
Abstract
Introduction:
In view of the limited availability, our study addresses the issue of optimal case selection for robotic liver surgery over standard laparoscopy offering an in-detail analysis of intra- and postoperative outcomes.
Materials and Methods:
Clinical and technical data of all consecutive cases of robotic liver surgery of a single high-volume center from 2018 to 2020 were collected prospectively. Second, we performed a retrospective analysis of all laparoscopic liver resections from 2015 to 2020. Parameters of surgical complexity were extracted and descriptive analysis and statistical hypothesis testing were performed to assess parameters of intraoperative and postoperative outcomes.
Results:
A total of 121 robotic resections were compared with 435 laparoscopic resections. Shorter robotic operating times were shown for segmentectomies of the right liver lobe compared with laparoscopic procedures (P = .003) with an according trend for extended resections. A shorter duration of applied Pringle's maneuver was observed for robotic procedures. This advantage was further enhanced in cases with close proximity of the tumor to major vessels. There were no significant differences in postoperative morbidity and mortality between both groups.
Conclusion:
Our study offers the first in-detail analysis of intraoperative and postoperative outcomes of robotic liver surgery depending on established parameters of surgical complexity. The results indicate potential technical advantages of robotic technology in liver surgery based on parameters that can be studied before the operation. When evaluating robotic technology, future studies should focus not only at overall postoperative outcomes, but rather at potential technical intraoperative advantages to allow optimal case selection for robotic liver surgery. Clinical Trial Registration Number: DRKS00017229.
Introduction
After an implementation period of more than two decades, laparoscopic liver surgery now represents the standard of care for most benign and malignant indications. With shorter operating time, lower intraoperative transfusion rate, shorter hospital stay, and reduced morbidity, benefit in perioperative outcomes has been shown for laparoscopic liver surgery compared with open liver surgery.1,2 At present, robotic liver surgery is becoming broadly available offering technical solutions to relevant drawbacks of laparoscopic surgery, that is, a stable, high-definition and 10 × magnifying camera system, imitation of the seven degrees of freedom of manual instrumentation, and improved ergonomics. 3
The availability of robotic liver surgery remains limited mainly owing to its high cost in material and staff. Our study addresses the issue of optimal case selection for robotic liver surgery. First available data describe benefits in perioperative outcome for robotic surgery compared with laparoscopy.4,5 Our study aims to zoom-in on those suggested benefits and to evaluate the technical advantages of robotic liver surgery when confronting established parameters of surgical complexity. We hereby offer the first in-detail analysis of intraoperative and postoperative outcome with the aim to characterize cases that might draw the greatest benefit from the technical advantages of robotic liver surgery.
Materials and Methods
All consecutive cases of robotic liver resections that were performed at the Department of Surgery, Campus Charité Mitte and Campus Virchow Klinikum, Charité—Universitätsmedizin Berlin, between April 2018 and December 2020, were included in our study. Clinical data were collected in a prospective design within a single-center observational study (DRKS00017229). We refer to previous publications for further information on design and data collection. 6
In a second step, baseline characteristics and clinical data on surgical complexity and postoperative outcome were retrieved retrospectively of all consecutive laparoscopic liver resections performed at our center between January 2015 and November 2020. The data were handled according to the above-cited ethical and data protection guidelines after prior approval by the institutional review board (EA2/006/16).
Approval of the local Ethics Committee was obtained (EA4/084/17) and the study was conducted in accordance with the ethical standards of the Declaration of Helsinki 1975.
Clinical parameters and classifications
Baseline characteristics were retrieved included age, sex, body mass index, preexisting medical conditions (diabetes, hypertension, liver diseases), and assessment of performance status by means of the American Society of Anesthesiologists' Physical Status Classification (ASA score).
The pathological results were determined by the senior pathologists in all cases. The histopathological classification according to Desmet et al. was used for definition and grading of liver fibrosis. 7 Clinical stages of liver cirrhosis were classified by means of the Child–Pugh Score. 8
Bile leakage was graded according to the International Study Group of Liver Surgery (ISGLS) definition. 9
Perioperative parameters
Computed tomography scan was performed for preoperative staging. Additional magnetic resonance imaging of the liver was programmed for most cases. All cases with underlying malignant disease were discussed by the interdisciplinary tumor board for hepatopancreatobiliary entities. Assignment to laparoscopic or robotic resection was based on individual decision-making between the surgeon and the patient. Furthermore, perioperative outcome parameters included duration of surgery, intraoperative need for transfusion of red blood cells, length of stay in the intensive care unit (ICU), and length of stay in the hospital.
