
Abstract
Introduction:
Concomitant gallstones and common bile duct (CBD) stones is a common problem, and there is still no consensus on the best approach in the management. Options include preoperative endoscopic retrograde cholangiopancreatography (ERCP), Laparoscopic cholecystectomy (LC) with CBD exploration, and LC with postoperative ERCP. Each option has its own limitations and complications. In this article, we assessed the feasibility of laparoscopic surgical clearance of the CBD after a failed ERCP, reasons for failure of endoscopic clearance in our cohort. We will discuss the management options after ERCP failure, the challenges, and the outcomes.
Materials and Methods:
We retrospectively reviewed all the cases of laparoscopic common bile duct exploration (LCBDE) performed in our hospital between April 2006 and January 2019. Two hundred cases were performed, 178 cases as a primary procedure while 22 were performed as a secondary procedure after failed ERCP. We have previously published data on the case series (PMID 33140155) and here explored the cases performed after failed ERCP as a secondary procedure. We analyzed demographics of patients, preoperative investigations, ERCP trials, and reasons for ERCP failure, operative approach, duration of operation, conversion rate, complications, and outcomes.
Results:
Twenty-two patients underwent a laparoscopic CBD clearance after failed ERCP. Sixteen of these were in the first 5 years of the study. Multiple attempts of ERCP were made in 7 patients (31.8%) and a single attempt in 15 patients. In 8 patients (32%), the duct was not accessible (failed cannulation) due to a variety of reasons. Nine patients had impacted stones larger than 1 cm, 4 patients had Mirrizi syndrome with concomitant large CBD stones, and 1 patient failed endoscopic clearance because of the large number of stones in the CBD. CBD clearance was successful in 19 patients (88%), 8 were completed by a transcystic approach and 14 by a transcholedochal approach. Postoperative length of stay was 12 (+10) days. One patient had an unplanned readmission within 30 days. One patient required reoperation for bleeding. Three patients developed recurrent stones and 1 developed a subsequent stricture. No mortalities were recorded.
Conclusion:
LCBDE is feasible and appears safe as a secondary procedure after failed ERCP. The new technologies and the advancement of surgical techniques will continue to improve success and reduce morbidity.
Introduction
Common bile duct (CBD) stones are found in up to 20% of patients with symptomatic gallstones. 1 Management of these stones varies, with no consensus on the best approach. Options include laparoscopic cholecystectomy (LC) and pre-, post-, or intraoperative endoscopic retrograde cholangiopancreatography (ERCP); surgical approaches (Laparoscopic and Open) to the bile duct; and more recently, percutaneous, combined percutaneous, and endoscopic approach, and SpyGlass (cholangioscopy) are also available, although usually used as a secondary or a rare alternative option.
Several reports have indicated high technical success rates with extraction of at least 90% of stones endoscopically (ERCP).2,3 Recent meta-analysis showed that the two-stage approach (ERCP followed by LC) is associated with a higher CBD stone clearance rate, lower postoperative bile leakage rate, and higher rate of pancreatitis; while the single-stage laparoscopic approach may shorten hospital stay. 4 Laparoscopic CBD exploration (LCBDE) can be performed either as the primary procedure or as a secondary procedure after failed ERCP.
The reasons behind ERCP failure include inability to cannulate the CBD, previous operations, presence of periampullary or duodenal diverticulum, inability to clear the stones (very large stones or impaction), or due to the large number of stones present.
The aim of the study is to investigate the reasons behind ERCP failures, the decision-making process regarding the chosen operative options following ERCP failure, revisit specific challenges, and how to improve outcomes in these cases.
Materials and Methods
We retrospectively interrogated a prospectively collected database of all the patients who underwent LC and CBD exploration (April 2006–January 2019). Two hundred cases were performed, 178 cases as a primary procedure while 22 were performed as a secondary procedure after failed ERCP. We have previously published data on the case series (reference), and here explore the cases performed after failed ERCP. These cases were performed by 4 different Upper Gastrointestinal (GI) surgeons at our district general hospital as a secondary procedure after ERCP failure. A new database was created and populated by this cohort, including demographics, clinicopathological data, including preoperative liver function tests (LFTs), preoperative imaging modalities, preoperative CBD diameter, number and size of stones (or largest stone if multiple present), date of preoperative ERCP, reason for ERCP failure, number of ERCP attempts, duration between the failed ERCP and surgery, intraoperative details, and outcomes.
