
Abstract
Background:
Intestinal duplication is the most common type of alimentary tract duplications in childhood. Laparoscopic-assisted surgery has become the main surgical procedure, but robot-assisted resection has rarely been reported; the aim of this study was to retrospectively present our experience with robot-assisted intestinal duplication excision using the Da Vinci Xi surgical system and discuss the technical points.
Methods:
In total, 49 patients who were diagnosed with intestinal duplication and underwent surgery from April 2020 to February 2022 in the Children's Hospital, Zhejiang University School of Medicine, were retrospectively analyzed. The data were collected including the clinical information of the patients, operative details, and postoperative outcomes.
Results:
Among these 49 patients, a total of 15 underwent robot-assisted surgery and 34 underwent laparoscopic-assisted surgery. For the robot-assisted surgery group, all the cysts were peeled off by complete endoscope, the integrity of the intestine was preserved and intestinal resection and anastomosis were not required. The operation time of 80 minutes for the robot-assisted group was not significantly longer than the 90 minutes for the laparoscopic-assisted surgery group(P > .05), but the mean time to take the liquid diet after surgery and the average length of postoperative hospital stay were significantly shorter (P < .05).
Conclusion:
Robot-assisted resection of intestinal duplication is safe and feasible and the refinement of the Da Vinci Xi surgical system was much better than that of the conventional laparoscopic equipment, resulting in significantly improved intraoperative and postoperative outcomes.
Introduction
Intestinal duplication is the most common type of alimentary tract duplication (72.0%) and the majority occurs in the ileum. 1 Its clinical presentation includes abdominal pain, vomiting, abdominal mass, gastrointestinal bleeding, and intussusception, but some may be totally asymptomatic, and identified on routine physical examination or during incidental investigations. 2 The treatment for this disease is surgical resection even if they are asymptomatic 3 and laparoscopic-assisted surgery has now become the main surgical procedure, 4 the procedures usually involving the resection of the duplication together with the adjacent normal bowel, followed by primary anastomosis.