Laparoscopic liver resection was performed as described in previous publications.10,11 Port strategies included single incision laparoscopic surgery, multi-incisional laparoscopic surgery, as well as hand-assisted laparoscopic surgery.
For robotic resections, the daVinci® Xi surgical system (Intuitive Surgical, Sunnycale, CA, USA) was used. Four robotic 8 mm trocars were inserted with two additional 12 mm and one 5 mm assist trocars. For details on the operating procedure, positioning of the patient, port placement, and setting of the robotic arms, we referred to a previous publication. 12
Intraoperative ultrasound was performed for all resections to confirm the exact tumor location, margins, and proximity to relevant structures. Before parenchymal resection, 250 mg intravenous methylprednisolone was administered. Intermittent Pringle maneuver was performed as necessary over a maximal duration of 15 minutes with a 5-minute reperfusion interval in between individual intermittent Pringle maneuvers.
For robotic resections, a modified clamp crush technique using Harmonic ACE® was applied. For all resections, relevant vessels were either clipped or transected using staplers. For laparoscopic resections, parenchymal dissection was performed using energy shears for superficial dissection (Harmonic ACE, Ethicon Inc., Somerville, NJ, USA; and THUNDERBEAT®; Olympus K.K., Tokyo, Japan) and cavitron ultrasonic surgical aspirator (CUSA®; Valleylab Boulder, CO, USA) or waterjet (ERBEJET®; Elektromedizin GmbH, Tübingen, Germany) for deeper dissection.
An abdominal drain was systematically placed in contact with the resection site and removed at 48 hours postsurgery given normal secretion. Patients with impaired liver function or after major resections received ICU surveillance.
Postoperative complications within 90 days postsurgery were documented and graded according to the Clavien–Dindo classification. 13 Severe postoperative complications were defined as a Clavien–Dindo score ≥IIIa.
Parameters of surgical complexity
Clinical and radiological parameters of surgical complexity as defined by the IWATE criteria were recorded including intrahepatic tumor location, extent of hepatic resection, and proximity to major vessels. 14 (Sub)segmentectomy, sectionectomies (right posterior and left lateral), and left and right hemihepatectomies were analyzed as categories for extent of resection.
Statistical analysis
Testing for normality was performed using the Shapiro–Wilk test. For continuous data, the Mann–Whitney U-test or Student's t-test was performed according to the normality test. Parametric data are described with mean and standard deviation (SD), and nonparametric data with median and interquartile range (IQR). For categorical variables, chi-square test was used. Differences were considered significant at P < .05. Statistical analyses were performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics
A total of 610 liver resections were performed, of which 133 were robotic and 477 were laparoscopic. Of those, 121 robotic cases and 435 laparoscopic procedures were included in our analysis (Fig. 1).
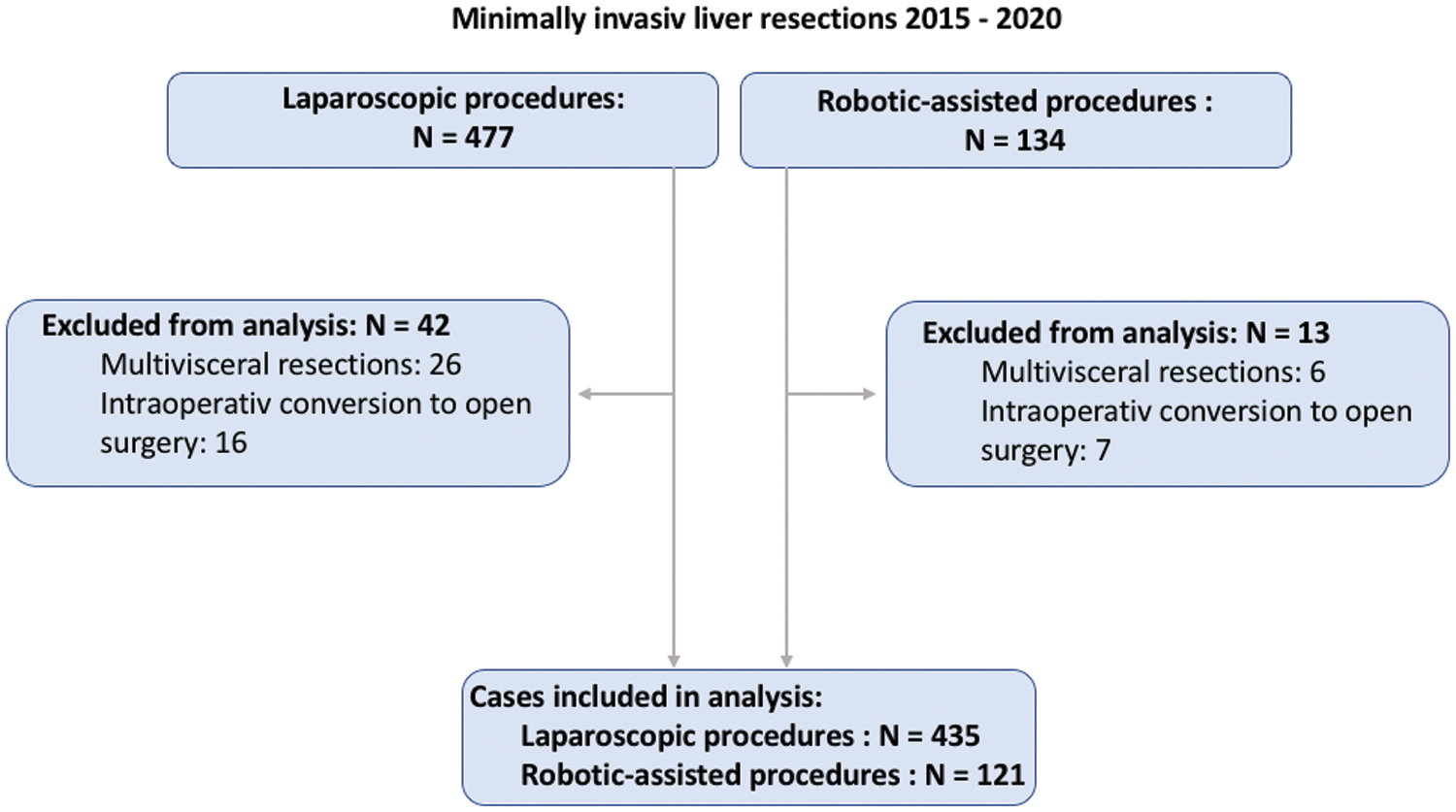
Flowchart of case numbers. Color images are available online.
No significant difference was found for age (P = .74), BMI (P = .28), and ASA score (P = .29) between the laparoscopic and robotic resection group. Malignant entities were the most common indication for liver resections (77%), with hepatocellular carcinoma (31%), colorectal metastases (27%), and intrahepatic cholangiocarcinomas (7%) representing the most frequent entities. Baseline characteristics are given in Table 1. Twenty-two percent of all cases received neoadjuvant systemic therapy. There was no difference in frequency of neoadjuvant treatment between the robotic and the laparoscopic group (P = .42).
Baseline Characteristics of Cases Included in the Analysis
ASA, American Society of Anesthesiologists' Physical Status Classification; BMI, body mass index; CRLM, colorectal liver metastasis; FNH, focal nodular hyperplasia; HCC, hepatocellular carcinoma; ICCA, intrahepatic cholangiocarcinoma; IQR, interquartile range.
Intraoperative outcomes
In a first step, the intraoperative outcomes were assessed based on the parameters “operating time,” “duration of Pringle's maneuver,” and “intraoperative blood transfusion.”
Operating time
Mean operating time was 262 minutes for the robotic group and 245 minutes for the laparoscopic group (P = .088). To further differentiate longer and shorter operating times, a stratification for the parameters of surgical complexity “Intrahepatic Tumor Location” and “proximity to Major Vessels” (as defined previously) was performed. For the evaluation of the parameter “Intrahepatic Tumor Location,” a mapping of the lesions' intrahepatic location was performed for segmental resections, sectionectomies, and hemihepatectomies, respectively.
For segmental resections, no overall difference in operating time was found between robotic and laparoscopic resections (180 minutes [IQR: 71 minutes] versus 200 minutes [IQR: 122 minutes], P = .14, for laparoscopic resections). In the next step, segmental mapping according to the tumor location was performed. A shorter operating time was found for robotic segmental resections, when the tumor is located with the right liver lobe (179 minutes [IQR: 78 minutes] versus 223 minutes [IQR: 119min], P = .003). For left-sided segmental resections, no significant difference in operating time was observed between robotic and laparoscopic resections (196 minutes [IQR: 77minutes] versus 186 minutes [IQR: 107 minutes], P = .22).
