
Abstract
Purpose:
The classical colon substitution procedure is open surgery. Still, technological developments could allow a minimally invasive procedure that might improve patient outcomes. To present the efficacy and safety of esophagocolonic OrVil anastomosis after minimally invasive esophagectomy.
Methods:
This retrospective study included 10 patients with esophageal cancer treated with OrVil anastomosis (OA) between August 2017 and May 2021 at Department of Thoracic Surgery, Nanjing Lishui People's Hospital, Zhongda Hospital Lishui Branch, Southeast University, Nanjing, China and the Fourth Associated Hospital of Anhui Medical University. The patient's characteristic information and related perioperative indexes were collected from the hospital's electronic medical record system and the patients were followed up.
Results:
The mean operative time and median intraoperative blood loss were 530 ± 88 minutes and 200 (range: 100–300) mL, respectively. A median of 26 (range: 13–30) lymph nodes was dissected per patient. The median total duration of hospitalization and postoperative hospitalization was 32 (range: 24–64) and 15 (range: 12–42) days, respectively. Seven (70%) patients had postoperative pulmonary infections. Two (20%) patients had postoperative respiratory failure. No esophagocolonic anastomotic leakage was observed in all cases. One patient was complicated with postoperative colonicoduodenal anastomotic leakage after the operation and was cured. However, 1 (10%) of the remaining 9 patients died from colonicolonic anastomotic leakage during hospitalization. The living 9 cases were followed up, and the median overall survival time was 36 months.
Conclusion:
Colonic interposition for esophageal cancer is effective and safe using the minimally invasive OA technique.
Core Tip
This study suggests that colonic interposition for esophageal cancer combining OrVil anastomosis and thoracoscope-laparoscope-based minimally invasive surgery is effective and safe in patients with esophageal cancer when the stomach cannot serve as a substitute for the esophagus without increased operative time, complications, and mortality compared to the literature.
Introduction
E
Small early lesions can be resected using endoscopic procedures, but larger, more extensive lesions will require esophagectomy.2–4 The stomach is the usual organ of choice for esophageal replacement, and gastric pull-up is a standardized, fast, and safe procedure, requiring only one anastomosis either in the thorax or in the neck, and is usually performed with minimally invasive techniques. 6 The colon can be used when the stomach is not available or when stomach pull-up is impossible,7,8 but colonic interposition is a technically challenging procedure.9–12
The classical colon substitution procedure is an open surgery. 13 Still, with the development of thoracoscopic Ivor-Lewis esophagogastric anastomosis technology, there are many kinds of literature reports that the application of thoracoscopic Ivor-Lewis esophagogastric OrVil anastomosis (OA) technology has achieved satisfactory results. With these foundations, the application of thoracoscopic esophagocolonic OA procedure becomes possible, which might improve patient outcomes.14–17 According to the available literature, only Kang and others reported 4 cases of successful thoracoscopic esophagocolic OA. 18
This study aimed to present a double-center experience of colonic interposition for esophageal cancer with the left colon-artery supplying colonic segment, combining the advantages of the OA technique and thoracoscope-laparoscope-based minimally invasive surgery.
Materials and Methods
Study design and patients
This retrospective case series study included patients with esophageal cancer treated with OA between August 2017 and May 2021 at Department of Thoracic Surgery, Nanjing Lishui People's Hospital, Zhongda Hospital Lishui Branch, Southeast University, ( Nanjing 211200, China) and at the Department of Thoracic Surgery of the Fourth Associated Hospital of Anhui Medical University (Hefei, China). The inclusion criteria were (1) definitive diagnosis of esophagus cancer by preoperative esophagogastroduodenoscopy, barium meal, and thoracic and abdominal computed tomography (CT), (2) T1-3 according to the AJCC staging manual, 8th edition, 13 (3) adequate pulmonary function allowing the use of single-lung ventilation, and (4) the stomach was not available.
