
Abstract
Background:
The introduction of splenectomy in pediatric robotic surgery programs remains controversial. The aim of this study is to evaluate the feasibility and safety of robotic assisted splenectomy (RAS) in children and compare its outcomes with the laparoscopic splenectomy (LAS).
Method:
A single institution retrospective study was performed (2011–2020). We used the minimally invasive splenectomy score described by Giza et al. to measure the level of technical difficulty. The data collected for each procedure included its duration, the need for blood transfusion, complications, analgesic use, and the length of hospital stay. A standard univariate analysis is applied.
Results:
We recorded 41 cases (26 LAS and 15 RAS). The mean age was 11 years [7.00; 13.5]. The operating time was 97 minutes [85.5–108] for LAS and 223 minutes [190–280] for RAS (P < .001). The length of stay was 6.50 days [5.00–8.00] for LAS and 5 days [5.00–5.50] for RAS (P = .055). The cumulative use of level III analgesic was not statically different (P = .29). Two cases of difficult splenectomy were found in each group with comparable performances. In the RAS, we demonstrated the improved outcomes with the progression of the learning curve of a single surgeon.
Conclusions:
In our experience (as in the literature), RAS remains safe, but offers no additional advantage compared to laparoscopy as the cost and the operating time are higher. Our study has the advantages of having a 9 years long evolving experience, including broad indications in comparison to other pediatric studies.
Introduction
In 1590,
Materials and Methods
This is a 9-year retrospective study identifying all minimally invasive pediatric splenectomies in our institution between 2011 and 2020.
We selected broad indications, which we discussed with the hematology and oncology teams of our pediatric hospital. We performed splenectomies for benign hemopathies [N = 36]: (sickle cell disease, thalassemia, pyruvate kinase deficiency, Blackfan-Diamond, Minkowski-Chauffard, idiopathic thrombocytopenic purpura), for tumors [N = 15]: (epithelial, mesothelial, dermoid), and for a case of Nieman Pick disease [N = 1].
All the surgeons in the team are trained for LAS and a referring surgeon performs RAS. The distribution of patients was random.
The level of difficulty was evaluated according to the minimally invasive splenectomy score (MISS) proposed by Giza et al. 4 classifying splenectomies in two groups: simple and difficult. The intervention was considered as simple if the score was lesser than 3 points. It is calculated by evaluating 5 items: Whether the patient has a partial (+3 points) or a total resection (0 point), thrombocytopenia (+1 point if platelet count is >40.000/mm3), overweight (+1 point if body mass index [BMA] >30), splenomegaly (+1 point), and/or hepatopathy (+3 points if presence of liver cirrhosis or tumor) as detailed in Table 1.
The Minimally Invasive Splenectomy Score According to Giza et al. 4
MISS <3 simple splenectomy; MISS ≥3 difficult splenectomy.
MISS, minimally invasive splenectomy score.
All our LAS were performed with an anterior approach, which allows a unique installation in case of an associated cholecystectomy. The triangulation of the operating trocars depended on the size of the spleen. Extraction of the specimen was done by enlarging the left iliac trocar's incision.
For RAS, the patients were installed in a supine position. We used a 12 mm umbilical trocar, two 8 mm trocars: one in the left flank and the other in the epigastric region, and a 5 mm help trocar between the first two. The short vessels and the splenic pedicle are approached anteriorly. Once fragmented in the Endobag, the piece is extracted through the 8 mm incision of the left flank, which is enlarged to 12 mm.
The studied items were the operative duration, the use of hemostatic, the need for transfusion, conversion, the duration of drainage, the consumption of level III analgesics, and the length of hospital stay. Morbidity and mortality were assessed by the Clavien Dindo complications score. 4
A standard univariate statistical study was conducted. We used the statistical tool “Medistica. pvalue.io 2020.” 8 Qualitative variables were compared using a chi-square test. Otherwise, if the conditions for performing this test are not met, the exact Fisher test is used. Quantitative variables were compared by a Student's t-test for Gaussian variables, and by a Wilcoxon-Mann-Whitney test for non-Gaussian variables. A difference is considered statistically significant when the p-value is less than or equal to .05.
Research ethics approval was obtained by the Institutional Review Board of our hospital.
Results
Our cohort consisted of 41 patients over 9 years, including 10 partial splenectomies (24.23%). The average age was 11 years [7–13.5]. We recorded 15 cases of RS, of which 40% were partial versus 26 cases of LS, of which 15% were partial (Fig. 1).
