
Abstract
Aim:
The value of intraoperative bronchoscopic inspection (IBI) for accurate confirmation of the location and distance between the distal tracheoesophageal fistula (TEF) and the proximal blind end of the esophagus (GAP) was evaluated in Type C esophageal atresia (EA)+TEF.
Methods:
IBI involved inserting the tip of a bronchoscope into the TEF and a nasogastric tube into the blind end of the EA and measuring GAP with fluoroscopy. EA+TEF patients (n = 23) treated thoracoscopically between 2007 and 2020 were classified according to IBI as IBI+ (n = 16) and IBI− (n = 7) to compare demographics, operative time, and time taken for TEF division.
Results:
Demographics were similar. Mean time for TEF division (15.4 ± 4.6 minutes for IBI+ versus 38.6 ± 20.9 minutes for IBI−; p < .05) and mean operative time (215.3 ± 48.9 minutes for IBI+ versus 286.4 ± 51.7 minutes for IBI+; p < .05) were significantly shorter. Mean GAP measured radiographically was 0.5 cm (range: 0–1.2 cm); mean GAP measured with IBI was 0.9 cm (range: 0–2.2 cm). Postoperative complications were 3 anastomotic leakages (1/16 in IBI+ and 2/7 in IBI−) that resolved without surgery and 8 strictures (3/16 in IBI+ and 5/7 in IBI−) treated by dilatation.
Conclusions:
IBI was effective for measuring GAP and is recommended for improving the efficiency of thoracoscopic repair.
Introduction
Ever since the first successful thoracoscopic repair of esophageal atresia (EA) performed in 19991 and the first thoracoscopic repair of EA with tracheoesophageal fistula (TEF), 2 thoracoscopic repair has come to be recognized as a safe and viable option for treating EA+TEF as a result of advancements in both endoscopic technology and surgical technique. Several series have evaluated thoracoscopic repair, highlighting its safety and feasibility.3–6
In an earlier published article by the authors comparing postoperative respiratory function after open and thoracoscopic repair of Type C EA, the most obvious advantage of thoracoscopic repair was that direct mechanical manipulation of the lungs was eliminated, resulting in fewer postoperative respiratory tract-related complications and smoother recovery. 7 Despite successful outcomes using thoracoscopy, all options for surgical intervention face the same hurdle at some stage, obtaining detailed information about the distal TEF and measuring the distance between the upper esophagus and the TEF (GAP). Ideally both are essential for successful surgery, but they are difficult to obtain preoperatively using radiography and are often wildly inaccurate because of angulation and stretching.
As the length of rectourethral fistulas is measured routinely during laparoscopic anorectoplasty for male imperforate anus 8 and the length of intrapancreatic common bile duct is measured routinely during laparoscopic repair for choledochal cyst, 9 the same technique was adapted for use during thoracoscopic repair for EA with TEF to measure GAP exactly between the TEF and the upper esophagus pouch.
To this end, intraoperative bronchoscopic inspection (IBI) was considered a possible solution and was evaluated in Type C EA+TEF patients undergoing thoracoscopic repair by comparing IBI results with actual intraoperative findings and assessing outcomes of surgery with respect to IBI.
Materials and Methods
For this study, the medical records of 23 consecutive Japanese neonates who underwent thoracoscopic repair of EA+TEF between 2007 and 2020 at a single institute by a single surgical team were reviewed retrospectively. In this study, all EA+TEF patients had a gastrostomy created at birth for two main reasons: to prevent inspirational pneumonia due to gastroesophageal reflux and to improve nutrition and assist growth. Not every patient will have or need a gastrostomy, but from experience, patients tend to thrive with a gastrostomy and the lungs can be protected from inspirational pneumonia.
Indications for thoracoscopic repair were weight at least 2.0 kg and absence of severe cardiac malformation or severe chromosomal aberrations. All surgeries were performed by a team of 2 board-certified pediatric surgeons (H.K. and A.Y.) with extensive technical experience and numerous publications in the literature.