The primary endpoint for this observational study was a successful CBD clearance, the secondary endpoints included operative time, t-tube placement, retained and/or recurrent stones, postoperative length of stay, need for reoperation, 30-day readmission, CBD stricture formation, and mortality.
All operations were carried out by consultant upper gastrointestinal surgeons with a standard four-port approach for LC. We aim first for laparoscopic approach with all the cases except if there is an absolute contraindication for this approach. CBD access approach was decided on based specifics of the case, that is, reason(s) for endoscopic failure, size and number of the stones, anatomy and feasibility of transcystic approach, expertise, and technology availability. The transcystic approach was preferred if feasible, with the transcholedochal approach used as a rescue procedure. Three and 5 mm choledochoscopes were used for exploration of the CBD and confirmation of clearance. Baskets, direct extraction using forceps, flushing with saline, and balloon catheter techniques were used to clear the CBD.
Definitions
The CBD diameter was reported by a GI radiologist on preoperative magnetic resonance cholangiopancreatography (MRCP). Operative time was the interval between the initial skin incision and skin closure. If at the end of the operation all stones were not cleared from CBD, this was considered a failure. If a stone was diagnosed unexpectedly within 6 months from the time of the operation on follow-up imaging due to abnormal LFTs, this was considered a retained stone. A recurrent stone was defined as a stone discovered more than 6 months from the date of the primary operation.5,6 Length of stay was defined as the number of postoperative days in hospital. Readmission was defined as admission within 30 days of discharge.
Statistical analysis
Quantitative variables are presented as mean + standard deviation. Qualitative variables were presented as absolute value and percentage.
Results
During the period 2006–2019, a total of 200 LC with CBD exploration were performed in our hospital. Twenty-two cases (11%) were performed as a secondary operation after a failed CBD clearance endoscopically. The mean age was 55.6 years (±13.0) and 14 patients (63.6%) were female (Table 1). Sixteen cases were performed before 2013 and only 6 performed after 2013. There were two ERCP attempts in 7 patients (31.8%) and a single attempt in the remaining 15 patients (Table 2). The reason for ERCP failure was either due to failure to cannulate (8 cases) or failure to clear the CBD (14 cases). The cause of failure to cannulate the CBD during ERCP in this cohort was the presence of a duodenal diverticulum, with the most common cause for failure to clear the CBD being a large, impacted stone.
Demographic and Preoperative Data
Data expressed as mean (±SD) or absolute value and percentage.
ALP, alkaline phosphatase; ALT, alanine transaminase; CBD, common bile duct; CBDE, common bile duct exploration; CT, computerized tomography; ERCP, endoscopic retrograde cholangiopancreatography; LFTs, liver function tests; MRCP, magnetic resonance cholangiopancreatography; SD, standard deviation; US, ultrasound.
Failed Endoscopic Retrograde Cholangiopancreatography Data
Data expressed as mean (±SD) or absolute value and percentage.
CBDE, common bile duct exploration; ERCP, endoscopic retrograde cholangiopancreatography; SD, standard deviation.
None of the 22 patients had previous surgery that would preclude standard ERCP (Roux-en-Y or Billroth II) as all those patients proceeded to LC + LCBDE directly as a primary operation and are therefore not discussed in this article. One of our patients in this cohort previously had a LC and was therefore excluded from subsequent analysis.
CBD clearance was initially attempted by transcystic approach in 9 patients (42.8%) and transcholedochal in the remainder. A direct transcholedochal approach was taken in large stones or at a difficult location. Two cases were converted from transcystic to transcholedochal explorations due to either equipment failure or unfavorable anatomy. Fourteen patients had an intraoperative cholangiogram before proceeding to CBD exploration. An on table cholangiogram was not performed when the cystic duct could not be safely identified or Mirizzi Syndrome was present. The average preoperative CBD diameter was around 10 mm. The bile duct was repaired over a T-tube in 6 patients that had a transcholedochal approach. Average duration of operation was 210 (±68) minutes.