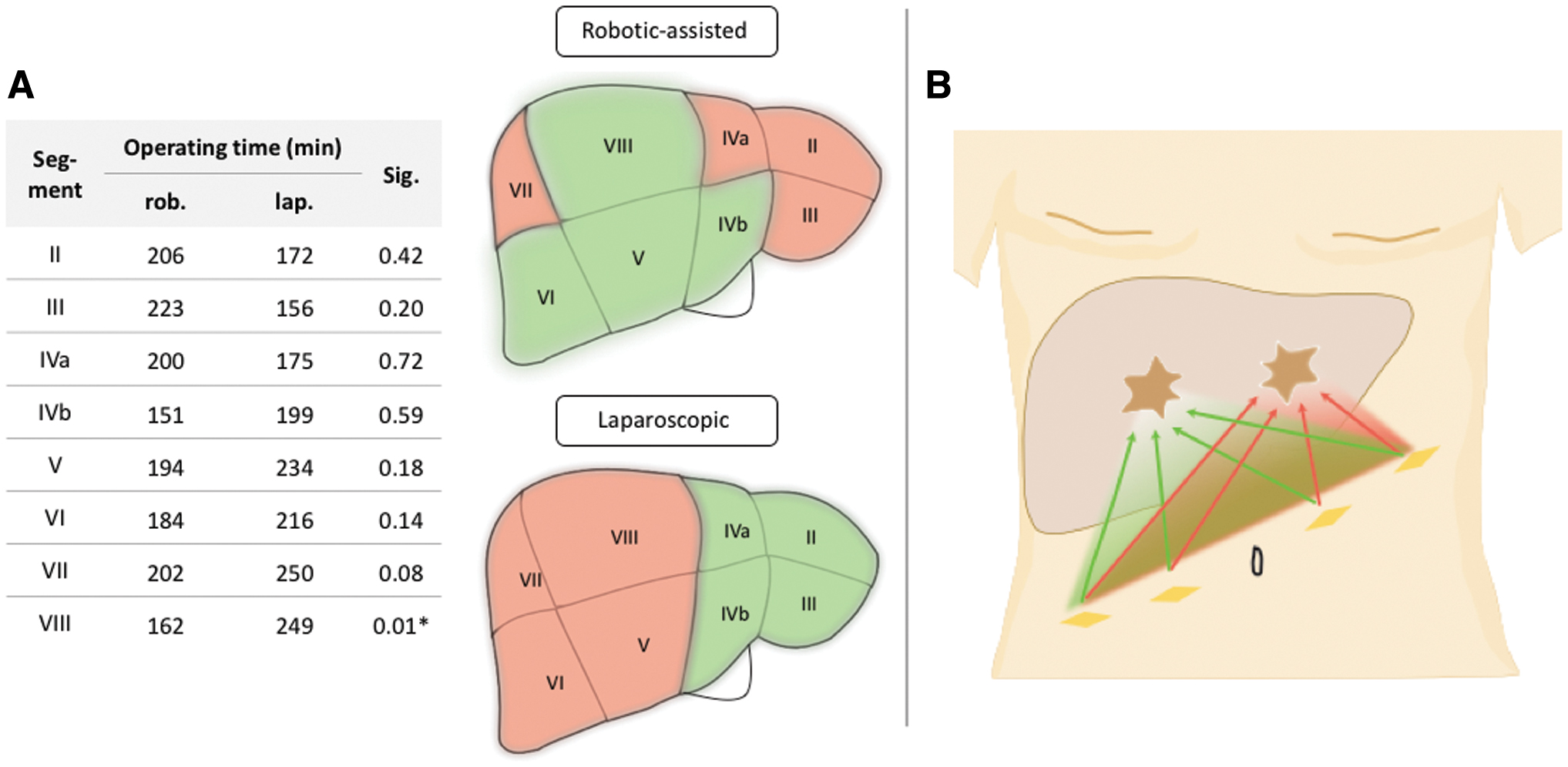
Significantly shorter operating times were noted for robotic segmental resections of segments 8 (−35%, P = .01), with according trends for segment 4b (−24%, P = .59), segment 5 (−17%, P = .18), segment 6 (−15%, P = .14), and segment 7 (−19%, P = .08), respectively. In turn, trends toward longer operating times were noted for segments 2 (+21%, P = .42) and 3 (+43%, P = .20) and 4a (+14%, P = .72), being, however, short of statistical significance (Fig. 2A). Independently from the surgical modality, resection of lesions in segment 7 was associated with longest operating times. Owing to a small case number, no evaluation for segment I was performed.
