
Abstract
Background:
The effectiveness of laparoscopic surgery for adhesive small bowel obstruction (ASBO) remains unclear. We aimed to compare the outcomes and safety of open and laparoscopic surgeries for ASBO.
Methods:
In this retrospective study, we analyzed an inpatient database of 42 national university hospitals in Japan. Patients who underwent surgery for the first episode of ASBO between April 2013 and March 2018 were identified. Using the propensity score method, patients who underwent laparoscopic surgery were matched one-to-one with those who underwent open surgery. We investigated postoperative clinical outcomes, including morbidity, mortality, length of hospital stay (LOS), and recurrence.
Results:
Overall, 306 and 96 patients underwent open and laparoscopic surgery, respectively (96 propensity score-matched pairs). The incidence rates of postoperative morbidity, mortality, and recurrence were comparable between the two groups. Cox regression analysis revealed a hazard ratio (HR) of 1.020 (P = .959) for readmission due to ASBO in the laparoscopic surgery group relative to the open surgery group. Postoperative hospital stay was longer for open surgery than for laparoscopic surgery (13.0 days versus 10.0 days, P < .001). Cox regression analysis revealed that laparoscopic surgery was associated with earlier postoperative discharge compared with open surgery (HR 1.641, P = .002).
Conclusions:
The postoperative LOS was shorter with laparoscopic surgery than with open surgery for ASBO, but there were no differences between the procedures in other clinical outcomes. Laparoscopic surgery is suitable to treat patients with ASBO.
Introduction
Adhesive small bowel obstruction (ASBO) is one of the most common causes of postoperative hospital admission. Generally, patients with ASBO initially undergo nonsurgical treatment.1–4 However, a high failure rate of conservative management and the need for surgery have been documented.4–6
In the recent decades, studies with a small sample size have elucidated the feasibility and safety of laparoscopic surgery for ASBO.7–11 Although laparoscopic surgery reduces the risk of ASBO by 75% compared with open surgery, 12 it remains unclear whether this effect applies to surgery for preexisting ASBO. Recent studies suggest that laparoscopic adhesiolysis is associated with better short-term outcomes, such as shorter length of hospital stay (LOS) and lower 30-day morbidity and mortality, compared with open surgery.11,13 However, these studies did not consider the impact of previous episodes of ASBO or evaluate long-term outcomes.
Therefore, this study aimed to compare the short- and long-term clinical outcomes of open and laparoscopic surgery for first-episode ASBO through a propensity score-matched analysis of a large-scale dataset from 42 large national university hospitals in Japan.
Patients and Methods
Data source
This study used data from the Diagnosis Procedure Combination (DPC) database of 42 national university hospitals. This database includes data from over 1000 Japanese hospitals on administrative claims, discharge summaries, and patients' demographic characteristics, diagnosis, comorbidities at admission, complications after admission (recorded using International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10] codes), surgeries and procedures performed (recorded using Japanese original codes), duration of anesthesia, and use of blood transfusion. 14
Patient selection and data extraction
Adult patients admitted to certain national university hospitals with a diagnosis of first-episode ASBO (ICD-10 code K56.5) between April 1, 2013 and March 31, 2018 were included.
We excluded patients who did not undergo open or laparoscopic surgery during hospitalization; those with a nonadhesive cause of small bowel obstruction, such as intussusception (ICD-10 code: K56.1), volvulus (K56.2), peptic ulcers with perforation (K27.1, K27.2, K27.5, or K27.6), gastrojejunal ulcers with perforation (K28.1, K28.2, K28.5, or K28.6), hernia with obstruction (K40.0, K40.3, K41.0, K41.3, K42.0, K43.0, K43.3, K43.6, K44.0, K45.0, or K46.0), paralytic ileus (K56.0), gallstone ileus (K56.3), intestinal diverticula (K57.x), Meckel's diverticulum (Q43.0), Crohn's disease (K50.x), ulcerative colitis (K51.x), intestinal vascular disorders (K55.x), or unspecified intestinal obstruction (K56.6); those who had experienced episodes of ASBO, Crohn's disease, ulcerative colitis, or abdominal or pelvic radiotherapy in the previous 2 years; and those younger than 20 years or older than 85 years.
The resulting cohort consisted of adult patients aged 20–85 years who were admitted for first-episode ASBO and underwent open or laparoscopic surgery during the study period. Body mass index was categorized as <18.5, 18.5–25, 25–35, and >35 kg/m2. The Charlson comorbidity index was calculated using Quan's protocol, and the ICD-10 codes for 12 comorbidities were converted into a summated score for each patient. 15 Early surgery was defined as surgery for ASBO performed on the day of or the day following admission (postadmission days 0 and 1).