Clearance was successfully achieved in 19 patients (90.5%). This was achieved by open operation (conversion to Kocher incision) in 6 cases (28.5%). Indications for conversion to an open operation were impacted stones at the ampulla, unclear or unfavorable anatomy, and equipment failure.
The 3 patients who failed operative CBD clearance were referred to tertiary hepatopancreaticobiliary (HPB) centers and managed with SpyGlass cholangioscopy. Two cases had large stones at ERCP, the other a duodenal diverticulum which negated cannulation. Irrigation failed during operative CBD clearance in one case, an impacted stone at cystic duct/CHD junction was unable to be dislodged in a second, and the third thought to be clear at the end of the case on both cholangiogram and cholangioscopy. Two of these patients were explored by laparoscopic approach without conversion to open operation, the decision was made by the responsible operating surgeon depending on clinical judgment, patient factors, logistics, and the availability and feasibility of alternatives.
The mean postoperative hospital stay was 11.5 (±9.6) days (Table 3). One patient returned to theater due to bleeding. One patient was readmitted within 30 days of discharge with a wound infection and retained stone.
Outcome Data
Data expressed as absolute value and percentage or mean (±SD).
Retained stones were diagnosed unexpectedly postoperatively either on a follow-up imaging or ongoing LFTs abnormalities.
Recurrent stones were defined as a stone discovered more than 6 months from the date of the primary operation, these were discovered more than 2 years postoperatively.
Length of stay defined as the number of postoperative days patients stayed in hospital.
CBD, common bile duct; CBDE, common bile duct exploration; ERCP, endoscopic retrograde cholangiopancreatography; LFTs, liver function tests; SD, standard deviation.
No retained stones were noted. Three patients required postoperative ERCP. Two patients (9.5%) developed a recurrent stone; one after 7 months and the other after 2 years. Both recurrent stones were managed successfully by ERCP. One patient developed a CBD stricture that subsequently required a reconstruction in our tertiary HPB center following Mirrizi syndrome and a concomitant large CBD stone.
The median follow-up was 80 months. No mortality was reported.
Discussion
The options for management of CBD stones include LC with pre-, post-, and intraoperative ERCP or single-stage approach LC with LCBDE. The management of CBD stones is still incredibly challenging in some cases, despite advances in technologies, training, and expertise, with a chance of failure in all approaches.
LCBDE can be performed as a primary procedure or secondary after failed ERCP. Overall failure rate to clear the CBD at ERCP is 10%–15%, regardless of the reason for failure. 7 Postprocedural ERCP-related complications occurred in (8.0%) patients with difficult bile duct stones, in comparison to less than 5% in relatively easy nonchallenging CBD stones cases. 8 Therefore, patient selection and early referral of those who are considered very high risk of failure of endoscopic treatment is crucial. There is also evidence that the complication rate increases after multiple ERCP trials.9,10
From our data, it was clear that the number of LCBDE performed per year, increased since our first case in 2006. At the same time, there was a decrease in the number of failed ERCP, which required surgical intervention. This may be due to an increased experience of our ERCP endoscopists, or advances in ERCP technique.
From the same data collection period, there was no single case of cholecystectomy and CBD exploration performed in an open approach as a primary procedure, this only occurred after failed laparoscopic approach.
We believe that the reduction in the number of cases that required surgical intervention after failed ERCP in this cohort could be attributed to the multidisciplinary team approach in managing choledocholithiasis. This leads to appropriate case selection and an individualized management approach. In our series, the majority (16 cases) were performed in the first 5 years of this study period and significantly decreased after, as only 6 cases subsequently failed ERCP clearance and required surgical intervention. Therefore, most of these particularly challenging and difficult cases are managed while we are in the early stages of our learning curve in bile duct exploration laparoscopically, which will have affected outcomes.