With the development of minimally invasive technology, the invention and application of the Da Vinci robotic surgical system have created a new era of surgery. Compared with conventional laparoscopic surgery, the stability and refinement of the Da Vinci robotic surgical system are much better than those used in conventional laparoscopic surgery. 5 The Da Vinci robotic surgical system has been widely used for the treatment of various diseases, 6 and this study presents a report of its use in robot-assisted pediatric intestinal duplication excision.
Materials and Methods
Patients and clinical data
A total of 49 patients with intestinal duplication who had undergone surgical resection between April 2020 and February 2022 at the Children's Hospital, Zhejiang University School of Medicine, were studied retrospectively. The study was approved by the institute ethics committee (No. 2022-IRB-067) and the patient underwent the robot-assisted surgery or conventional laparoscopic-assisted surgery depending on the surgeon's clinical decision and the patient's and parents' preference. No specific selection criteria were used for these patients.
Surgical procedures
Robot-assisted surgery
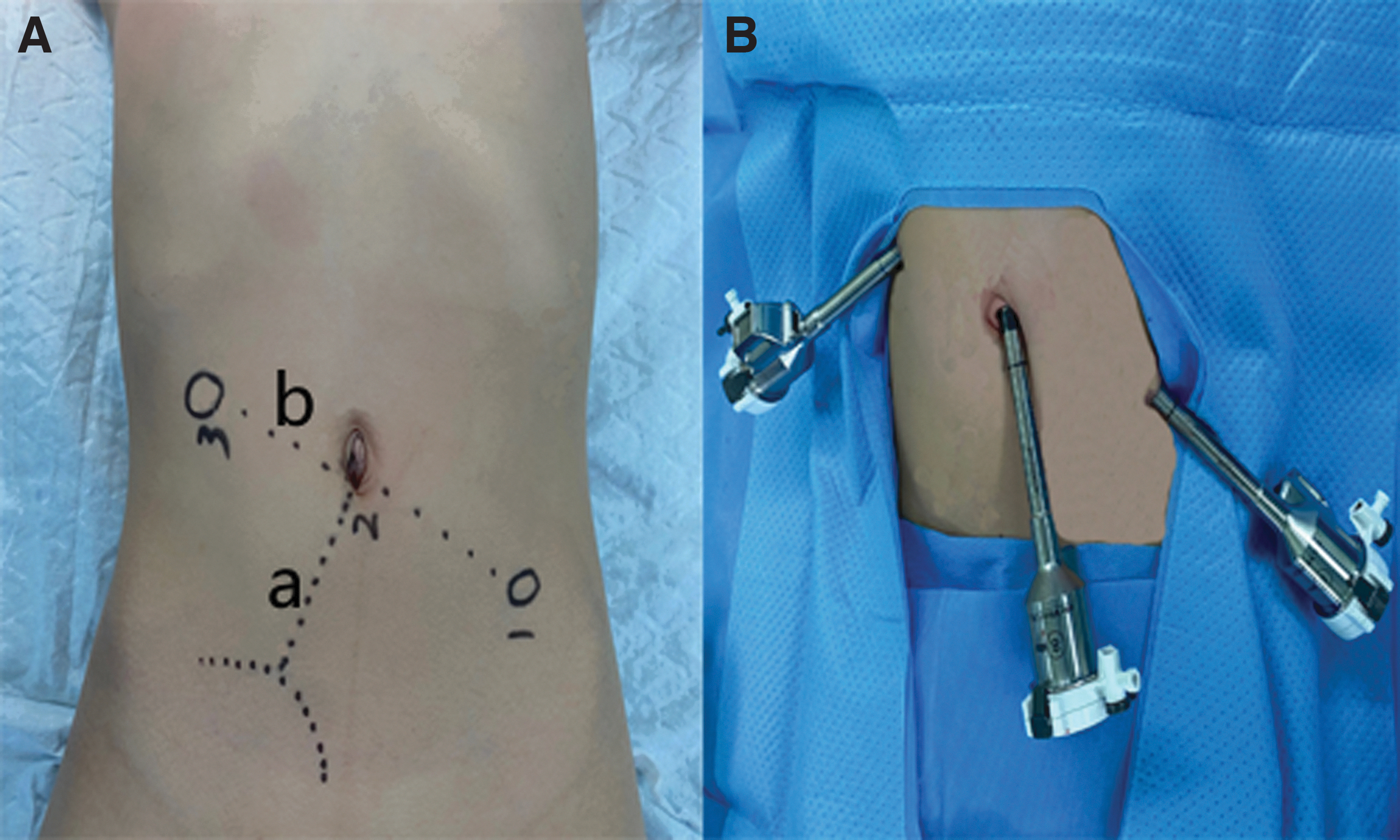
The Da Vinci Xi Surgical System was used to perform the surgery. The patient was placed in the supine position and after the pneumoperitoneum was established, an 8 mm da Vinci trocar was inserted at the umbilical incision, which was used as a port for the three-dimensional (3D) camera. Another two 8 mm trocars were placed at the right upper abdomen and left lower abdomen ∼8 cm (at least 3 cm) from the umbilicus incision (Fig. 1). After setting the “ lower abdominal operation” mode of the machine, the No. 2 arm was connected to the umbilical trocar and robotic arms No. 1 and No. 3 were connected to the left lower abdominal trocar and right upper abdomen trocar, respectively.
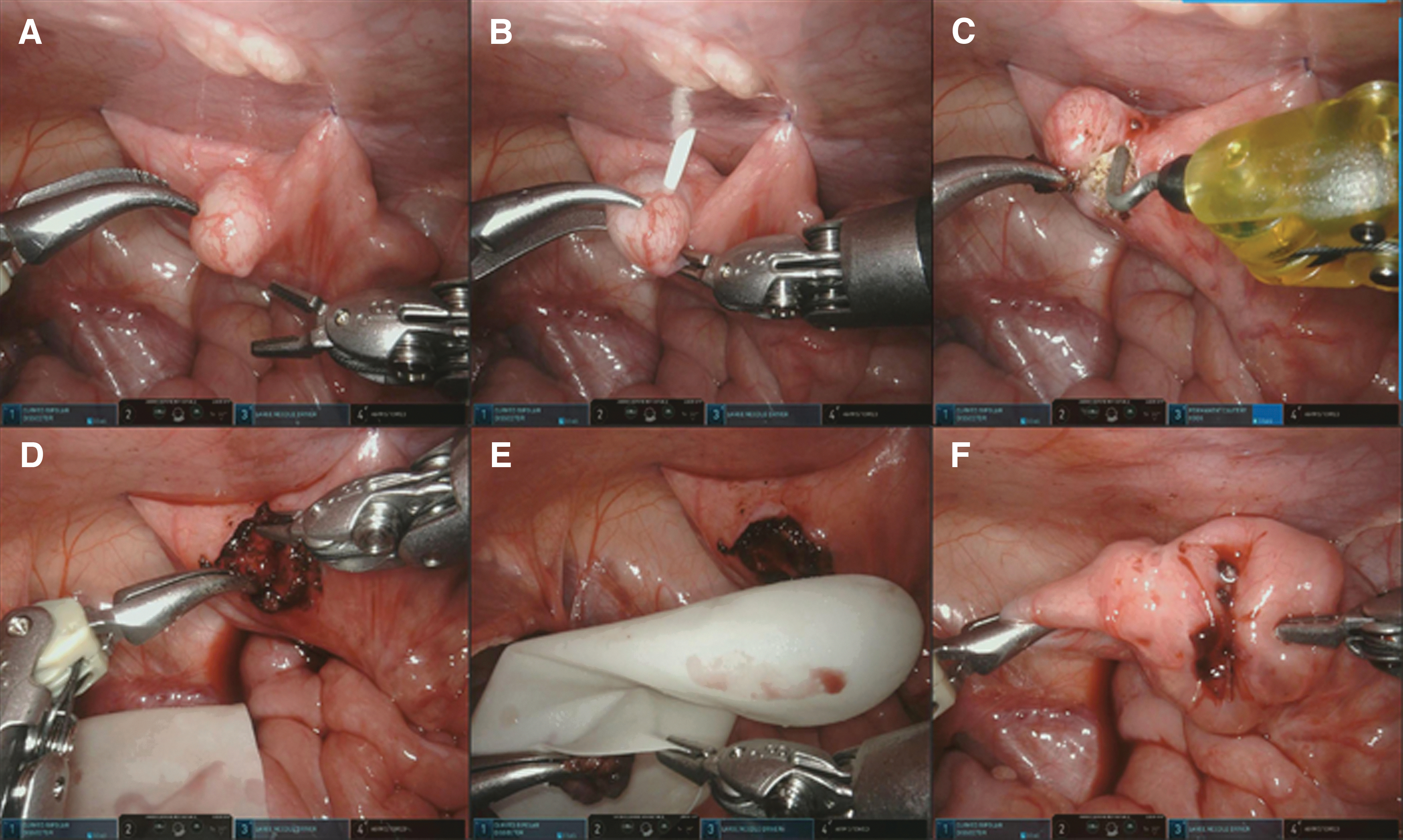
Under endoscopic monitoring, the operating devices were installed and the surgeon could explore the abdominal cavity starting from the ileocecal region. After the discovery of the diseased intestine, the bowel loop carrying the duplication cyst was suspended in the abdominal wall (Fig. 2A), which could be decompressed by puncture and aspiration (Fig. 2B) and then stripped after the tension was reduced (Fig. 2C). After the cyst was dissected, it was disposed into the retrieval bag and removed from the abdominal cavity under surveillance (Fig. 2E). A 4-0 absorbable suture was used to close the seromuscular of the local normal intestine (Fig. 2F). If no obvious bleeding was observed, the scope was withdrawn, exhausted, and the incision was sutured.