Disclosure of Ethical Statement
The protocol for this research project has been approved by a suitably constituted Ethics Committee of The University of Tokyo (approval No.: 2020388NI) and it conforms to the provisions of the Declaration of Helsinki. The requirement for informed consent was waived by the ethics committee because of the anonymous nature of the data.
Statistical analysis
One-to-one nearest-neighbor propensity score matching of patients who underwent laparoscopic surgery and those who underwent open surgery was performed with a caliper width of 0.2 of the standard deviation of the logit of the propensity score. Balance diagnostics after matching were performed by calculating the standardized difference between the matched groups. A standardized difference >0.1 was considered significant. 16
Categorical variables were compared using the chi-square test. Continuous variables are presented as medians with interquartile ranges and were compared using the Mann–Whitney U test. Postoperative complications were investigated using logistic regression analysis, and the results of this analysis are presented as odds ratios with confidence intervals (95% CIs). Recurrent obstruction-free survival after index surgery was evaluated using the Kaplan–Meier estimator. Recurrent obstruction-free survival and LOS after index surgery were analyzed using the Cox regression model, and the results were described as hazard ratios (HRs) with 95% CIs. All reported P-values were two tailed, and a P-value of <0.05 was considered statistically significant. Stata/MP 15.0 (StataCorp., College Station, TX) was used for statistical analysis.
Sensitivity analysis
We performed a sensitivity analysis in which patients who underwent early surgery for ASBO were excluded. These patients were those in whom nonsurgical management might not have been possible, and they likely underwent surgery due to ASBO complicated with mesenteric ischemia, including closed-loop small bowel obstruction.
Results
Between April 2013 and March 2018, 2669 patients were hospitalized for first-episode ASBO (Fig. 1). Among them, we included 402 who underwent open (n = 306) or laparoscopic surgery (n = 96). After one-to-one matching of the patients in the open and laparoscopic surgery cohorts using propensity scores, the resulting cohort consisted of 188 patients, with 94 patients in each group. The C-statistic for goodness of fit in the propensity score model was 0.679 (95% CI, 0.617–0.734).
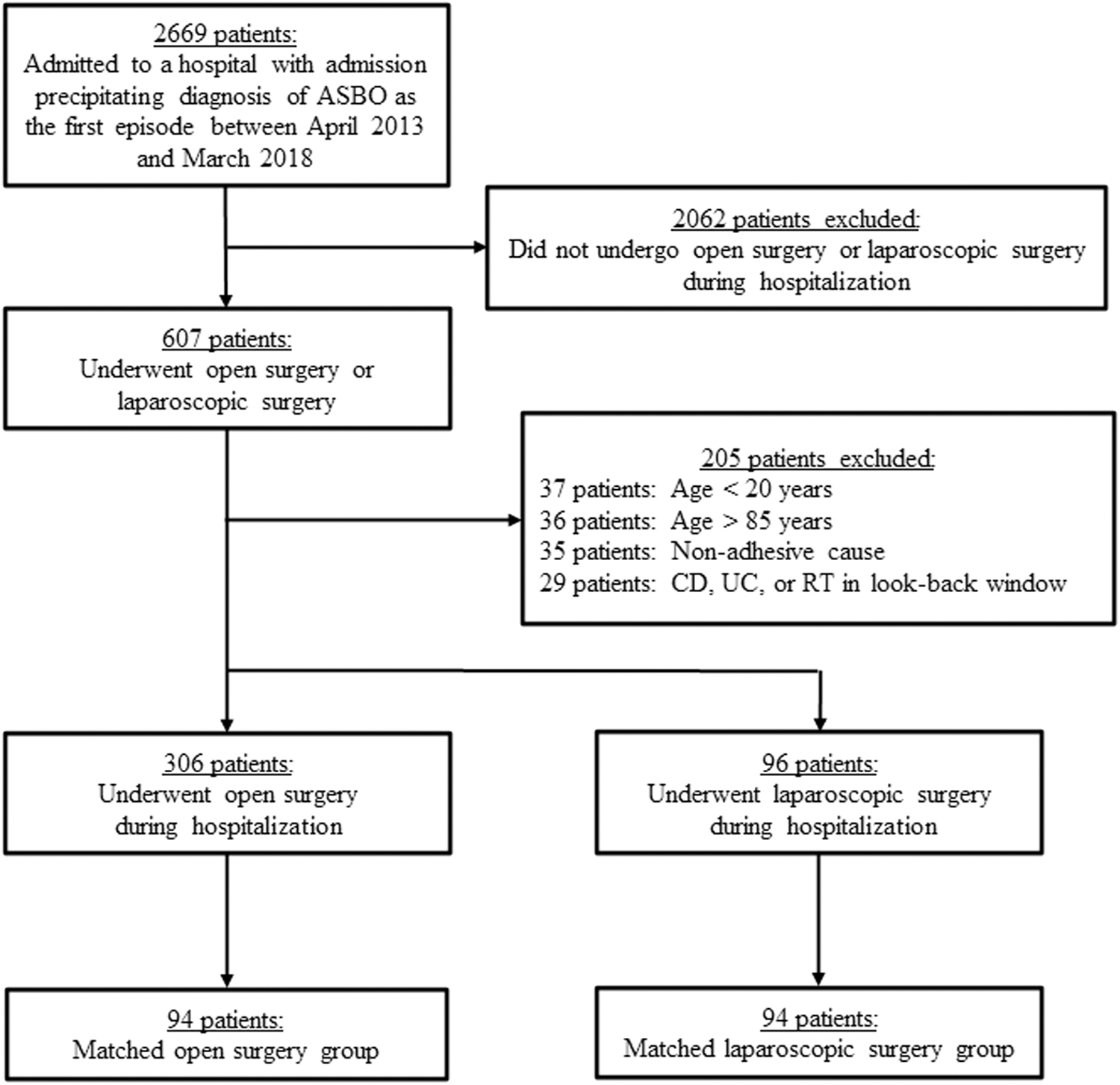
Flowchart of the selection of study groups. CD, Crohn's disease; RT, radiotherapy; UC, ulcerative colitis.
Table 1 shows the demographic characteristics of the patients in the unmatched and propensity-matched groups. Several factors, namely, body mass index, Barthel index score, Charlson comorbidity index, early surgery, and partial resection of the small intestine, were unbalanced between the open and laparoscopic surgery groups with absolute standardized difference values >0.1. Balance diagnostics revealed that, except for age, our cohorts were well-matched with absolute standardized difference values <0.1.