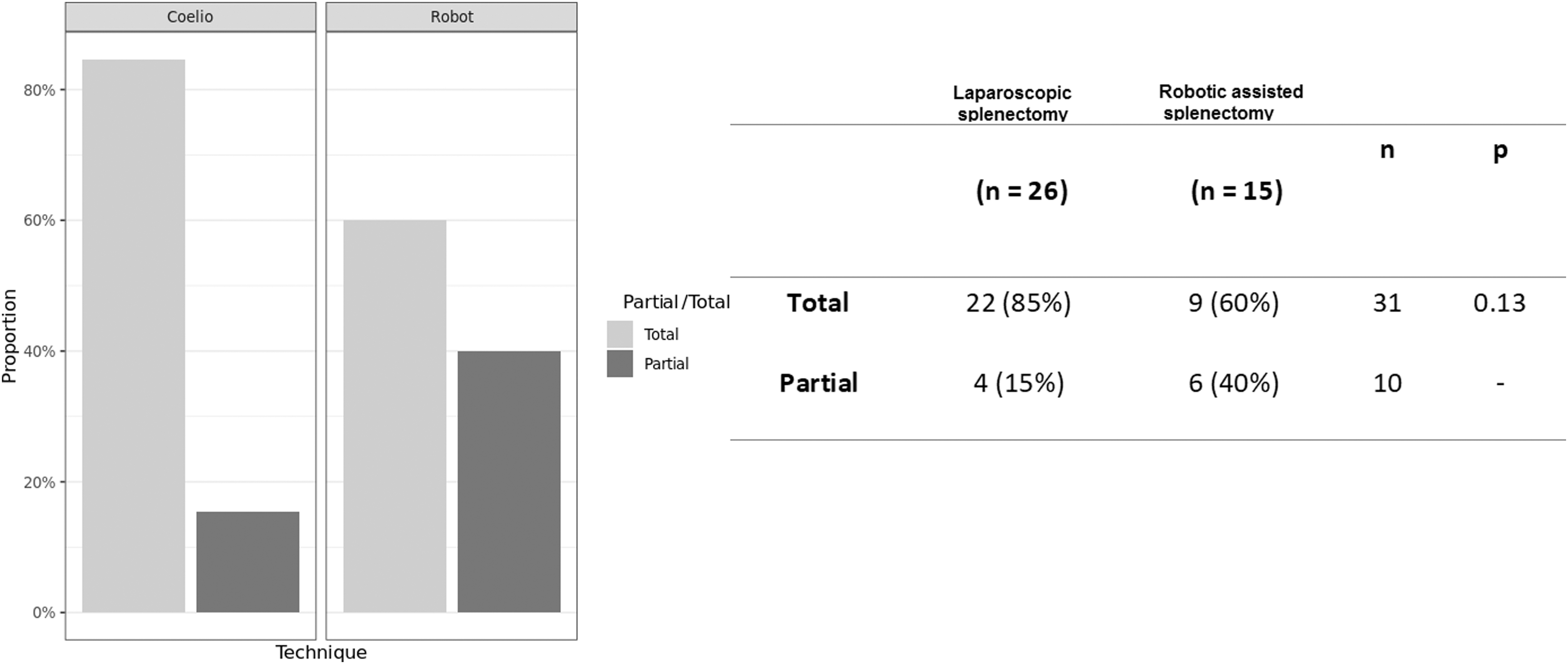
Patients distribution depending on the minimally invasive technique. LS, laparoscopic splenectomy; RAS, robotic assisted splenectomy.
Comparing the two techniques, the operating time was significantly higher in RS (P = .001) with an average of 223 minutes [190–280] versus 97 minutes [85.5–108] for LS.
Whatever the technique, drainage has not been systematic. It was done in only 26.92% of LS and 20% of RS, with an average duration of 3.08 days [0–5], (P = .51).
The surgical technique did not influence the consumption of level III analgesics (P = .29), nor the length of hospital stay, which was 6.50 days for LS [5.00–8.00] and 5 days [5.00–5.50] for RS (P = .056).
Our operative complication rate was 4.9% without statistical significance depending on the technique (P = .13). They were dominated by bleeding due to a tear in the splenic vein that was not controlled by hemlocks, indicating a conversion in one case (MISS <3). Intraoperative hemostatic drugs were used in 12% cases in laparoscopy and 6.7% in RS with no statistically significant difference (P = 1). Same for transfusion: 15% for LS and 7.1% for RS (P = .64).