The exclusion criteria were (1) history of chest surgery, (2) distant metastasis, (3) impaired cardiac, kidney, liver, or coagulation function, or (4) ulcerative colitis. CT staging was performed preoperatively. Preoperative history of chronic diarrhea, hematochezia, mucus stool, and schistosomiasis should be known, except for colonic diseases. Colonic fiberscope examination should be performed for patients suspected of colonic lesions. This study was reviewed and approved by the ethics committee of the Fourth Associated Hospital of Anhui Medical University (PJ-YX2021-011). The requirement for informed consent was waived.
Surgery
Before surgery, the bowel was prepared by mechanical cleansing. Oral antibiotics, gentamicin injection (80,000 U, bid) and ornidazole tablets (500 mg, bid), were administered for 3 days to decontaminate the colonic interposition graft before surgery. Respiratory function training was carried out before surgery. Enteral nutritional suspension (diabetes) (TPF-DM) or Kabiven TM PI was used to improve the patients' nutritional status for 1 week before surgery. Oral hygiene care was performed 1 day before surgery. The capillary blood glucose of diabetic patients is controlled at 4–12 mmol/L before operation. 19
All patients underwent general anesthesia induction intubation using cisatracurium 15 mg intravenously, sufentanil 20 μg intravenously, propofol 80 mg, midazolam 2 mg, intravenous dexamethasone 10 mg, and tropisetron 5 mg. Sufentanil was administered, 25 μg, before the skin incision, 20 μg sufentanil was administered again during surgical exploration, and 10 μg sufentanil was administered 30 minutes before the end of the operation. Cisatracurium 7 mg/h, propofol 200 mg/h, remifentanil 1 mg/h, and dexmedetomidine 25 μg/h were given by continuous intravenous pump for maintenance anesthesia. All patients were operated on in the supine position.
A thoracoscopic and laparoscopic combined approach was used for the minimally invasive resection of the esophagus. The surgeon and camera surgeon were on the patient's right and left side, respectively, and the assistant was on the left. Five ports were arranged the same way as Ma et al described. 20 The adhesions between the intestine and abdominal wall were released under laparoscopy.
As mentioned by Rice, 7 according to the surgical method and the position of colon-esophageal anastomosis, the length of the colon ring required was estimated by measuring the anterior chest surface in two conditions: (1) intrathoracic anastomosis was used as the thoraco-laparoscopic Ivor-Lewis operation, from the stump of the jejunum or duodenum (after total gastrectomy) or the middle of the stomach to the distal end of the esophagus and (2) from the stump of the jejunum or duodenum (after total gastrectomy) or the middle of the stomach to the lower esophagus when the left neck was anastomosed. An intraoperative light transmission test can also accurately determine the direction of colon blood vessels and the colon blood vessels to be preserved.21,22
The middle colic artery was exposed as far as possible to its origin from the superior mesenteric artery, and the artery was ligated at the beginning of the middle colic artery. 7 The colon transected line was located on the left side of the colon's hepatic flexure and below the splenic flexure of the colon. The colonic graft was supplied by the left colonic artery (Fig. 1). The colon's hepatic flexure and splenic flexure were freed through a 12-cm midline incision of the upper abdomen. A loop of the colon with the left colonic vessel was prepared. Enema was performed using 200 mL of ornidazole-sodium chloride injection (ornidazole: 1 g and sodium chloride: 1.8 g) and normal saline for cleaning residual feces and bacteria in the loops of the intestine.

Operation of colon replacement for the esophagus.
The proximal and distal colon were anastomosed end-to-side with a circular stapler (EEAXL31; Covidien, Dublin, Ireland). The partial jejunum or total stomach or residual stomach at the esophagojejunum or esophagogastrostomy site was removed. The distal end of the colon graft was anastomosed to the jejunum or duodenum or gastric end to end or end to side with a circular stapler (EEA28; Covidien). The proximal end of the colon graft was anastomosed with the esophageal stump by three silk threads.
