
Abstract
Background:
Advances in three-dimensional (3D) printing technology have allowed the development of customized medical devices. Endoscopic internal drainage (EID) is a novel method to facilitate drainage of an abscess cavity into the lumen of the gastrointestinal tract by placing a double pigtail biliary stent through the fistula opening, originally designed for biliary drainage. They are available in manufacture-determined sizes and shapes. The aim of this study is to explore the feasibility of 3D printing personalized internal drainage stents for the treatment of leaks following gastrointestinal surgery over a sequential period.
Methods:
We retrospectively identified patients who underwent gastrointestinal anastomotic surgery complicated by postoperative leaks and underwent serial EID for treatment. Computerized Tomography scans were reviewed over a period of time, abscess cavity dimensions and characterizations were evaluated, and 3D reconstructions were obtained. The stents were designed, their shape and size were customized to the unique dimensions of the abscess and lumen of the patient. Stereolithography (SLA) 3D printing technique was used to produce the stents.
Results:
A total of 8 stents were produced, representing 3 patients. These stents corresponded to 2 or 3 stents per patients. Each patient underwent several endoscopic treatments, before resolution of leak.
Conclusions:
Customized stents may improve drainage of intra-abdominal abscesses after gastrointestinal surgery, if based on unique anatomy. This proof-of-concept study is a real-world application of personalized health care, which introduces the novel description of customizable 3D printed stents to manage complications following gastrointestinal surgery and may advance therapy for this complex clinical condition.
Research Ethics Committees (REC) number is A-2021-012.
Introduction
Anastomotic complications after gastrointestinal surgery can lead to prolonged hospital stay, intensive care unit admission, organ dysfunction, sepsis, and even death. 1 The management of these complications requires a multidisciplinary approach with a goal to control sepsis and improve nutritional status to promote tissue healing by means of radiographic, endoscopic, and surgical interventions.2,3 Endoscopic techniques are often the first-line therapy in gastrointestinal surgery-related complications such as leaks and fistulas. 4 Traditionally, endoscopy focused on closure of the leak opening by placing a fully covered self-expanding metal stents and/or clips. 5
In recent years, the principle of providing endoscopic internal drainage (EID) through placement of double pigtail plastic biliary stents through the fistula opening has shown efficacy. The concept of EID is to facilitate drainage of an abscess cavity into the lumen of the gastrointestinal tract and eventually closure of the fistula tract by secondary intention. Multiple reports have described effective management of acute and chronic leaks following gastrointestinal surgery using this method.6–8
The current commercially available stents are designed for biliary drainage and not for treatment of gastrointestinal leaks. We have found in our practice that some patients might benefit from asymmetric and uniquely designed stents, based on anatomy. Advances in three-dimensional (3D) printing technology may offer the flexibility to produce tailored medical products according to individualized patient needs. 9 The objective of the study is to determine the feasibility of printing customized 3D internal plastic drainage stents over time for treatment of leaks following gastrointestinal surgery.
Materials and Methods
Study design
This is a proof-of-concept study. Patients with a leak after gastrointestinal surgery who underwent EID were identified and included (Fig. 1). Computed tomography (CT) scan images were reviewed to determine volumes and shapes of the extraluminal abscess cavity as well as the gastrointestinal lumen over patients' treatment period. Based on the number of clinical evaluations, including upper endoscopy with stent management, plastic stents were designed and printed corresponding to the unique requirements at that moment in treatment. This is an ex vivo study. The stents were not implanted in patients. This study has been approved by our Institutional Review Board.

Process of 3D printing personalized double pigtail stents. Steps 2–5 were repeated as necessary throughout the treatment course of each patient. 3D, three-dimensional. Color images are available online.
Inclusion criteria
Patients older than 18 years of age who presented to our hospital from 2018 to 2021 with a leak following gastrointestinal surgery with radiological evidence of abscess formation, who underwent serial EID for treatment, and had corresponding CT imaging available.
Exclusion criteria
Patients younger than 18 years of age, patients who underwent gastrointestinal surgery complicated by a leak managed exclusively by an operation or those managed with less than two EID treatments and patients with no abscess cavity formation were excluded.