The 23 EA+TEF patients were divided into two groups based on IBI: patients who had IBI were called group IBI+ (n = 16) and patients who did not have IBI were called group IBI− (n = 7). Data collected included gestational age, birth weight, age and weight at the time of thoracoscopic repair, time taken to divide the TEF, total operative time, and incidence of complications.
Measuring the distance between the proximal blind end of the esophagus and the TEF (GAP)
IBI was performed for complete evaluation of the airways, identification of the TEF and its location, evaluation of tracheomalacia, and confirming the presence of any other incidental or concomitant anatomic anomalies with a 3.1 mm flexible bronchoscope (Olympus, Tokyo Japan) under general anesthesia with spontaneous respiration. Lengths of esophageal pouches were measured once the TEF was identified, and GAP was calculated by inserting the tip of the bronchoscope into the TEF and a nasogastric tube into the blind end of the EA and measuring the distance between the two under fluoroscopic control (Fig. 1).
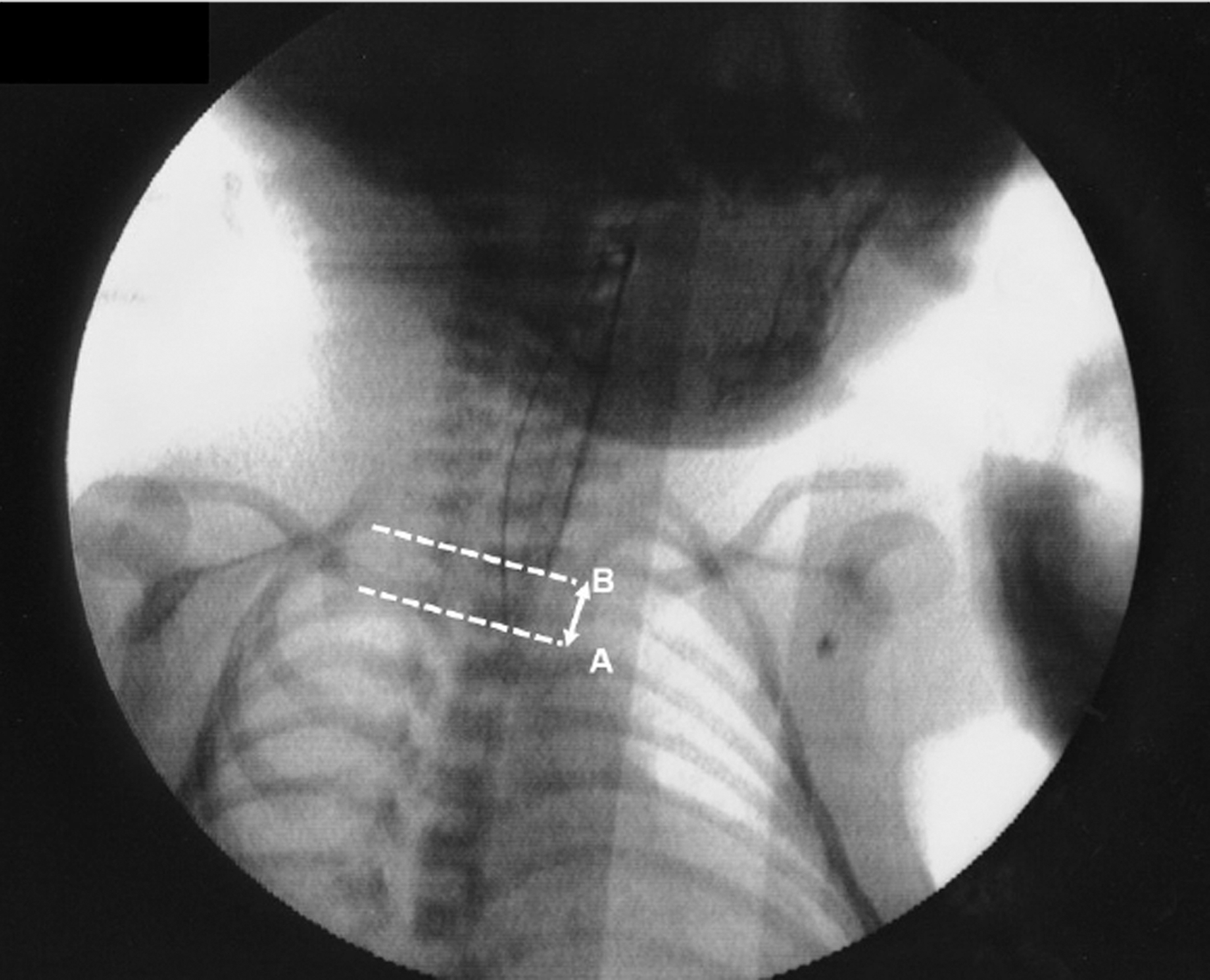
By inserting the tip of a bronchoscope into the blind end of a TEF (dotted line A: level of the tip of a bronchoscope) and a nasogastric tube into the atretic end in EA (dotted line B: level of the nasogastric tube), the distance between the two can be measured intraoperatively using fluoroscopy. EA, esophageal atresia; TEF, tracheoesophageal fistula.
