
Abstract
Background:
With the development of minimally invasive techniques, laparoscopic adrenalectomy (LA) has become the standard for the treatment of adrenal surgical diseases, but conversion to open adrenalectomy (OA) is also necessary in some cases. The purpose of this study was to investigate the risk factors for conversion from LA to OA.
Methods:
A retrospective study was performed on 911 patients who were diagnosed with adrenal tumors and underwent LA in the Department of Urology, Second Hospital of Lanzhou University from January 2013 to December 2021. According to the surgical methods, the patients were divided into the laparoscopic group (n = 873) and the conversion group (n = 38). Logistic regression was used to analyze the independent risk factors of conversion, and the logistic regression equation was established to predict the probability of conversion.
Results:
In this study, 38 patients (4.17%) were converted to open. In the univariate analysis, body mass index (P = .037), tumor side (P < .001), tumor size (P < .001), surgical approach (P < .001), and histological type (P = .006) were significantly associated with conversion. In the multivariate analysis, tumor diameter >7 cm (odds ratio = 2.835, 95% confidence interval 1.096–7.335; P = .032), transabdominal approach (odds ratio = 2.400, 95% confidence interval 1.136–5.074; P = .022), pheochromocytoma (odds ratio = 5.018, 95% confidence interval 1.964–12.822; P = .001), and malignant tumor (odds ratio = 17.781, 95% confidence interval 4.156–76.075; P < .001) were independent risk factors for transition opening. The logistic regression equation showed good power to predict conversion.
Conclusion:
Tumor size, surgical approach, and histological type were predictive factors for conversion from a laparoscopic to an open procedure. Preoperative evaluation of these characteristics is of great value for clinicians to evaluate the risk of conversion and make a surgical plan. It can not only reduce the conversion rate but also help to improve the intraoperative situation and shorten the length of hospital stays.
Introduction
Laparoscopic adrenalectomy (LA) was first described by Gagner et al. 1 in 1992 and has replaced the traditional open adrenalectomy (OA) as the standard operation for adrenal tumors. It has significant advantages such as less intraoperative bleeding, light postoperative pain, and short hospital stay. However, the surgical operation space of LA is relatively narrow, and conversion may be finally selected for various reasons during surgery. Therefore, if the risk factors related to conversion can be clearly identified before surgery, objective assessment of operation difficulty, special preoperative preparation, or strict control of surgical indications can improve the efficiency and safety of surgery, make sure the surgery goes smoothly so as to reduce the conversion rate, alleviate the pain of patients, and improve the quality of medical care. There is no consensus on the risk factors for conversion. In this study, we retrospectively analyzed the clinical data of patients diagnosed and treated in our hospital to investigate the independent risk factors for conversion from LA to OA.
Methods
A retrospective descriptive observational study was performed on 911 patients with LA in the Department of Urology, Second Hospital of Lanzhou University from January 2013 to December 2021. If the laparoscopic surgery was successfully completed, the patients were included in the laparoscopic group. If the patients were found to have difficult bleeding control, serious adhesion between the tumor and surrounding tissues, tumor rupture, failure to identify target lesions, peripheral viscera injury, etc., and chose to conversion from a laparoscopic to an open procedure, the patients were included in the conversion group. All operations were performed by experienced and senior urologists. The study was approved by the Clinical Research Ethics Committee, and all patients were fully informed of the procedure before signing the informed consent.
To distinguish it from the enlarged incision for specimen removal, we defined the conversion to open as an enlarged abdominal wall incision greater than 5 cm to prevent serious complications. The following variables were collected for all patients, including gender, age, body mass index (BMI, according to the Chinese BMI reference standard classification), previous abdominal surgery, coexisting hypertension, or diabetes, tumor side and size (obtained from computed tomography scan), the American Society of Anesthesiologists (ASA) grade, surgical method, and histopathological type. In addition, the analysis of relevant indicators such as operative time, intraoperative blood loss, intraoperative blood transfusion and postoperative hospital stay was performed for both groups.
Statistical analyses
Categorical variables were expressed as percentages and analyzed using the χ 2 test or Fisher's exact test; the Kolmogorov–Smirnov test was used to determine whether continuous variables were normally distributed and expressed as mean and standard deviation or median and interquartile range (25th–75th percentile), and Student's t-test or Mann–Whitney U test was used for analysis. Univariate and multivariate analyses were performed by logistic regression model (Enter method). The odds ratio and 95% confidence intervals were calculated. The optimal cutoff point was evaluated with the receiver operating characteristic (ROC) curve and maximum Youden index. The area under the curve (AUC) was calculated to evaluate the efficiency of the logistic regression equation. Statistical significance was set at P < .05 and two-tailed tests were used in hypothesis testing. Data were analyzed using the SPSS 26.0 statistical program for Windows.