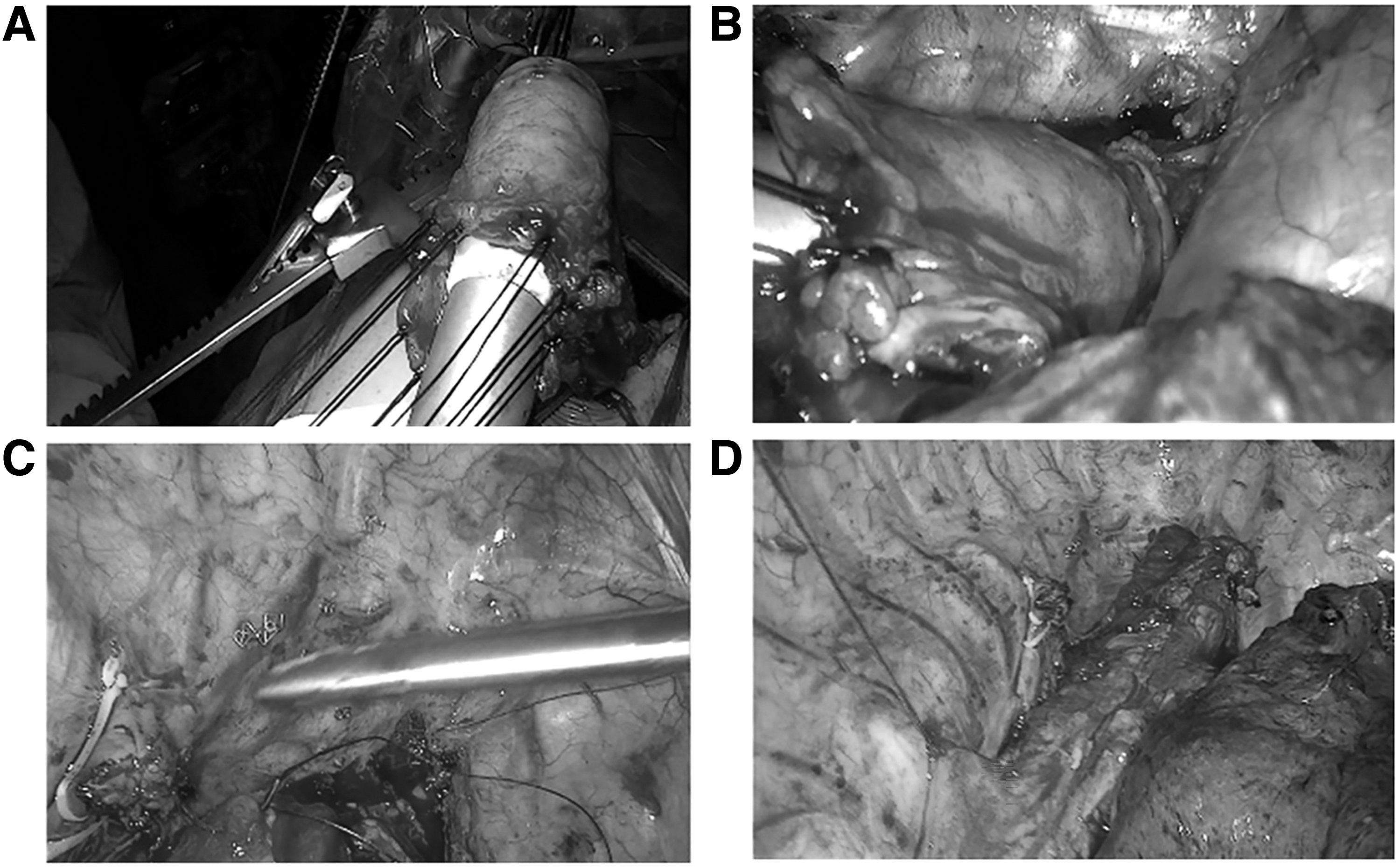
For colon grafting, the patient was placed in the left lateral decubitus position with left lung ventilation. Four working ports were created without artificial pneumothorax. Four 1-cm incisions were made at the mid-axillary line in the third intercostal space, the infrascapular line in the seventh intercostal space, the posterior axillary line in the eighth intercostal space for the 30° camera, and the anterior axillary line in the fifth intercostal space. Then the incision at the posterior axillary line was extended to 3 cm to introduce the anastomosis stapler (Fig. 2A). The esophagus was mobilized with the paraesophageal lymph nodes in an en bloc maneuver. The anastomosis's anticipated location on the esophagus was 8 cm higher than the superior edge of the tumor. 23

Thoracic surgery incision, esophagus segmentation level under thoracoscopy, and OrVil lead from the proximal end of the esophagus.
