trocar is placed under the tip of the XII rib on the midaxillary line.
A 3D camera (Endoeye 3D flex tip; Olympus®, Tokyo, Japan) is inserted and the surgeons wear 3D lenses, which are maintained during the entire procedure.
The perinephric fat is dissected to expose the Gerota's fascia, which is incised to isolate the kidney and to skeletonize the renal vein and artery, without clamping them. In patients with endophytic tumors, the ultrasonographic probe Aloka 4000 (UST-5534T-7.5 Ultrasound Aloka® Co., Ltd., Tokyo, Japan) is used to identify the margins of the renal mass and the optimal cleavage plane (Fig. 1A). Then, the cortex is incised with cold blade scissors, and the tumor was progressively excised (Fig. 1B, C). In the case of bleeders, bipolar forceps are used to coagulate the vessels.
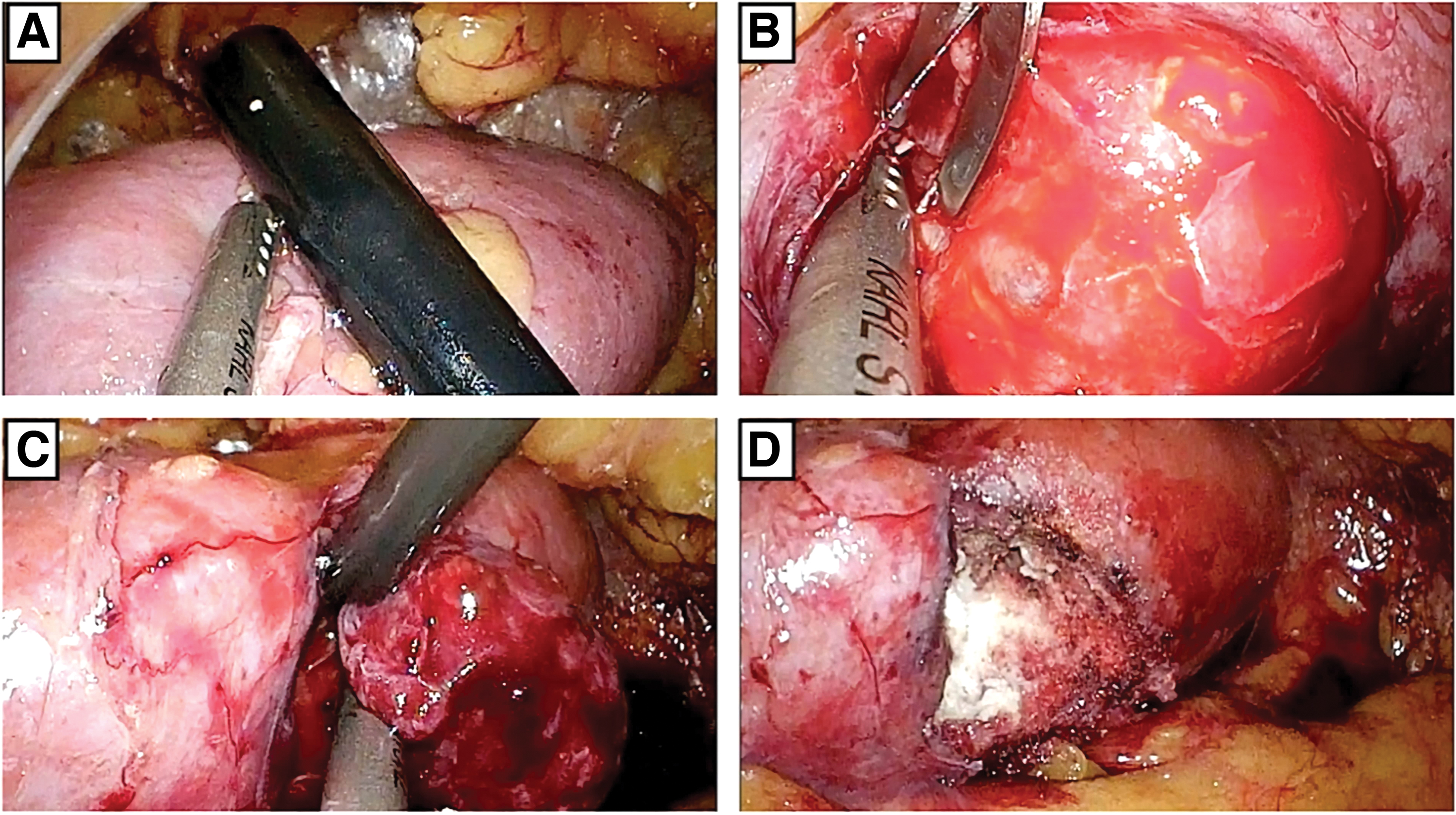
Surgical steps of tumor enucleation.