Characteristics of Patients in the Unmatched and Propensity-Matched Groups Who Underwent Laparoscopic or Open Surgery for Adhesive Small Bowel Obstruction
Standardized differences are calculated as shown in the Patients and Methods section.
BMI, body mass index; SD, standard deviation.
There were no differences in recurrence within 30 days, 90 days, 1 year, and 3 years of index surgery (4.3% versus 4.3%, P > .999; 5.3% versus 7.4%, P = .551; 8.5% versus 8.5%, P > .999; and 13.0% versus 12.0%, P = .824, respectively) and in the overall risk of recurrence (14.9% versus 14.9%, P > .999) between the open and laparoscopic surgery groups (Table 2). There were no differences in the rates of mortality within 30 days of index surgery, in-hospital mortality, and postoperative complications between the two groups (1.1% versus 0%, P > .999, 8.5% versus 6.4%, P = .578, 5.3% versus 4.3%, P > .999, respectively). Patients in the laparoscopic surgery group had a shorter postoperative LOS than those in the open surgery group (13.0 days versus 10.0 days, P < .001) (Supplementary Table S1).
Outcomes of 94 Pairs of Propensity-Matched Patients in the Laparoscopic and Open Surgery Groups
Table 3 demonstrates the results of the logistic regression analyses of ASBO recurrence, mortality, and postoperative complications associated with laparoscopic surgery with reference to those associated with open surgery in the propensity-matched groups. The risks of ASBO recurrence, postoperative morbidity, and mortality were comparable between the two groups. Cox regression analysis revealed that no factors increased the risk of recurrence of ASBO (Supplementary Table S2). Kaplan–Meier analysis revealed that recurrent obstruction-free survival following index surgery was also comparable between the two groups (Fig. 2). Laparoscopic surgery was associated with earlier discharge after surgery (shorter LOS; HR 1.641, 95% CI, 1.203–2.240; P = .002) than open surgery (Table 4).

Rate of recurrence of adhesive small bowel obstruction after index surgery among patients in the open surgery group (solid line) and those in the laparoscopic surgery group (dotted line). The plus and cross marks represent censoring of data in the open and laparoscopic surgery group, respectively.
Results of the Logistic Regression Analyses of Outcomes in 94 Pairs of Propensity-Matched Patients
Odds ratios for the laparoscopic surgery group with reference to the open surgery group are shown.
CI, confidence interval; Inf, infinity.
Results of the Cox Regression Analysis of Postoperative Length of Hospital Stay After Index Surgery in the Propensity-Matched Cohort
The outcome in this analysis was hospital discharge.
CI, confidence interval.