Conventional laparoscopic-assisted surgery
The patient was placed in the supine position and after the pneumoperitoneum was established, two 5 mm trocars were placed at the left upper edge incision and left lower edge incision of the umbilicus, respectively, which were used as ports for the camera and operating devices, allowing the surgeon to explore the abdominal cavity starting from the ileocecal region. After finding the lesion, the diseased bowel could be removed from the abdominal cavity through the enlarged umbilical incision, with the duplication resected together with the adjacent normal intestine. If no obvious bleeding was observed, the intestine was put back into the abdominal cavity and the incision was sutured.
Statistical analysis
Statistical analysis was performed with SPSS 24.0. Pearson's chi-square and Fisher's exact tests were used for categorical variables, and the frequencies were reported as a percentage of the group of origin. Mann–Whitney U test was utilized for continuous variables and frequency of continuous variables was reported as median and range. P values <.05 were considered statistically significant. All P-values reported were two tailed.
Results
Robot-assisted surgery
Fifteen patients (7 males and 8 females) received robot-assisted surgery, all the cysts were peeled off under complete endoscopic treatment, the integrity of the intestinal was preserved, and intestinal resection and anastomosis were not required. The median age of these patients was 19 months (range: 7.5–150 months) with a median weight of 12.4 kg (range: 8.4–44.6 kg). The median surgical time was 80 minutes (range: 40–120 minutes), and there was no blood transfusion in all patients. The median postoperative feeding time was 3 days (range: 2–4 days). The median length of postoperative hospital stay was 6 days (range: 3–8 days).
Conventional laparoscopic-assisted surgery
Thirty-four patients (19 males and 15 females) received conventional laparoscopic-assisted surgery. The median age was 43.5 months (range: 2.7–153), the median weight was 16.15 kg (range: 6.5–56 kg). The median surgical time was 90 minutes (range: 60–120 minutes). The median postoperative feeding time was 4 days (range: 2–6 days). The median length of postoperative hospital stay was 7.5 days (range: 5–13 days).