Particular attention was paid to protecting the thoracic duct, especially at the azygos, and to protecting the main bronchus, especially the left main bronchus. The azygos vein was divided and clamped using a Hem-o-Lok. The level 7 lymph nodes were completely dissected. The left and right para-recurrent laryngeal lymph nodes were selectively dissected. The turn-angle model 60 disposable Endo-GIA (staplers of 4.8 mm) was used to disconnect the esophagus from the top of the chest (Fig. 2B) or the neck, and an opening was cauterized on the stump of the esophagus (Fig. 2C). The OrVil guide was orally inserted into this opening to extract the OrVil Anvil head (Fig. 2D). The adequate length of the colon loop was raised from the esophageal hiatus to the right thoracic cavity. The colon's proximal graft was dragged out of the right thoracic cavity from the posterior axillary line port in Figure 2A(c).
The edge of the whole circumference of the colon graft proximal end was sutured intermittently with 7–0 silk thread for traction. An end-to-side colon-esophagus anastomosis was performed at the top of the chest by lifting the proximal traction line of the colon loop, by feeding it into the 25 staplers in a controlled manner (EEAORVIL25A; Covidien) (Fig. 3B), and the stump of the colon was transected using an Endo-GIA (staples of 3.5 mm).15,24 The colon loop was suspended and fixed with three stitches in the right parietal and right parietal pleura at the top of the right chest (Fig. 3C), and the whole operation was completed (Fig. 3D). A gastrointestinal decompression tube was placed to the site near the colo-jejunal or colo-duodenal or colo-gastric anastomosis. If necessary, the cervical anastomosis process was similar to that described by Yajima et al.15,25,26
With the assistance of the circumferential traction line, the proximal end of the transplanted colon is sent to the extended curved anastomosis, and end-to-side anastomosis of the colon and esophagus is performed, and the colon is suspended and fixed.
Postoperative nursing
After the operation, the patient was sent to the intensive care unit (ICU) for observation, and the tracheal intubation was removed. Attention was paid to prevent the thoracic and abdominal drainage tube from accidentally falling off, observe the drainage volume, observe blood volume, and prevent pulmonary edema caused by circulatory overload.
On the first or second day after the operation, the patient was transferred from the ICU to the general ward and was given 3–4 L/min of double nasal oxygen inhalation. The patient was assisted in mobilization, and the back was pat to assist expectoration. 27 Intravenous nutrition support was given. Enteral nutrition was gradually increased from 500 to 1500 mL, and intravenous nutrition was reduced accordingly and eventually stopped. Prophylactic administration of cephalosporin did not exceed 48 hours.
The patient was encouraged to gradually strengthen getting out of bed on the third day after surgery. About 1 week after the operation, The gastrointestinal decompression tube was removed, and the patient gradually recovered from a liquid diet to a semiliquid diet and eventually a normal diet.
Data collection
The patient's characteristic information (including age, sex, body mass index [BMI], cancer location, lifestyle habits, comorbidities, and history of disease) and related indexes during the operation (operative time, intraoperative bleeding, lymph node dissection, total hospitalization time, and duration of postoperative hospital stay) were collected from the hospital's electronic medical record system. Postoperative complications were also recorded.
Statistical analysis
Only descriptive statistics were used by SPSS 22.0 (IBM Corp., Armonk, NY). Continuous data with a normal distribution were presented as means ± standard deviations. Continuous data with a non-normal distribution were presented as median (range). Categorical data are presented as n (%). The OS (overall survival rate) of patients was analyzed by Kaplan–Meier estimation.