Stent design
Double pigtail plastic stents were designed using SOLIDWORKS™ software.
Stent printing
The stents were produced by 3D printing technology using Formlabs™ Form 3 printer. First, the anatomical models and custom stents were exported as Standard Triangle Language (STL) files. Second, the files were imported into a print preparation software to allow correct orientation, layout, and support to grant proper manufacturing. Then, the parts were digitally transferred to the printer to start the printing process. Stereolithography (SLA) 3D printing, also known as resin printing, was utilized. The material used to print is Draft Resin (v2)™, which prints four times faster than other standard materials.
The resin is in a liquid form, which is composed of a mixture of different monomers made of carbon atoms and a few other functional groups. These chains come together through a process called photopolymerization. In this process, energy from a beam of ultraviolet light ultimately forms polymer chains, which eventually forms the hard-plastic material for our 3D printed products. Following completion of printing, the parts were separated and light cured to achieve a solid finish. Finally, the abscess and gastrointestinal lumen were painted using an acrylic paint mixed with a surface primer.
Results
We retrospectively studied 3 patients who were treated for postoperative gastrointestinal surgery anastomotic complications at our hospital. All these patients underwent their initial surgery at an outside facility (Fig. 2). We reviewed multiple abdomen/pelvis CT scans for each patient over a period of time and evaluated the progression or resolution of the intra-abdominal abscess cavity. All these patients underwent standard of care management in our hospital using endoscopic techniques.
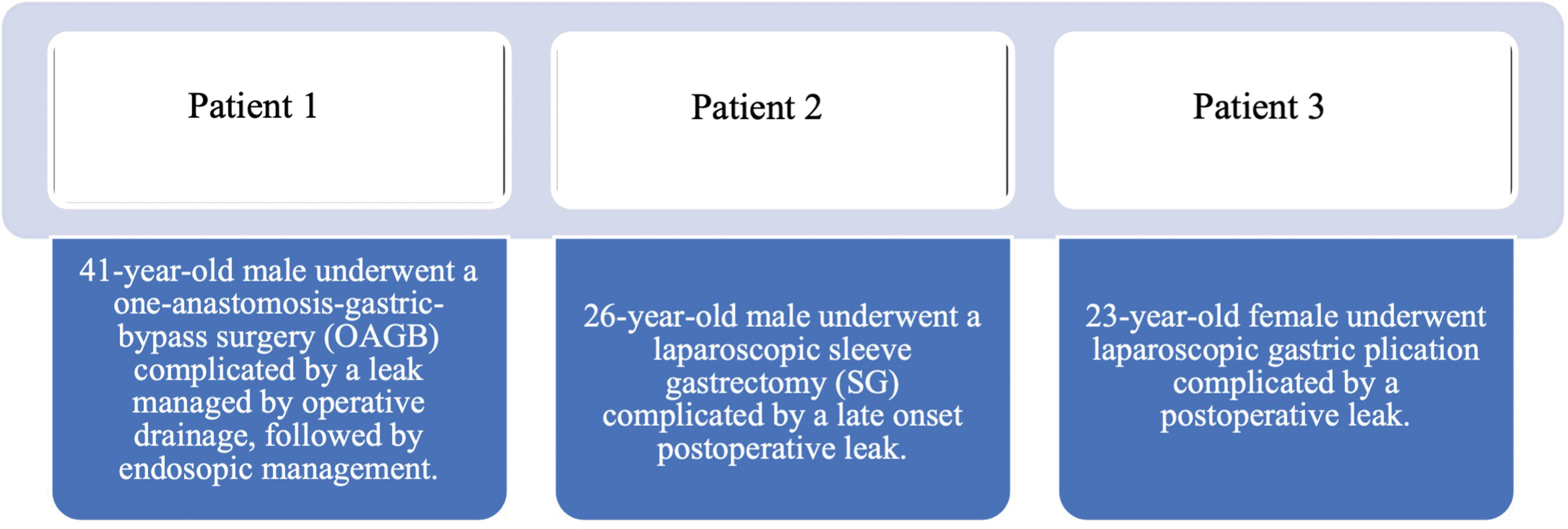
Clinical details of patients included in our study. Color images are available online.