The success rate of biliary cannulation at ERCP is 84%–94% even in expert hands.11,12 This can be as low as 78% in cases of duodenal diverticulum and 38% if the ampulla is located at the bottom of a diverticulum.13,14 This is mirrored in our series, with a failed cannulation, the cause of failure to clear the CBD at ERCP in 8 of 22 (36%) cases.
The average duration between ERCP attempts was 15.9 (+13.0) weeks, a little outside the recommended 3 months by the European Society of Gastrointestinal Endoscopy (ESGE). 15
The need for imaging between failed ERCP and surgery also requires contemplation. In our series, 9 patients (41%) had a MRCP between the last ERCP failed attempt and the operation. There are no current guidelines for interval imaging. The ability to perform on table cholangiogram and/or intraoperative ultrasound may override the need for routine preoperative imaging except in occasional cases, for example, previous cholecystectomy. In this situation, the indication for surgery is the CBD stones not the gallbladder, avoiding exposure of the patient to an unnecessary operation with high conversion rate if the CBD is clear of stones.
In the literature, the most common cause for failure of clearance after ERCP was missed stones, in around 80% of cases, this would mandate CBD imaging preoperatively or intraoperatively for all patients who have had an attempt at endoscopic clearance of the CBD irrespective of the duration between the two procedures. 16 We would also recommend further preoperative imaging if a worsening of LFTs occurred during the interval between procedures.
The mean duration between the last failed ERCP trial and the operation was 16.5 (±15.8) weeks. This is well outside the ESGE recommendation of 2 weeks for patients treated for choledocholithiasis to reduce the risk of conversion rate and risk of recurrent biliary events. 15 Investigations into the time interval between ERCP and LC have shown outcomes suggesting that early LC (within 72 hours) appears to be safe and might prevent the majority of biliary events in the period following sphincterotomy17,18 and which is also relevant when performing LCBDE after failed ERCP. There is currently no recommendation if the ERCP was unsuccessful, but the risk reduction benefits from early intervention (<2 weeks) would also apply in these cases. Timings are important when considering the urgency of CBD clearance, as indications of pancreatitis and cholangitis require timely intervention.
Bridging maneuvers and stenting can be used while deciding on the best management approach. The combination of stent placement and oral administration of ursodeoxycholic acid can result in disintegration of the CBD stones, 19 but there is no data on its role after bile duct clearance. Long-term stenting of the bile duct for choledocholithiasis is not recommended for most patients due to high rates of morbidity and mortality, often related to sepsis. 20
Several studies have observed that after biliary stenting for 3–6 months, a significant proportion of large CBD stones disintegrated, decreased in size, or even disappeared.21–26 These effects of biliary stenting, which we have also seen, can serve as an adjuvant measure to finally clear initially deemed “unextractable” CBD stones.
Transcholedochal stone clearance rate after ERCP failure in the literature is 62.5%–100%,27–30 including 95.7% when performed after ERCP failure in nondilated CBD 29 and 83.3% for impacted stones. 28 This fits with our rate of 90.5%.
Clearance of CBD stones surgically after failed ERCP required special consideration of certain important factors, not necessarily relevant when performed as a primary procedure. The approach to the duct needs to be tailored to the reason for failure. Where failure was due to failed cannulation, we may still approach the CBD via a transcystic route; if the stones are small, with minimal duct dilation. If the stones are large and impacted, a transcholedochal route would be necessitated. Recent use of the electrohydraulic and laser lithotripsy as adjunct in managing the large stones may increase the feasibility of a transcystic approach, even in the cases of large stones. Shim 31 and Swahn et al. 32 have shown their use to markedly increase stone clearance rate. The number of stones also factors into deciding the approach, as the transcholedochal approach is preferred in cases with a multitude of stones.
The diameter of the CBD is the most important factor in deciding the approach to the bile duct. The smallest safe diameter of transcholedochal CBD exploration remains controversial, our institution uses a cutoff of ≥10mm, however, are aware that specialist HPB surgeons explore ≥8mm bile ducts transcholedochally.