After tumor enucleation, the hemostasis is performed, completed punctually with monopolar scissors and the adjunct of gelatin matrix-thrombin sealants, such as Surgiflo® (Ethicon, New Brunswick, NJ) or FloSeal© (Baxter, Deerfield, IL) (Fig. 1D). A single layer of parenchymal 2-0 running suture with Hem-o-lok® pledgets sliding clip technique is used if deemed necessary. Finally, the excised tumor is pulled out, using a 10-mm ENDOPUCH RETRIEVER© bag (Ethicon, Inc., Somerville, NJ) through a skin incision.
Statistical analysis
Qualitative variables were described using absolute frequencies and percentages. Quantitative variables were described using the mean and interquartile range. Follow-up changes in biomarkers were calculated and analyzed using the Wilcoxon test. All statistical tests were two-tailed and P < .05 was considered to indicate statistical significance. Statistical tests were performed using IBM SPPS (v 26) software.
Results
Between the study periods, 57 patients met the inclusion criteria and were included in the analysis. Table 1 shows patients' demographics and characteristics. Mean age was 62 (55–71) years, and the Charlson comorbidity index was 4.2 (3–5). As for the tumor characteristics, the mean size was 37 (26–47) mm, and the mean R.E.N.A.L. score was 8.2 (7–9).
Baseline and Perioperative Data of Patients Related to Completely Endophytic Tumor Group
Data are presented as means (interquartile range) and frequencies (proportions).
ASA, American Society of Anesthesiologists; BMI, body mass index; CET, completely endophytic tumor; R.E.N.A.L., radius exophytic/endophytic nearness anterior/posterior location.
As shown in Table 2, mean OT was 131 (88–160) minutes, and EBL was 202 (140–240) mL. The mean length of stay was 4.7 (4–7) days, while the median 24-hour decrease in Hemoglobin was 1.6 (1.2–2.4) g/dL. All procedures were performed without the necessity of selective ischemia and completed without any conversion to radical nephrectomy. At least one postoperative complication occurred in 12 patients: 10 of them were minor, while 2 major complications (CD 3a or more) occurred. No case of postoperative urine leakage was detected. One patient needed super-selective embolization 8 days from NSS, and one required dialysis due to renal failure. An anatomopathological examination reported only 1 case of positive surgical margins. MIC score was achieved in 53 (93%) cases.
Perioperative Data of Patients Related to Completely Endophytic Tumor Group
Data are presented as means (interquartile range) and frequencies (proportions).
CD, Clavien–Dindo; CET, completely endophytic tumor; EBL, estimated blood loss; MIC, margin, ischemia, and complications.
Baseline and postoperative renal functional data are summarized in Table 3. No significant differences were found at 1 month and 1 year after surgery.
Preoperative, 1 Month Postoperative, and 1 Year Postoperative Renal Function Compared Using Paired Wilcoxon Test
Data are presented as means (interquartile range) and frequencies (proportions).
1MPO, 1 month postoperative; 1YPO, 1 year postoperative; Cr, creatinine; eGFR, estimated glomerular filtration rate; Pre, preoperative.