Segmentation and 3D reconstruction
Data from CT scans, including the abscess cavity and gastrointestinal lumen, were segmented and then reconstructed to 3D images (Figs. 3 and 4). CT images were obtained by 64 and 128 detector CT. One millimeter axial images were reconstructed to 3D volumetric images. During reconstruction, the gastrointestinal lumen and abscess cavity were separated from the rest of the abdomen using Materialise Mimics software™.
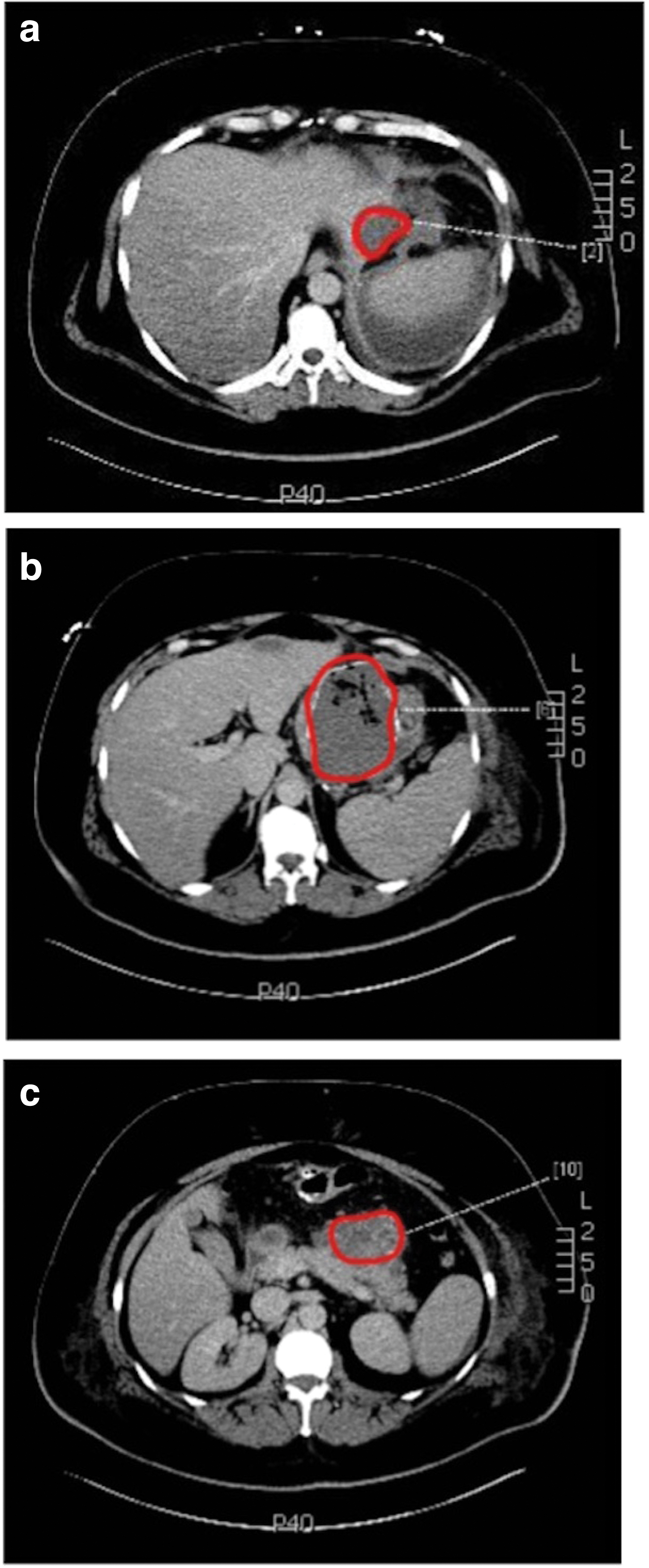

3D reconstruction of the abscess cavity from patient 1. 3D, three-dimensional. Color images are available online.