Results
During the study period, 911 patients underwent LA. The characteristics of patients are shown in Table 1. There were 413 men and 498 women, with a median age of 49.0 years. 3.5% of patients were lightweight (BMI <18.5 kg/m2) and 60.4% were overweight (BMI ≥24 kg/m2), 14.4% patients had a history of abdominal surgery, 60.6% with hypertension, and 13.1% with diabetes. The tumor affected the left gland in 51.8% of cases and ectopic lesions in 2.7%, and 23.9% with an ASA score of being equal or greater than 2. The tumor was larger than 7 cm in 6.6% of patients, and 79.8% had retroperitoneal space surgery. Postoperative histopathological results showed that adenoma was the most frequent (63.2%), followed by pheochromocytoma (18.4%), and also included myeloid lipoma, malignant tumor, cyst, granulocytic neurofibroma, eosinophilia, schwannoma, tuberculosis, and teratoma. All patients underwent unilateral surgery, of which 38 cases (4.17%) were converted to open surgery. The median postoperative hospital stay was 6 (1–27) days, and 322 cases (35.3%) had relatively prolonged hospital stays.
Demographic Data and Characteristics of Patients Undergoing Laparoscopic Adrenalectomy
ASA, the American Society of Anesthesiologists; BMI, body mass index.
Analysis of risk factors for conversion from LA to OA
Variables associated with conversion in the univariate analysis are shown in Table 2. No significant relationship was found between the likelihood of conversion and any of the following variables: gender, age, hypertension, diabetes, previous abdominal surgery, and ASA grade. BMI, tumor side and size, surgical approach and histological type were significantly associated with conversion to open surgery. In the multivariate analysis, tumors >7 cm, transabdominal approach, pheochromocytoma, and malignancy were independent risk factors for conversion (Table 3).
Variables Associated with Conversion to Open Surgery in the Univariate Analysis
The significance of bold values represent P < 0.05.
ASA, the American Society of Anesthesiologists; BMI, body mass index.
Variables Associated with Conversion to Open Surgery in the Multivariate Analysis
The significance of bold values represent P < 0.05.
BMI, body mass index.
Establish logistic regression equation and predict its efficiency
The regression equation was established: Ln (P/1 − P) = β0 + β1X1 + β2X2 + β3X3 + β4X4 = −4.202 + 1.042X1 + 0.876X2 + 1.613X3 + 2.878X4. X1 is tumor diameter >7 cm, X2 is the transperitoneal route, X3 is pheochromocytoma, and X4 is the malignant tumor. Hosmer–Lemeshow goodness-of-fit test of regression equation showed that the model was reasonable (χ 2 = 3.088, P = .877).
The segmentation point (the optimal cutoff value) of the logistic regression equation in this study is the predicted value = 0.040. P ≥ .040 was considered as estimated positive, and P < .040 was considered as estimated negative, and a cross-classification table was made (Table 4). Respectively, the results showed that the sensitivity, specificity, positive predictive value, negative predictive value, false-positive rate (misdiagnosis rate), and false-negative rate (missed diagnosis rate) of the regression equation were 81.6%, 78.4%, 13.8%, 99.0%, 21.6%, and 18.4%. The AUC of ROC curve was 0.836 (Fig. 1), which indicates that the equation has a good power to predict conversion.