Patients were intubated after evaluating the location and size of the TEF and measuring GAP. Although IBI is possible after intubation, it is not performed because the tube can cover the fistula if it is located in a high position.
Thoracoscopic repair
The thoracoscopic repair of Type C EA+TEF used in this study has been published previously by the same authors. 7 In brief, patients were placed semiprone to allow the lung to fall away from the posterior mediastinum. Initially, three trocars (3–5 mm) were inserted. Insufflation of carbon dioxide was initiated at 0.5–2 L/min to establish an intrathoracic pressure of 4–6 mmHg to cause lung collapse. The TEF was identified and ligated using a surgical endo clip (Covidien, Mansfield, MA) and divided. If the TEF could not be identified at this stage, the light source at the tip of the bronchoscope illuminated the end of the fistula, which was beneficial when a TEF was difficult to find or see, for example, if it was behind the carina (Fig. 2).
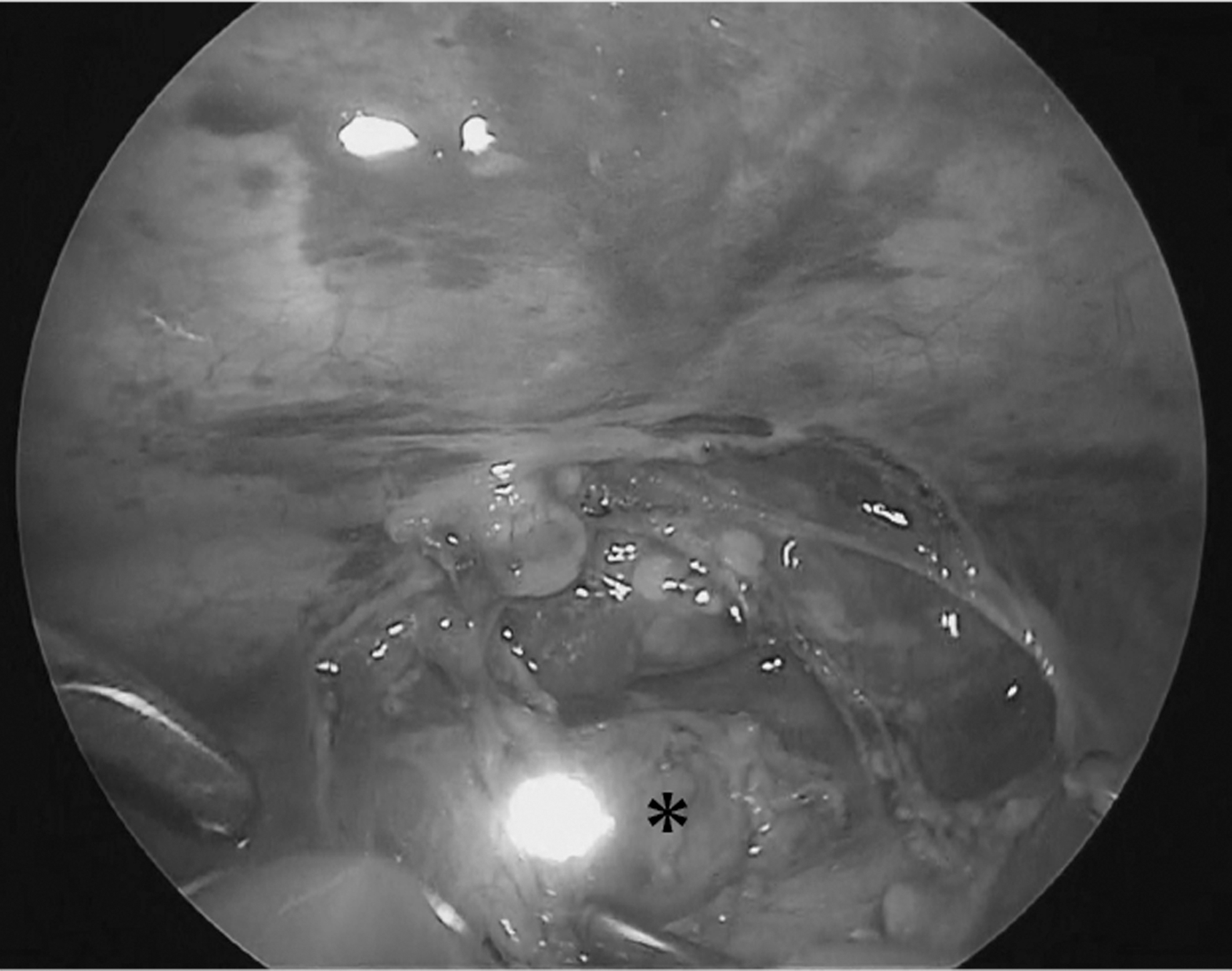
The light source of the bronchoscope indicates the exact location of the TEF (asterisk) under thoracoscopic view. TEF, tracheoesophageal fistula.
Anastomosis of the anterior part of the esophagus was then commenced with interrupted sutures. After completion of the anastomosis of the anterior part, a nasogastric tube was advanced through the proximal esophagus into the distal esophagus, and finally into the stomach. This transanastomotic tube was used routinely to relieve pressure on the anastomosis. The anastomosis of posterior part was then performed with 5/0 absorbable sutures tied extracorporeally. A chest drain was inserted under direct vision with the tip adjacent to the anastomosis.