For right posterior sectionectomies, a trend toward a shorter operating time was shown for robotic procedures (240 minutes [IQR: 72 minutes] versus 267 minutes [IQR: 106 minutes], P = .35). For left-lateral sectionectomies no difference in operating time could be observed (176 minutes [IQR: 103 minutes] for robotic resections versus 175 minutes [IQR: 103 minutes], P = .76). Accordingly, a trend for shorter mean operating times was found for robotic right hemihepatectomies (326 minutes [IQR: 129 minutes] versus 350 minutes [IQR: 116 minutes], P = .17). Operating times for different extents of resection and surgical modality are shown in the Supplementary Table.
In the next step, the parameter “Distance to Major Vessels” was assessed. No correlation was found for a narrow distance between the tumor and a major vessel and the operating time for both robotic and laparoscopic resections. In cases with given proximity to a major vessel, operating time for robotic and laparoscopic resections was 310 minutes (IQR: 96 minutes) and 301 minutes (IQR: 102 minutes, P = .44), respectively.
Duration of Pringle's maneuver
A Pringle's maneuver was applied in 64 robotic and 197 laparoscopic procedures. If applied, the mean duration of the Pringle's maneuver was 21 minutes (SD: 13) for robotic and 32 minutes (SD: 23) for laparoscopic procedures (P < .001).
For the parameter “Intrahepatic Tumor Location,” lesions located in the right versus left liver lobe were compared and anterior segments were compared with the posterior segments. For all four categories, a significantly shorter Pringle's duration was found for robotic resections compared with laparoscopic resections (P < .05; Table 2). Owing to small case numbers, no evaluation of individual segments was performed.
Duration of Pringle's Maneuver Depending on the Intrahepatic Location of the Tumor
Representing statistical significance.
SD, standard deviation.
A significantly shorter Pringle's time for robotic resections compared with laparoscopic resections was found for lesions with a narrow distance to major vessels. In case of a narrow distance to a major vessel, the mean Pringle's duration was 22 minutes (SD = 16, n = 23) for robotic procedures compared with 33 minutes (SD = 23, n = 79) for laparoscopic resections (P = .016). For cases with no close proximity to a major vessel, no significant difference in Pringle's duration was found 20 minutes (SD = 11) for robotic resections compared with 25 minutes (SD = 22, P = .103) for laparoscopic resections.
Blood transfusion
Blood transfusion was necessary in 8% of cases with no differences between the robotic and the laparoscopic group (P = .73). Owing to the rare prevalence of blood transfusion, no further statistical analysis was possible.
Postoperative outcome
Mean length of hospital stay was 10.2 days (robotic group) compared with 9.5 days (laparoscopic group; P = .48). Seventy-seven percent of laparoscopic cases required postoperative ICU surveillance compared with 79% within the robotic group (P = .588). Overall, no significant differences in postoperative morbidity were seen comparing laparoscopic and robotic resections. The overall complication rate was found to be 32.2% for robotic resections and 33.8% for laparoscopic resection (P = .75). Thereby, the rate of major complications (Clavien–Dindo score ≥ IIIa) was calculated at 19.0% and 14.5%, respectively (P = .22). Overall, a tumor-free resection margin (R0) was achieved in 85% of cases. No significant difference in R0 resection rates were seen between robotic and laparoscopic resections (84.3% versus 86%, P = .22).
Intrahepatic tumor location
In a next step, we evaluated the impact of the intrahepatic tumor location on postoperative outcome. For segmentectomies, a trend toward lower complication rates was demonstrated for robotic segmentectomy of the right lobe compared with laparoscopy (5% versus 12% for laparoscopic resections, P = .15). The frequencies of postoperative complications for major and minor resections depending on the intrahepatic tumor location are given in heat maps in Figure 3.