A sensitivity analysis performed after excluding 25 patients (26.6%) who underwent early surgery in each group (Supplementary Table S3) showed results similar to those of the primary analyses, with no differences in postoperative mortality, morbidity, and ASBO recurrence. As seen in the primary analysis, laparoscopic surgery was associated with earlier discharge than open surgery (HR 1.507, 95% CI 1.042–2.181, P = .030; Supplementary Table S4).
Discussion
There were no differences in the rates of ASBO recurrence and postoperative complications between open and laparoscopic surgery in this multicenter retrospective cohort study of propensity-matched patients with first-episode ASBO using a large-scale Japanese database. Furthermore, laparoscopic surgery was associated with a shorter LOS than open surgery. These results suggest that laparoscopic surgery is safe and feasible for use in patients with first-episode ASBO.
A previous study found laparoscopic surgery for ASBO to be associated with a high incidence of early ASBO recurrence requiring surgery, 17 whereas our data demonstrated no difference in recurrence between the laparoscopic and open surgical groups. One of the reasons for this discrepancy could be that our enrollment was restricted to patients with first the episode of ASBO because the recurrence risk of ASBO increases with the number of episodes, 18 while the number of previous episodes of ASBO was not reported in the above study.
Laparoscopic adhesiolysis has been found to be associated with a significant reduction in the 30-day mortality and morbidity 13 and a shorter LOS. 11 However, the impact of previous episodes of ASBO has not been considered in these studies. A key strength of our study is that we only enrolled patients with first-episode ASBO, because we considered patients with a complex history of ASBO to be more likely to undergo open surgery. Another key strength is that all data were from teaching hospitals—the high-quality surgery performed at these hospitals may have contributed to the low 30-day mortality rate observed (1.1% in the open surgery group and 0% in the laparoscopic surgery group). A previous study reported high 30-day mortality rates of 4.7% for open surgery and 1.3% for laparoscopic surgery. 13
Laparoscopic surgery has been found to be associated with fewer postoperative adhesions, a shorter postoperative LOS, and earlier recovery of bowel function than open abdominal surgery12,19–22; this is in line with our findings of a shorter LOS in the laparoscopic group than in the open surgery group.
In our study, the overall incidence of recurrence was comparable between the two groups (14.9%). Accordingly, studies have reported an overall recurrence rate of 15%–20% in patients who underwent surgery to treat ASBO.18,23 The consistency of these findings confirms the validity, reliability, and generalizability of our results.
A potential problem in the surgical treatment of ASBO using laparoscopy is accidental perforation during adhesiolysis. Suter et al. reported a higher rate of bowel injuries with laparoscopic surgery than with open surgery for ASBO. 24 Intestinal perforation occurs in 7%–16% of cases after laparoscopic surgery and 4%–14% after open surgery for ASBO.11,21,24–29 In our study, the incidence of postoperative intestinal perforation was 0% in both groups. However, the incidence of accidental perforation during adhesiolysis remains unknown.
This study has several limitations. First, the patients' surgical history, including information on any abdominal surgeries before ASBO occurrence, the procedure used therein, and abdominal organ diseases, was not available due to the nature of the DPC data. In particular, there was no information on the number of prior abdominal surgeries. Although this information does not correlate with risk of conversion to laparotomy,24,30–32 it can influence the selection of surgical approach for ASBO. In addition, patients who previously underwent highly invasive surgery or surgery that could cause severe abdominal adhesions, such as surgery for diffuse suppurative peritonitis before developing ASBO, are more likely to undergo open surgery. Second, conversion to open surgery was recorded as open surgery, and the proportion of patients who required conversion was unknown. Third, it is difficult to determine the appropriate surgical approach for recurrent ASBO based on our results because patients with previous episodes of ASBO were excluded. Therefore, our results may not be applicable to patients with recurrent ASBO. Finally, we could not minimize the loss to follow-up. The DPC system does not capture information on the same patients upon admission to other hospitals outside of its designated scope. Therefore, the recurrent obstruction-free survival after index surgery observed in this study may have been overestimated.
Conclusions
Laparoscopic surgery is safe and feasible and associated with a shorter postoperative LOS than open surgery in patients with ASBO. Further studies are needed to evaluate the additional advantages of laparoscopic surgery in these patients.
Footnotes
Authors' Contributions
Y.Y. designed the study, performed the research, and drafted the article. T.O. acquired the data. All authors take responsibility for the integrity of the data and the accuracy of the data analysis. M.K. and Y.S. revised the article. All authors have read and approved the final article.
Acknowledgments
The data for this study were provided by the Database Center of the National University Hospitals, The University of Tokyo Hospital. The use of the data was approved by the Database Center Management Committee of the National University Hospital Council of Japan (2021-K001).
Data Sharing and Data Accessibility
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.