Postoperative management
Upon completing surgery, all patients were commenced on a fentanyl infusion at 0.5–l mg/(kg·h) without muscle relaxants. Duration of use was determined by the premature infant pain profile protocol. 10 All patients remained intubated and required pressure-assisted respiratory support but use of oxygen and mechanical ventilation were minimalized, in principle. Weaning off ventilation and extubation was commenced as early as clinically possible. Chest tubes were removed after integrity of the anastomosis was confirmed with a contrast study on postoperative 7th day and a trial of swallowing was tolerated.
Statistics and approval
All data are expressed as mean ± standard deviation. The Student's t-test and chi-square test were used for statistical analysis. A P value >.05 was considered to be statistically significant. This study was approved by the Juntendo University School of Medicine Institutional Review Board (IRB number: E21-0189) and complies with the Helsinki Declaration of 1975 (revised 1983).
Results
Mean gestational age in IBI+ was 38.6 ± 1.3 weeks and that in IBI− was 38.0 ± 2.4 weeks. Seven of the 23 patients (30%) had at least one major physical anomaly: specifically 4 of 16 in IBI+ (25%) and 3 of 7 in IBI− (42%). There were no significant differences in age at the time of surgery (IBI+: 5.1 ± 1.7 days versus IBI−: 6.0 ± 3.1 days) or weight at the time of surgery (IBI+: 2.6 ± 0.4 kg versus IBI−: 2.5 ± 0.3 kg). Patient data are summarized in Tables 1 and 2.
Subject Data
Data: mean ± standard deviation.