Another consideration is to plan operative strategy, if unable (like us in 6 cases) to clear the CBD laparoscopically. Your plan will depend on patient factors, anatomy on preoperative imaging, reason for ERCP failure, and the availability of other expertise and techniques of CBD clearance before converting to open operation, either locally or farther afield. Conversion rate to open surgery is higher after failed ERCP compared to primary LCBDE. Impacted CBD stones, dense gallbladder adhesions, and previous upper abdominal surgery often increases the trend toward conversion to an open procedure during LCBDE.33,34
The complication rate increases dramatically when dealing with difficult CBD stones endoscopically, and much research has concentrated on finding the factors to predict those difficult cases. In a retrospective study to evaluate factors significantly contributing to a failed ERCP, Christoforidis et al. proposed criteria potentially contributing to the difficulty of endoscopic clearance of the CBD. 8 These factors include anatomic variations and alterations due to diverticulum or previous operations, stone factors (size >15 mm or >4 stones), acute distal duct angulation, and age >85 years.
However, their multivariate analysis showed only age ≥85 years, more than four stones and CBD stone diameter ≥15 mm were independent contributors to the failure of CBD stone removal. Kim et al. prospectively showed that large CBD stones (>15 mm), impacted CBD stones, a shorter length of distal CBD (<36 mm), and more acute distal CBD angulation were significant factors affecting the technical difficulty of CBD stone clearance. 35
Repairing the choledochotomy over a t-tube is a controversial issue. In primary LCBDE, there is a growing trend and strong evidence base toward avoiding them, to prevent the associated morbidity, with minimal benefits. The comprehensive metanalysis by Podda et al. showed that primary repair of the CBD is safe, feasible, and associated with less complications compared to repair over t-tube. 36 However, in secondary cases after ERCP failure, especially if due to failure to cannulate, t-tube insertion allows ongoing access to the biliary tree if further postoperative interventions are required. This is especially useful if there is any doubt about whether complete clearance of the CBD has been achieved. In this series, the CBD was repaired over a t-tube in 6 cases, where there was a doubt over complete clearance.
We believe the ability to manage most CBD stones with a transcystic approach will shift the pendulum toward this approach to become the standard of care and the first modality of choice in most centers.