Treatment outcomes
There was no blood transfusion in all 49 patients. In the robot-assisted surgery group, all the cysts were peeled off under complete endoscopic treatment, the integrity of the intestine was preserved, and intestinal resection and anastomosis were not required. In the laparoscopic-assisted surgery group, the diseased intestine was exteriorized, then only in 2 cases, the cysts were peeled off, the integrity of the intestinal was preserved, for the remaining 32 patients of this group, it was difficult to distinguish the boundary between the cyst and normal intestinal canal, so the cysts have to be resected together with the adjacent normal intestine and the intestinal anastomosis has to be performed.
One case in the laparoscopic group had a postoperative incision infection, which was cured by conservative treatment. All other patients recovered well after the surgery, the abdominal incision of the patients was well healed 3 months after the operation, and no obvious abnormality was found on B-ultrasound. There was no significant difference in patients' age and weight between two groups (P > .05) and the postoperative feeding time and the length of postoperative hospital stay time of robot-assisted surgery group were significantly shorter than that of laparoscopic-assisted surgery group (P < .05) (Table 1).
Clinical Parameters of the Patients
Discussion
Compared with conventional laparoscopic surgery, the Da Vinci robotic surgical system features hand tremor elimination, motion scaling, and motion indexing. It provides 3D high-definition vision and higher magnification up to 10 × , allowing for more accurate vision and more precise dissection. 7 It can also maintain the lens clarity for a long time without being affected by smoke, ensuring the smoothness of the entire operation process without interruption and save operation time. The three simulated wrist instruments possess seven degrees of freedom of movement, which can help the surgeon complete the operation in a narrow space and greatly improve the stability, accuracy, and safety of the surgical operation. 8
The cysts of intestinal duplication are often cowalled with normal intestinal canal, and it can be difficult to distinguish their boundaries with the naked eye using ordinary laparoscopic instruments, therefore, it is difficult to perform traditional laparoscopic surgery with complete laparoscopy.9,10 In most cases, the umbilical incision has to be enlarged, the diseased intestine has to be exteriorized, the local intestine has to be resected, and the intestinal anastomosis has to be performed. 1 Although surgical trauma has been reduced compared with traditional open surgery, some bowel loops still need to be exposed outside the body when removing the cyst and performing intestinal anastomosis, so there are still risks of intestinal adhesions and intestinal fistulas after surgery.
The Da Vinci surgical system has higher clarity and resolution, which can help the surgeon distinguish the cyst wall from the normal intestinal wall, so that the cyst can be peeled off using complete laparoscopic surgery. This avoids exteriorizing the intestine, and resection and anastomosis of the intestine are not required, all of which can further reduce the incidence of intestinal adhesions, intestinal obstruction, and intestinal fistulae, and the patients recover faster after operation.
The selected position of the puncture operation hole on both sides should be ∼8 cm from the umbilicus (at least 3 cm), which can avoid the restriction of the mechanical arm activity, because of the lack of force feedback, the surgeon needs to reduce the action of clamping the intestine and try to avoid clamping too much intestinal tissue so as not to damage the intestinal wall. The bowel loop carrying the duplication cyst can be suspended during the operation, which can not only avoid the use of additional trocars and reducing the incision but also better expose the cyst, making it more conducive to stripping. The cyst can be aspirated by puncture, which can reduce the local tension to strip the cyst without damaging the normal intestine.
The Da Vinci system also has shortcomings, which are mainly reflected in (1) high total hospitalization costs and (2) longer procedure time. The high surgical cost of the Da Vinci system, which is at the patient's own expense, is by far the biggest problem for this technology to be used routinely, 11 Assuming that traditional laparoscopic surgery can be performed well, the Da Vinci system still needs development time before being more widely used. Installation is time consuming and the replacement of the Da Vinci Si system by the Da Vinci Xi system significantly shortened the installation time. 12
The limitations of this study are its retrospective nature and small sample size, so a larger multicenter prospective clinical trial and long-term follow-up are deemed necessary to validate the probable advantages of this technique.
Conclusion
Robot-assisted intestinal duplication excision appears to be safe and feasible, and the reduction in the duration of the operation, the start of enteral nutrition, the duration of hospitalization were due to the use of a simpler and faster manipulation technique (enucleation). This study showed that owing to its stability and refinement, it was suitable to perform robot-assisted intestinal duplication excision in pediatric patients.
Footnotes
Authors' Contributions
Y.J. contributed to data curation and writing—original draft preparation. Y.Z. was involved in conceptualization and methodology. D.C. carried out formal analysis and visualization. Z.H. carried out investigation. S.Z. was in charge of software and validation. J.M. was in charge of supervision. Z.G. carried out writing—reviewing and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.