IBI, intraoperative bronchoscopic inspection.
Comparison of Surgery with Respect to Intraoperative Bronchoscopic Inspection
Data: mean ± standard deviation.
GAP, the distance between the upper esophagus and the TEF; IBI, intraoperative bronchoscopic inspection; TEF, tracheoesophageal fistula.
Mean time taken to divide the TEF was significantly quicker in IBI+ than in IBI− (15.4 ± 4.6 minutes versus 38.6 ± 20.9 minutes, P < .05) because IBI ensured precise identification of the exact location of the TEF. For the same reason, mean total operative time was also significantly lower in IBI+ than in IBI− (215.3 ± 48.9 minutes versus 286.4 ± 51.7 minutes, P < .05). All repairs were completed successfully using thoracoscopy without conversion to open thoracotomy.
Mean GAP measured by plain chest radiography (CXR) in IBI+ was similar to that in IBI− (0.5 ± 0.3 cm [range: 0–1.2 cm] versus 0.6 ± 0.4 cm [range: 0–1.2 cm], P = .51). Interestingly, mean corresponding GAP measured using IBI was 0.9 ± 0.6 cm (range: 0–2.2 cm). IBI took a mean of 9.0 ± 3.0 minutes. GAP was longer than expected from CXR in 4 of 16 IBI+ patients, otherwise preoperative CXR estimates corresponded with IBI measurements. In 2 of 16 IBI+ patients, the tip of the tracheal intubation tube covered the TEF because it originated very proximally, and in another 2 of 16 IBI+ patients, the light source at the tip of the bronchoscope was required to find the end of the fistula.
Minor anastomotic leakage occurred in both groups: IBI + n = 1/16 (6.2%) and IBI − n = 2/7 (28.5%), P = .14. All resolved conservatively with chest tube drainage, nutritional support, and administration of antibiotics taking a mean of 5.6 ± 0.5 days. Anastomotic strictures were significantly less in IBI+ than in IBI− (3/16 [18.7%] versus 5/7 [71.4%], P = .01). All resolved by endoscopic dilatation, taking a mean of 1.3 ± 0.5 treatments (Table 3).
Comparison of Postoperative Outcomes
Data: mean ± standard deviation.
IBI, intraoperative bronchoscopic inspection.
In the 8 most recent IBI+ patients, a Fogarty catheter (4F) was used to occlude the TEF by inflating with 0.5 mL of air under direct vision until the fistula was occluded. Elective occlusion of the TEF by using a Fogarty catheter improved ventilation of the opposite lung during thoracoscopic repair.
Discussion
Bronchoscopy is a procedure commonly used for gathering information and tissue samples by biopsy or lavage from the upper respiratory tract and lungs. A recent survey by the International Pediatric Endosurgery Group found that bronchoscopy for EA was routinely undertaken by 60% of pediatric surgeons, selectively by 13%, and never by 27%. 11 Another survey by the European Pediatric Surgeon Association found that 56% do not perform routine preoperative bronchoscopy. 12 However, these surveys did not specifically distinguish when bronchoscopy was performed.
Procedural diagnostic bronchoscopy and preoperative bronchoscopy have different purposes. Lal et al. reported that 66% of their 396 patients underwent preoperative bronchoscopy and they found it particularly useful for identifying multiple fistulae in 3 patients and laryngotracheal clefts in 2 patients and used it intraoperatively as well to occlude a fistula distally when required. 13
In this study, bronchoscopy was used in a novel way to confirm the status of EA+TEF so repair could proceed smoothly. The most obvious advantage of IBI was determining the exact location of a TEF and to measure GAP (the distance between the TEF and upper esophagus pouch) accurately, both facilitating repair immensely as reflected by significantly quicker operative times documented in this study. Surprisingly, GAP measured by IBI was much longer than expected from preoperative CXR in 25% of patients and this was particularly evident when the TEF was located at the carina.