As for Clavien-Dindo <2 complications, we counted a case of secondary involution of a hemispleen following a MISS ≥3 RS and a case of postoperative splenosis nodes following a MISS ≥3 LS; these were two small masses in the splenectomy lodge that have been respected. There were no Clavien-Dindo complications >3 and only one redo for totalization following a RS MISS ≥3.
Splenectomies with MISS ≥3 accounted for 26.82% of the cohort. The level of difficulty did not influence the operating time between the two groups (P = .2), no significant differences were seen in blood loss, hemostatic use (P = .24), analgesic use (P = .29), drainage time (P = .84), duration of hospital stay (P = .31), nor in the complications rate (P = 1) regardless of the minimally invasive technique chosen.
We studied the learning curve of RS performed by 1 surgeon. Complications occurred in 11% of simple RS and in 20% of difficult RS without statistical significance (P = .6). As for the operating time, we recorded the longest duration at the beginning of the experience (355 minutes), it has shortened over the last years with an average duration going from 338.5 minutes in 2016 to 193.5 minutes in 2019 (Fig. 2).

The learning curve of a single surgeon in pediatric robotic splenectomy.
We checked whether a longer time in the RS group was related to higher number of partial splenectomies by analyzing partial and total splenectomy duration separately. The mean rank of operative time is not significantly different according to the type of resection (P = .098).
Discussion
There are few pediatric series comparing LAS and RAS. Published adult articles report similar safety findings, but have shown, as in our study, a longer operative time in robotic surgery.5,6 Larger pediatric studies deserve to be conducted. Unlike in adults, hemodynamic stability is quickly threatened in case of blood loss. Pediatric spleen has its anatomical specificities: thicker capsule, perpendicular segmentation, and terminal vascularization. 1
Adult surgeons are more trained and have longer follow-up. There are more benefits of RAS than LAS in their studies, such as less blood loss and fewer conversions. 3
The pediatric series that is closest to ours is the one conducted by Mbaka et al. in 2017, 7 which had 11-year follow-up with a total of 55 splenectomies performed by the same operator who was faster in RAS [N = 32] than in LAS [N = 23], but with longer hospital stay. They demonstrated the safety of the robot but do not specify the arguments that made them chose one technique over the other.
The team of Shelby et al. in 2021 examined minimally invasive pediatric splenectomy exclusively for benign hereditary hematologic disease (24 patients in 5 years). 3 They recorded similar results to ours except for the operating time, which was similar in RAS and LAS. The robot had shorter hospital stay, but like other authors, 6 they pointed out its cost (44,724$ in RAS vs. 30,255$ in LAS, P = .01). In this specific indication, postoperative complications are dominated by the initial pathology expressions: Vaso-occlusive crisis, acute chest syndrome, and influenza.
Partial splenectomy (24% of cases in our study) is indicated whenever possible to preserve splenic function and avoid possible thromboembolic and infectious complications. However, it is itself a technical surgical challenge due to the risk of excessive bleeding and possible spread (splenosis, parasitosis). In the MISS, subtotal splenectomy is worth 3 points, which immediately classifies it as “difficult” regardless of the comorbidities of the patient. Therefore some authors, in the profit-risk balance, prefer to indicate a total splenectomy, which can be considered as more conservative than partial.9,10
Giza et al. in 20144 proved the robot's superiority over complex splenectomies with objective criteria: shorter operating time (84 vs. 97 minutes in LAS) and less blood loss (31 vs. 157 mL in LAS). In our experience, we did not find any difference in performance between the two techniques on the difficult cases. Their results could be reproducible on larger multicentric studies. The theoretical and sometimes subjective advantages of the robot, such as ergonomics, optical stability, range of motion, gesture precision, and better exposure through 3D vision, could be evaluated by a questionnaire study. Previous work has shown that the robotic simulation platform offers less cognitive stress when performing surgical tasks compared to the same simulated tasks in laparoscopy.11,12
Conclusion
Minimally invasive robot-assisted pediatric splenectomy remains safe, but offers no additional advantage compared to laparoscopy as the cost and the operating time are higher. Our study has the advantages of having a 9 years long evolving experience, including broad indications in comparison to other pediatric studies.
Footnotes
Authors' Contributions
I.B. and O.A. conceived the presented idea. I.B., T.P., D.A.A., C.L., and A.L.M. developed the theory and performed the computations. S.M. and O.A. verified the analytical methods. O.A. supervised the findings of this work. All authors discussed the results and contributed to the final artile.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.