Stent design over a period of time
A double pigtail biliary stent was designed for each time interval. The shape and size of the stent was customized to each abscess cavity over time. The anatomical location of the abscess cavity and the gastric lumen as well as their size and relationship were the basis of stent design.
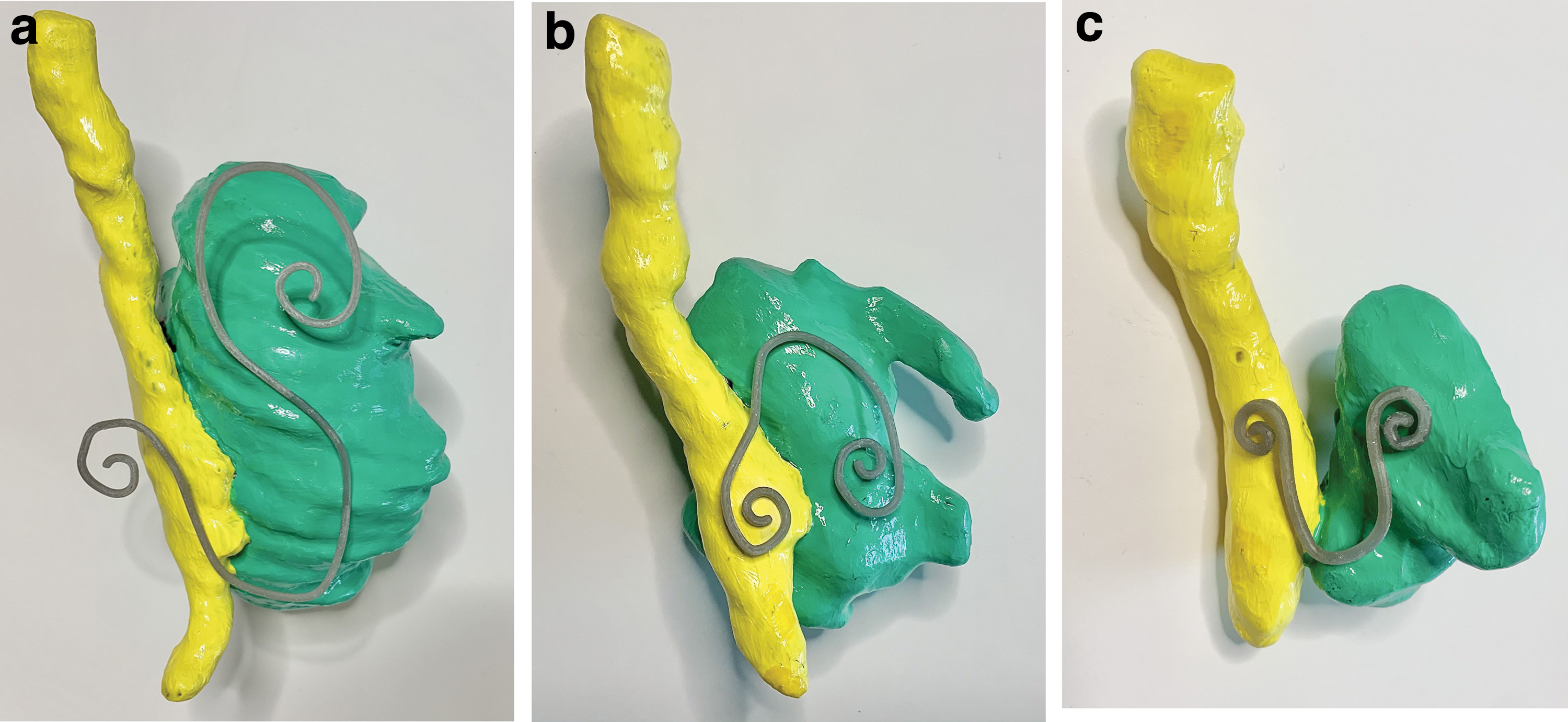
Printed stents
We printed the stents, in addition to the abscesses, and gastrointestinal lumens for illustration (Fig. 5a–c).