In recent years, the single-stage approach for managing the CBD stones has becoming more popular especially with developments in laparoscopic technologies and advanced laparoscopic training. The literature shows that a single-stage surgical approach is associated with a shorter hospital stay and comparable efficacy. 37 Moreover, it may show superior results in terms of perioperative safety and short- and long-term postoperative efficacy compared with ERCP. 38 However, we wish to emphasize that none of those different modalities or approaches should replace others entirely. We believe the combination of options complement each other and we should use a multidisciplinary approach to managing patients with choledocholithiasis. We proposed two algorithms to assist in formulating a management plan for patients who have failed ERCP clearance of CBD stones (Figs. 1 and 2).
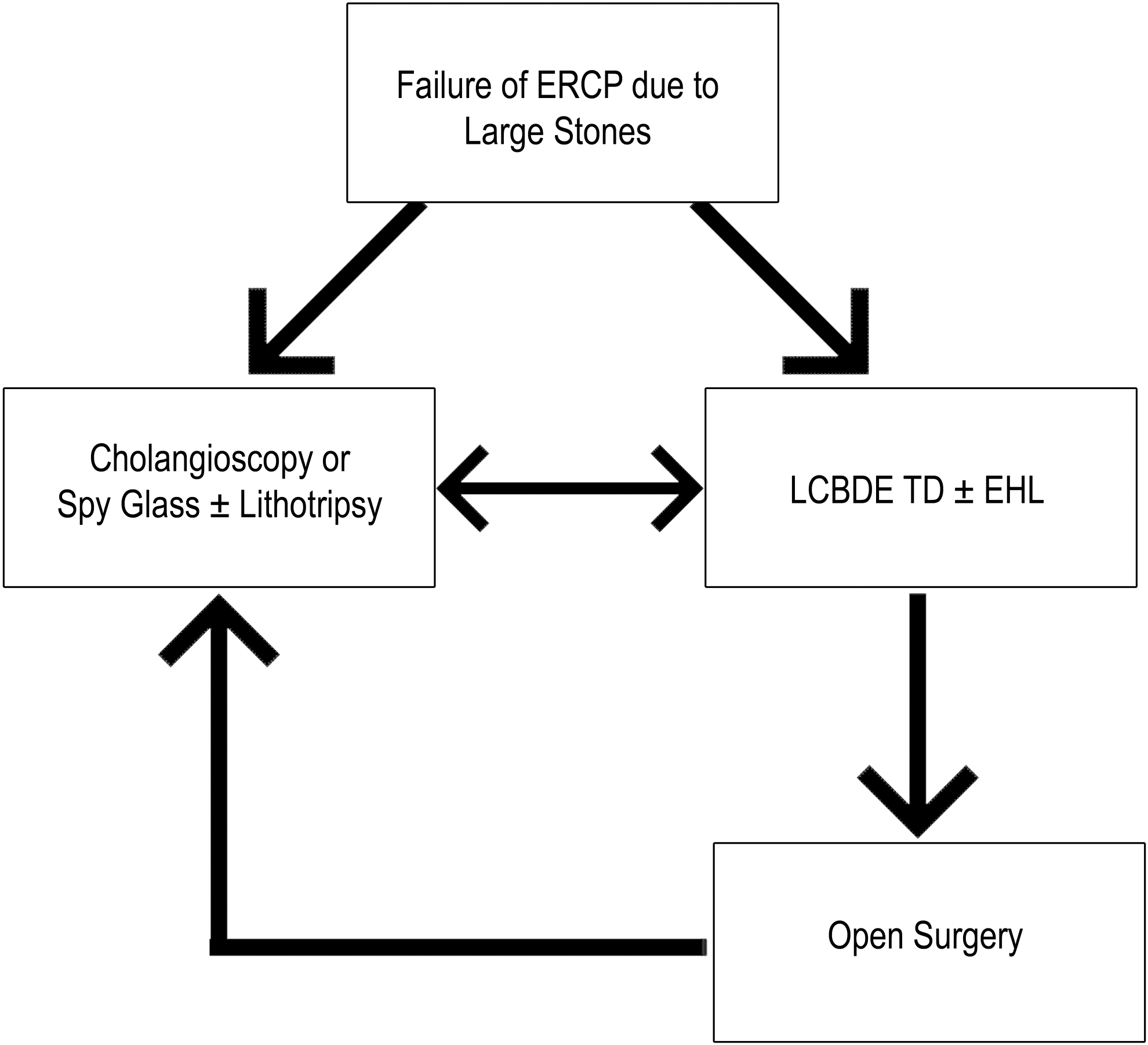
Management algorithm 1. CBD, common bile duct; CBDE, common bile duct exploration; EHL, electrohydraulic lithotripsy; ERCP, endoscopic retrograde cholangiopancreatography; LCBDE, laparoscopic common bile duct exploration; TD, transcholedochal approach to CBD.

Management algorithm 2. CBD, common bile duct; CBDE, common bile duct exploration; EHL, electrohydraulic lithotripsy; ERCP, endoscopic retrograde cholangiopancreatography; LCBDE, laparoscopic common bile duct exploration; PTC, percutaneous transhepatic cholangiography; TC, transcystic approach to CBD; TD, transcholedochal approach to CBD.
Conclusion
In our opinion, all modalities and approaches for management of CBD stones should be available and efforts should continue to ensure progress and development in these procedures with enough well-trained medical personnel available to perform them. The future should hold a complementary and multidisciplinary approach in dealing with patients with CBD stones.
Despite the small number of cases in this study, LCBDE is feasible and appears safe as a secondary procedure after failed ERCP. The new technologies and the advancement of surgical techniques will continue to improve success and reduce morbidity.
Footnotes
Authors' Contributions
M.A-.A.: Data curation, Writing—Original draft, Conceptualization, and Investigation; R.E.B.: Formal analysis and Methodology; H.W.: Data curation; T.B.: Supervision and Project administration; A.R.: Supervision, Project administration, Conceptualization, and Writing—Review and Editing
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.