Discussion
NSS is currently the gold standard treatment for cT1 renal cell carcinoma, ensuring oncological safety and long-term preservation of kidney function.
Major limitations of the pure laparoscopic approach are a reduced range of instrument motion, lower perception of visual depth, due to conventional bidimensional optical lenses, and the absence of tactile feedback. The introduction of 3D lenses represented a technological step forward, leading to improved visibility and amelioration of surgical outcomes. 11
The presented study confirmed that 3D laparoscopy assisted by endocavitary ultrasonography allowed us to perform clampless NSS in highly complex endophytic tumors, and with acceptable postoperative morbidity. Indeed, our study pointed out that no patient required open conversion, nor concomitant or delayed nephrectomy. Moreover, the use of intraoperative ultrasonography is fundamental for the identification of the correct surgical plane, avoiding positive margins.
Matin also found that the use of laparoscopic ultrasonography (LUS) allowed better visualization of tissues, enhancing the two-dimensional laparoscopic view, with an increased amount and quality of information available to surgeons. 12 Moreover, the application of intraoperative LUS allowed the identification of tumor margins, maximizing the preservation of the surrounding healthy parenchyma and lowering the rate of negative surgical margins. 13 Intraoperative US is also strongly recommended for exophytic tumors in patients with reduced baseline function to maximize normal parenchymal tissue sparing and make even on-demand or selective ischemia unnecessary.
The main disadvantage of intraoperative US application is the additional surgical time, which could determine a prolonged ischemia time, increasing hypoxia and related reperfusion injuries. Nevertheless, in experienced hands, a clampless technique is feasible, preserving preoperative renal function, according to the current literature. 14
The use of hemostatic renorrhaphy is associated with a decline of renal function after NSS. Indeed, the merging of healthy parenchyma and branches of renal segmental arteries in the inner part of the corticomedullary sutures mainly causes the damage. 15 Sutureless NSS for completely endophytic tumors was feasible in a low rate of surgeries and the other ones required a hemostatic renorrhaphy. In any case, a single layer approach did not influence negatively long-term functional outcomes, as reported by Bertolo et al. 16
Table 4 shows the available literature describing the use of LUS during laparoscopic NSS for completely endophytic renal tumors.17–25 Our results are in line with those of the other articles. The only exception is the change in glomerular filtration, which was lower in our study. Engel and Williams demonstrated the best preservation of renal function, but their clampless laparoscopic approach was hand-assisted. 25
Perioperative Outcomes of Laparoscopic Partial Nephrectomy Assisted by Intraoperative Ultrasound Series for Completely Endophytic Renal Tumors
Data are presented as means (interquartile range) and frequencies (proportions).
1MPO, 1 month postoperative; 1YPO, 1 year postoperative; CD, Clavien–Dindo; EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; OT, operative time; PO, postoperative; PSM, positive surgical margins; WIT, warm ischemia time.
Our work is not devoid of limitations. First of all, the retrospective nature of the study. Second, all procedures were performed by a single experienced surgeon, and the same results might not be achievable by less skilled surgeons. Finally, the number of completely endophytic renal tumors was relatively small, suggesting the need for multicentric studies.
Conclusion
On experienced hands, clampless renal tumor 3D laparoscopic enucleation guided by LUS ensured satisfactory oncological and functional outcomes for completely intrarenal tumors. The combination of zero-ischemia with intraoperative ultrasonography in laparoscopic NSS provides accurate anatomical details, minimizing healthy tissue resection and assuring oncological radicality with excellent preservation of renal function. According to our experience, LUS and clampless technique should be mandatory in cases of NSS for completely endophytic lesions, especially for patients with reduced preoperative renal function.
Footnotes
Authors' Contributions
M.D.B. and V.I. conceived the presented idea. C.G. and S.S. developed the theory and performed the computations. A.M. and M.D. verified the analytical methods. V.F. encouraged W.G. and G.S. to compare the present study with literature and supervised the findings of this work. All authors discussed the results and contributed to the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.