Discussion
Advances in therapeutic endoscopy have transformed the management of gastrointestinal wall defects from reoperating to minimally invasive endoscopic techniques. Clips and covered self-expandable metal stents (SEMS) have been widely used,10,11 however, EID is emerging as another endoscopic therapy. 8 SEMS work by sealing the anastomotic defect, diverting luminal content, and thus allowing mucosal wall healing. 12
Despite being an effective therapy for gastrointestinal leaks and fistulas, 13 SEMS has its own limitations. Related complications following stent deployment ranges between 20% and 70% in the literature with a stent-related mortality ranging from 0% to 28%.14–17 Complications include migration, hemorrhage, perforation, and stricture. 18 Specifically, stent migration is a major limitation, since it accounts for more than one third of cases needing reintervention.5,19 Those findings suggest that multiple stent deployment may be necessary to achieve clinical healing success of leaks and fistulas, thus increasing costs. 20 Patient tolerance is another limitation to wide application, as it can lead to early removal and incomplete treatment.
In 2012, Pequignot et al. 21 described for the first time the use of double pigtail biliary stents across leak orifices. The concept of EID with deployment of one or more stent is to drain any fluid collection into the gastrointestinal lumen, inducing mechanical reepithelization of the fistula tract, allowing orifice closure and early oral intake. 22 In their series, patients were treated with either SEMS or EID following a sleeve gastrectomy complicated by a gastric leak.
The authors reported better tolerability in the pigtail stents group, less procedures per patient with a shorter healing time and lower morbidity and mortality. 21 Several reports following that continued to show that EID may be more effective than placement of fully covered SEMS and clips.20,23,24 In addition, it was shown to be more cost effective.21,24 Therefore, a gradual shift in large referral centers toward EID as the preferred way to manage postbariatric surgery leaks in select patients has occurred.25–27
3D printing technology is being used in a variety of medical fields with different applications and purposes of each manufactured product. 28 Several studies have already reported 3D printing of stents customized to patient's anatomy such as utilizing airway stents in central airway obstruction, 29 biosynthetic biliary stents to relive biliary obstruction, 30 esophageal stents for inoperable esophageal cancer, 31 and endovascular stents for aortic aneurysms. 32 Despite many publications providing proof of concept studies in different medical fields, there are no studies currently evaluating 3D printed biliary stents to manage postoperative complications in gastrointestinal surgery patients.
In this proof-of-concept study, using 3D printing technology, we have successfully produced customized internal drainage stents based on patients' individual CT scans over time. The customized stents can potentially aid in better drainage of intra-abdominal abscesses with faster resolution of sepsis, and possibly a shorter recovery period. The results of our study may impact future technology that will improve patient's care in a personalized manner and potentially decrease the cost of care.
Although we have presented potential advancement in personalized health care technology, certain limitations should be noted. Our printed stents are made of a resin that is not biocompatible or implantable. In addition, the stents are not flexible. Producing flexible, hollow stents was challenging as it would require extensive support structures to keep the object from failing while printing. Improved printing materials and technology in the future will likely advance the printing process and overall manufacturing technique. Furthermore, the issue of cost is a concern when new technologies are being introduced. The production of a single stent required ∼$40 for design and $27 for printing, and around 60 minutes of time for each. With 3D printing becoming more readily available, we anticipate the costs will be lower and efficiency improved.
Conclusion
We have presented the successful reproduction of personalized, precision internal double pigtail stents through 3D printing technology. We anticipate that these customized stents will provide a framework for future applications and advancements in the field of personalized health care. Furthermore, the results of this study are relevant for designing, creating, and testing many 3D printed products besides double pigtail stents. Although our proof of concept was successfully accomplished, additional work is anticipated to produce stents that are both biocompatible and implantable, to improve production of deployable stents using the current endoscopy equipment while maintaining unique stent configuration and patency.
Footnotes
Authors' Contributions
Y.Q. carried out the implementation of the project, designed the stents, and wrote the article with support from M.K. M.A. supported project implementation and data collection. J.S.B.G., G.D.D.G., J.P.P., and R.C. provided feedback and helped edit and review the article. J.R. helped supervise the final stages of the project. N.B. did data analysis and interpretation and the software. M.K. conceived the original idea, in charge of overall direction, and planning of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.