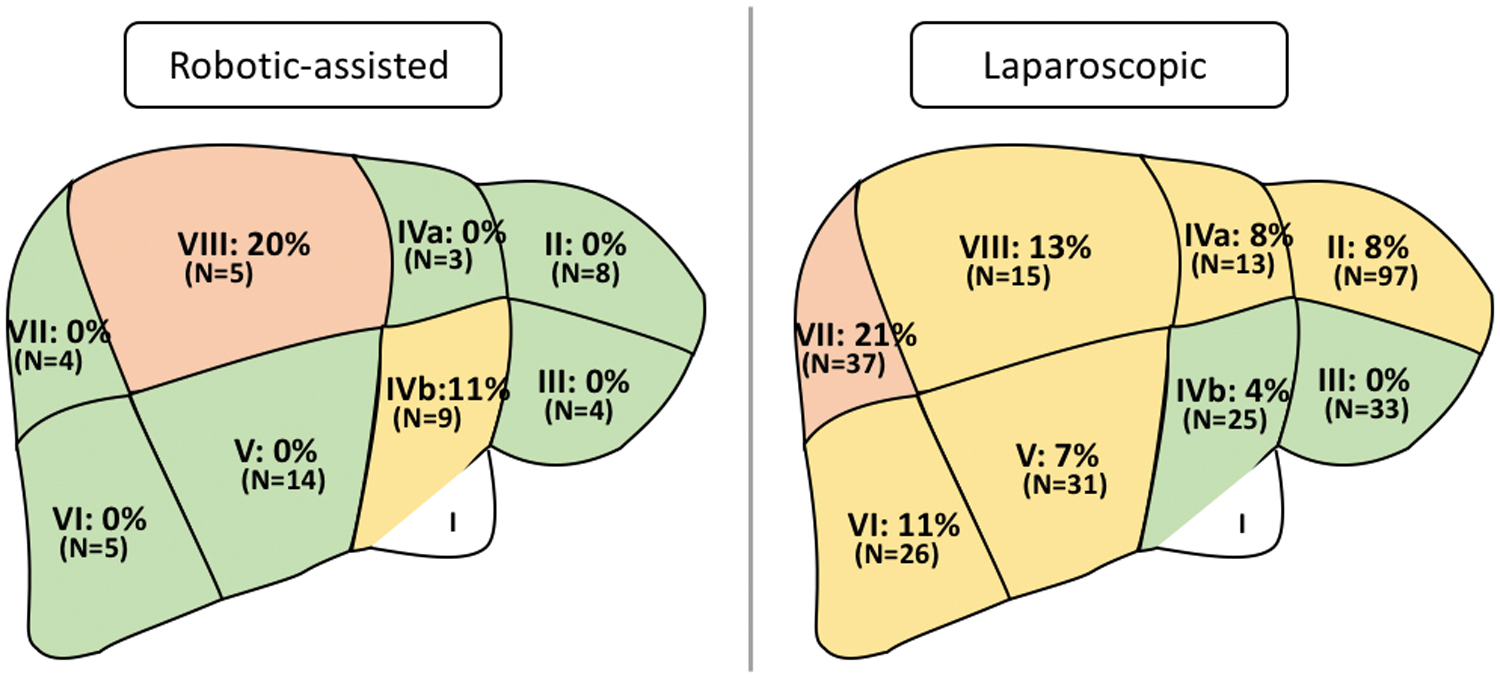
Frequencies of major postoperative complications (Clavien––Dindo classification >2) for (sub)segmentectomies depending on the intrahepatic tumor location visualized in heat maps. Color images are available online.
Furthermore, a significant correlation is found between the risk of complication and involvement of specific liver segments: Involvement of the segment 3 is associated with a significantly lower risk of postoperative complications, whereas involvement of segment 7 or 8 is associated with a higher risk of complication (P < .005 for both parameters).
Distance to major vessels
No significant distribution of postoperative complications was observed in dependence of the distance between the tumor and a major vessel. For cases with narrow distance to a major vessel, no difference in postoperative morbidity was shown (22% [n = 11] versus 19% [n = 28]; P = .54) of major complications for robotic and laparoscopic resections, respectively.
Discussion
Our analysis offers the first comprehensive evaluation of intra- and postoperative outcome of robotic liver surgery depending on operative modality and factors of surgical complexity. The results indicate potential technical advantages of robotic technology over the standard laparoscopy for procedures of the right liver lobe and in the presence of specific parameters of surgical complexity. Today, laparoscopic liver surgery represents the standard surgical technique and robotic liver surgery emerges to be broadly available.5,15 A metanalysis was able to show higher procedure-related costs for laparoscopic compared with open liver surgery and for robotic liver surgery compared with conventional laparoscopy. 16 Recent data support this finding calculating significantly higher operative costs for robotic hemihepatectomies. 17 Given the rather limited availability and significantly higher costs of robotic liver surgery, criteria for an optimal selection of the optimal surgical modality are needed. The parameters that we describe can be assessed before the surgery and therefore qualify to help in choosing the optimal surgical technique.