If the distal end of a TEF enters at the carina, it is likely that the distance between the two pouches is greater, especially if the upper pouch does not extend into the mediastinum very far. Another advantage of IBI was the ability to find a TEF promptly and determine the extent of dissection required. The light source at the tip of a bronchoscope was put to practical use to indicate where to dissect behind the carina when the operative field viewed through the thoracoscope was limited, and if a TEF enters mid-trachea, GAP would be expected to be smaller, requiring minimal dissection. During dissection of a TEF during thoracoscopic repair, there is potential for over aggressive/extensive dissection.
By allowing precise identification and guided dissection, IBI would also have potential for preventing postoperative anastomosis leakage because of over aggressive/extensive dissection that could compromise vascular perfusion that hinders tissue recovery and avoid postoperative tracheomalacia and chylothorax due to minimal dissection.
Another advantage of IBI was early TEF control. By ligating the TEF, shunting can be prevented. Uncontrolled shunting may result in hypercapnia and gastric distention. Addition of Fogarty placement would add minimal time to the operating procedure. Our data suggest that the addition of both bronchoscopy and Fogarty placement would extend total operating times for only as little as 10 minutes, which may arguably be regained in some patients with increased security that occlusion of the fistula provides.
The complication rate in this study was better in IBI+ than generally reported in the literature; in particular, anastomotic leakage, reported to range from 8% to 20% in experienced hands,4,14–16 was 6.2% in IBI+. In IBI−, leakage rates were typical of reported rates in the literature at 28.5%. Although the incidence of anastomotic leakage was less, the difference was small at 1.8% and could in fact be due to sampling bias because the number of patients in this series is small.
However, less manipulation of tissues during thoracoscopy equates with less traumatic repair compared with open surgery and IBI could improve the focus of surgical intervention to contribute to decreasing anastomotic leakage, anastomotic stenosis, and scar/adhesion formation. Larger series will confirm the specific impact of IBI on complications, and larger longer studies are underway.
This study has limitations. The small sample size prevents the actual value of IBI from being appreciated fully and being retrospective, more recent results might not be included and be the cause of selection bias. For these reasons, this study of the value of IBI is presented as a preliminary study as clinically relevant trends were noted and considered worthy of reporting. Longer term outcomes of the patients in this study assessed through at a longitudinal multidisciplinary clinic will also enable quality of life to be assessed in relation to IBI.
The learning curve for EA+TEF repair is steep because it is a rare condition everywhere and many pediatric surgeons consider thoracoscopic repair of EA+TEF far too technically challenging to perform routinely despite growing interest in the procedure. Experienced surgeons should be able to adapt their skills to overcome any lack of confidence once the anatomy is obvious. The surgical maneuvers and tasks involved in EA+TEF repair are not unique, although anyone attempting thoracoscopic EA+TEF repair must have mastered minimally invasive surgical techniques in neonates.
IBI described in this preliminary study represents an innovative application of existing technology for improving the thoracoscopic repair of EA+TEF without involving complicated concepts. In fact, when an EA+TEF patient has a gastrostomy tube, a flexible bronchoscope could even be inserted through the gastrostomy and advanced retrogradely to identify/examine a TEF without involving the airway. A study is planned to assess this potential application of IBI.
In conclusion, for EA+TEF patients, IBI has potential for identifying the location and size of a TEF; however, in the absence of standard guidelines for its use during routine anesthesia or surgery for EA+TEF, IBI could be considered somewhat controversial. Nevertheless, enhanced confidence will improve learning curves and IBI would be particularly appreciated by less experienced surgeons.
Footnotes
Authors' Contributions
H.K. and A.Y. designed the study. H.K., G.M., T.O., S.S., Y.M., Y.Y., K.K., K.N., and A.Y. were involved in clinical treatment. H.K., T.O., and Y.M. collected and analyzed data. H.K. and G.J.L. prepared and revised the article. All authors have read and approved the final article.
Disclosure Statement
The authors declare that their research was conducted in the absence of any commercial financial relationships that could be construed as potential conflicts of interest. No competing financial interests exist.
Funding Information
The authors have not declared a specific grant for this research from any funding agency in the public or commercial.