Results
Characteristics of the patients
Ten patients were included. All procedures were completed under thoracoscopy and laparoscopy, and OA was successful in all patients without converting to open thoracotomy. As shown in Table 1, the median age was 64.5 (range: 56–76) years. Nine patients were male, and 1 was female. Esophageal cancer was located in the upper esophagus in 1 patient, in the middle esophagus in 2 patients, and the lower in 7 patients. Nine patients had a history of smoking (90%), 8 of drinking alcohol (80%), 3 with hypertension (30%), 1 with diabetes (10%), and 2 with chronic obstructive pulmonary disease (COPD) (20%). The median BMI was 18.8 (range: 15.6–27.8) kg/m2.
Characteristics of the Patients
Continuous data with non-normal distribution were presented as medium (range). Categorical data were presented as n (%). Categorical data are displayed as n (%).
BMI, body mass index; AJCC, American Joint Committee on Cancer.
Nine patients had a history of gastric surgery (90%). Five patients (50%) had squamous cell carcinoma; 3 patients (30%) had adenocarcinoma, and 1 of the 3 adenocarcinoma patients (10%) with an esophagojejunostomy adenocarcinoma received neoadjuvant chemotherapy (fluorouracil and cisplatin). Also, 2 patients (20%) had a dual-origin carcinoma (esophageal squamous cell carcinoma and gastric stump adenocarcinoma). Postoperative American Joint Committee on Cancer (AJCC) Cancer Staging, Eighth Edition (2017) classification was stage IIa-b disease (pT3, pN0, and pM0) in 5 patients, stage IIIb in 2 patients (pT3, pN1–2, pM0), and stage IVa in 3 patients (pT3–T4a, pN2–3, and pM0).
Intraoperative-related indicators
The mean operative time and median intraoperative blood loss were 530 ± 88 minutes and 200 (range: 100–300) mL, respectively. A median of 26 (range: 13–30) lymph nodes was dissected per patient. The median total duration of hospitalization and postoperative hospitalization was 32 (range: 24–64) and 15 (range: 12–42) days, respectively.
Postoperative complications
As shown in Supplementary Table S1, intraoperative and postoperative complications occurred in 0% (0 of 10) and 100% (10 of 10) of the patients, respectively. None of the patients required additional surgery or suffered from an anastomotic stricture. No esophagocolonic anastomotic leakage was observed in all cases. No graft necrosis was observed. One (10%) patient developed colonicoduodenal leakage after surgery and was cured and discharged after conservative treatment. 28 One (10%) patient died of a colonicolonic anastomotic leakage during postoperative hospitalization. Seven (70%) patients had postoperative pulmonary infections. Two (20%) patients had postoperative respiratory failure.
Follow-up
After a patient was discharged from the hospital, the patient was reviewed at the outpatient clinic or by phone every 3–6 months. The final date of follow-up was January 15, 2022. The patients were followed for 23 (range: 9–46) months, and OS was 35.14 ± 4.9 months. Brain metastasis occurred in 22% (2/9) of patients in 9 and 15 months after surgery, respectively. One patient died 23 months after surgery, and 1 patient was lost to follow-up 22 months postoperatively. A patient died of pulmonary infection in a community hospital 36 months after surgery.
Discussion
The first coloplasty as a substitute after esophagectomy was reported by Kelling in 1911, and the first clinically successful colon interposition was performed by Von Hacker in 1914. 7 Esophagocolic anastomotic fistula and colonic regurgitation were common complications when the transverse colon was interposed as a food reservoir between the esophagus and stomach or between the esophagus and duodenum, and early postoperative mortality was high, but he also mentioned the advantages of colon graft for esophagus that the colonic mucosa was resistant both to acid and to alkaline digestion and colonic interposition did not have the disadvantage of jejunum substitution for the esophagus, which was prone to dumping syndrome. 29
The left colic artery is the first branch of the inferior mesenteric artery, which is divided into ascending and descending branches. The ascending branch ascends by the descending colon and anastomoses with the left branch of the middle colic artery in the splenic flexure area to form a marginal vascular arch, accounting for 97.3% (564/582), 30 and in a series of mesenteric arteriograms, the marginal artery in the left colon was present in all the 20 cases studied (100%). 31 Meanwhile, the left colon is thinner in diameter and occupies a small volume of the thoracic cavity. So we used the left colic artery colon graft as an esophageal substitute similar to what Lee and others reported, of course; if the left colonic artery is not the dominant blood vessel supplying the colonic blood vessels, we will use the transverse colon or the right colon as a substitute for the esophagus, alternatively. 32
We had no esophagocolic anastomotic leakage, similar to that reported by Kang and others in 4 cases of esophagocolonic OA under total thoracoscopic. 18 While Lee and others reported, 11.9% (8/67) of their, 22 and 19.04% (8/42) by Huang et al 21 under a traditional non-OA anastomosis manner.