Our study suggests shorter operating times for right-sided, robotic segmentectomies of right-sided segments. Accordingly, a trend for shorter operating times for right-sided sectionectomies and hemihepatectomies was shown. The advantage of robotic resections within the right lobe may be explained by the range of motion and the trocar placement. Robotic procedures require the trocars to be placed in one line to guarantee maximum mobility for the robotic arms. In conventional laparoscopic procedures, trocars can be placed freely, which allows a flexible triangulation toward any defined target. Figure 2B provides the robotic trocar placement. A symmetric, optimal triangulation (represented by green arrows) is given for targets located in the right liver lobe, that is, segments 8, 6, 5, and 4b. Targets within the left liver lobe are merely reached by a less optimal triangulation (red arrows).
When visualizing the segments with the shortest robotic operating time (Fig. 2A), the map matches with the “green area” of optimal instrument triangulation. For laparoscopic procedures flexibility in trocars placement is given. Accordingly, different set-ups are used for right- versus left-sided intrahepatic locations.
Our findings for postoperative outcome match the findings on intraoperative outcome. According to the outcome for operating times, a trend toward a lower postoperative morbidity is shown for robotic segmentectomy of the right liver lobe. The same trend is observed for robotic right-sided sectionectomies and hemihepatectomies.
Furthermore, a shorter duration of the application of the Pringle's maneuver was shown for robotic resections. An advantage for cases with narrow distance to a major vessel, representing high complexity, is suggested by our data. The high range of mobility of the robotic arms can hereby be particularly beneficial. When evaluating the Pringle's duration, no additional benefit between lesions situated in the right or left liver lobe was shown.
No statistical analysis was possible for “intraoperative blood transfusion” as a parameter of intraoperative outcome. The low incidence of needed blood transfusion suggests a limited informative value of this parameter even in the setting of a large, multicenter study.
Several limitations of our study have to be discussed. The data comprises the experience of a single high-volume liver center and parts of the laparoscopic data were collected in a retrospective design. Robotic liver surgery was introduced at our center in 2018 and the potential effect of a learning curve throughout the study period was not considered. 18 Several in-detail evaluations were not possible owing to low case numbers. Thus, a multicenter approach with a prospective data collection is needed for further evaluation.
Conclusion
Our study shows that the technical applicability of robotic surgery demands an in-detail assessment beyond a mere evaluation of postoperative outcome. The data suggest that stratification for surgical complexity can help to highlight advantages of the robotic over the laparoscopic technique. To confirm the finding of our study, we propose a multicenter approach with a prospective data collection.
Footnotes
Authors' Contributions
N.N.: conceptualization, formal analysis, writing, visualization; L.F.: formal analysis, review and editing; S.K.: formal analysis, visualization; F.K.: conceptualization, writing, reviewing and editing, visualization, P.K.H.: reviewing and editing, visualization; T.M., G.L., and W.S.: conceptualization, reviewing, and editing; J.P.: conceptualization, supervision; M.S.: conceptualization, supervision, writing, review, and editing.
Disclosure Statement
J.P. reports personal fees or other support from Johnson & Johnson, Medtronic, Astellas, CHG Meridian, AFS Medical, Chiesi, Falk Foundation, Neovii, NOGGO, pharma-consult Peterson, La Fource Group, Merck and promedicis.
M.S. reports personal fees or nonfinancial support outside of the submitted work from Merck Serono GmbH, Bayer AG, ERBE Elektromedizin GmbH, Amgen Inc., Johnson & Johnson Medical GmbH, ERBE Elektromedizin GmbH, Takeda Pharmaceutical Limited, Olympus K.K., Medtronic GmbH, Intuitive Surgical Inc.
N.N., L.F., S.A.O.G., S.K., F.K., P.H., T.M., G.L., and W.S. have no conflict of interest to disclose.
Funding Information
J.P. received a research grant from Intuitive Surgical Deutschland GmbH for conducting this study (Grant number: 00017229).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.