In this study, in all cases, the posterior mediastinal route was applied for colon interposition, as described previously.7,33 Our average operation time was lower than that reported in the literature, accounting for 530 ± 88 minutes and 723 ± 132 minutes, respectively. 33 Since the company, Covidien, did not have an extended circular stapler, to facilitate colon-colonic anastomosis, a small 12 cm incision was added to the upper abdomen, freeing the hepatic flexure, splenic flexure, and transverse colon and performing end-to-end anastomosis of the colon.
When doing esophagocolon OA, the loop of the colon was pulled out of the chest cavity through the thoracoscopic observable port extended to 3.0 cm, the OrVil circular stapler was inserted into the colon loop, and the colon loop was returned to the thoracic cavity, and then the tension of the traction wire was maintained during the esophagocolic anastomosis step. Being able to control the direction of the colon loop can make the esophagocolic OA uniform, which is vitally important to ensure the anastomosis under thoracoscopy and the quality of the anastomosis. On the other hand, the colon loop was suspended and fixed with three stitches in the right parietal and right parietal pleura at the top of the right chest, reducing the tension of esophagocolic anastomosis and benefiting anastomotic healing.
Meanwhile, no colon redundancy occurred, as reported previously, 34 which might be because of the use of an isoperistaltic colon graft. 21 No anastomotic stricture occurred, as reported.35,36
The postoperative complication rate in our study was 100%, mainly mild controllable complications, such as pulmonary complications, but our intrahospital mortality was 10% lower than that reported in the literature. 37 The mortality rate was inconsistently reported in the literature, ranging from 0% to 12.5%.21,26,38
After the operation, 1 patient was complicated with postoperative colonicoduodenal anastomotic leakage and was cured. However, one of the remaining 9 patients died from colonicolonic anastomotic leakage; the lack of active lavage and drainage may be the main cause of death 39 during hospitalization. To avoid intra-abdominal leaks, a colojejunal anastomosis can be considered (instead of a coloduodenal) and intraoperative indocyanine green fluorescence might help to avoid postoperative dehiscence of the colo-colic anastomosis. 39
Indeed, minimally gastrointestinal surgeries reduce the trauma and benefit postoperative recovery.25,40 Colon interposition for esophageal cancer is a known procedure, but the main feature of this study is the use of OA minimally.
This study has limitations. It was merely a series of 10 patients operated at one of two hospitals. All patients did not receive angiography before surgery in this study, especially for those with a history of gastric surgery, so we did not fully understand whether the blood supply to and venous return from the colon were accidentally damaged or variations in the blood supply to the colon itself before surgery, which might increase the risk of surgery according to the traditional literature opinions.7,31 However, one article suggested that routine preoperative colonic angiography did not reduce the occurrence of postoperative complications such as an anastomotic leak, graft necrosis, and anastomotic stricture. 41 Meanwhile, an intraoperative light transmission test can also accurately determine the direction of colon blood vessels and the colon blood vessels to be preserved.21,22
Conclusion
In conclusion, this series of 10 patients suggests that OA is effective and safe in patients with esophageal cancer. Nevertheless, longer follow-ups and larger sample size are needed to evaluate the advantages of this procedure.
Footnotes
Acknowledgments
We are grateful to the anesthesiologists and nursing teams in the operating rooms of the two hospitals for their full cooperation and support for the operations. We are also grateful to the nursing teams in the postoperative wards for taking care of the patients, especially the nurse: Wen Du. Finally, we are grateful to everyone who contributed to this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.