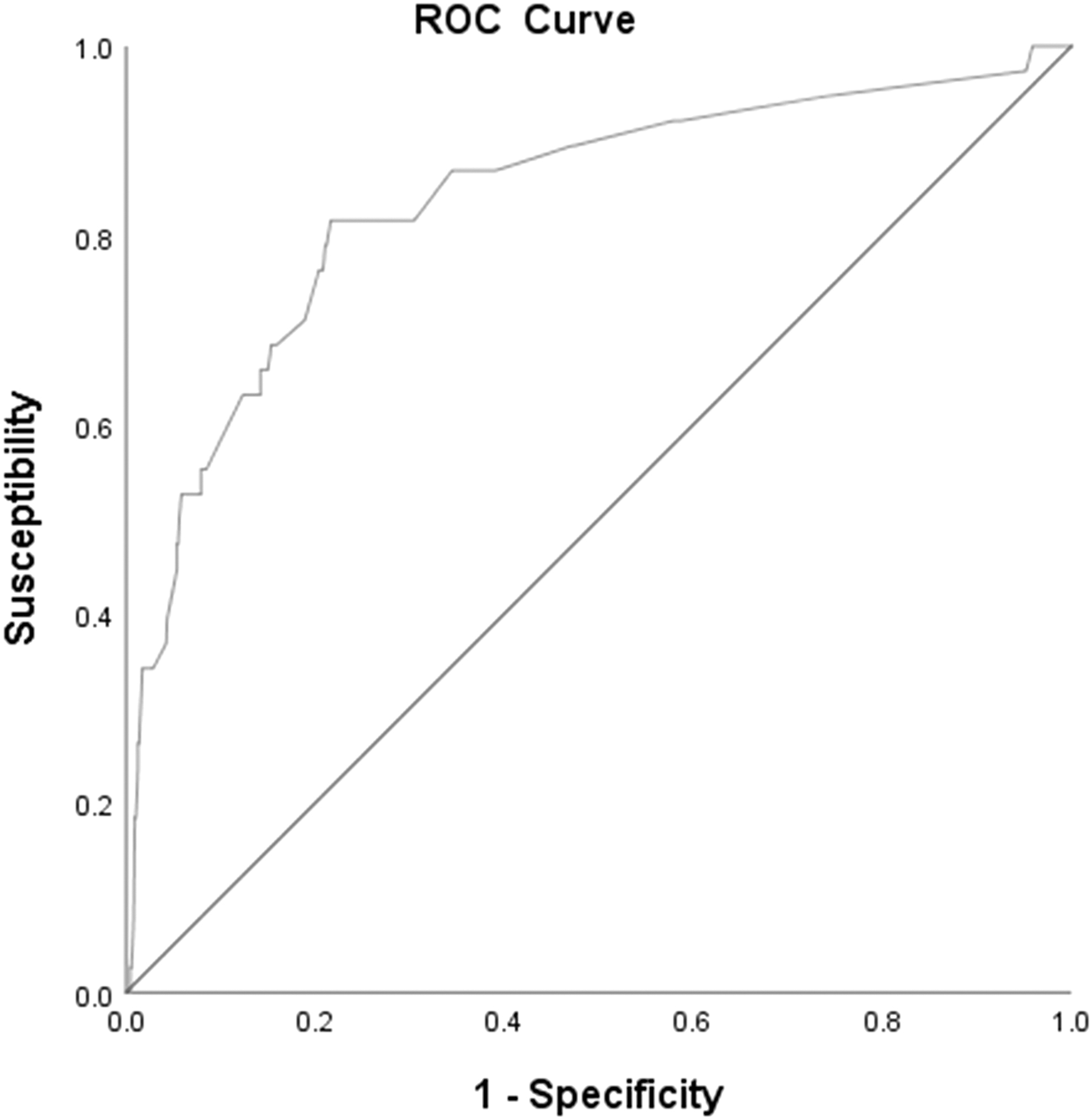
ROC curve of the logistic regression equation. ROC, receiver operating characteristic.
Cross-Classification Table of Observed Numbers and Regression Equation Estimated Number [n (%)]
Comparison of intraoperative and postoperative indicators
The results showed that the laparoscopic group was superior to the conversion group in terms of operative time, intraoperative blood loss, intraoperative blood transfusion rate, and postoperative hospital stay, and the differences had statistical significance (P < .05) (Table 5).
Comparison of Intraoperative and Postoperative Indicators in the Laparoscopic Group and Conversion Groups
IQR, interquartile range.
Discussion
The adrenal tumor is a common urological disease, with a prevalence of 1.5%–9.0% in the general population. 2 The incidence of adrenal incidental tumors is also increasing year by year with the development of global aging and the progress of imaging technology, with an incidence as high as 7%–10% in the elderly. 3 Currently, the undisputed benefits of LA render it become the first choice for adrenal lesions, but several factors may increase the risk of conversion and also lead to increased intraoperative blood loss and prolonged operating time and hospital stay. The conversion rate in this study was 4.17%, which was consistent with the 2.8%–13% reported in the literature. 4 The most common reasons for conversion were bleeding and adhesion. In this study, we systematically reviewed the clinical data of patients and analyzed several factors that may lead to conversion. The results showed that tumor diameter >7 cm, transperitoneal approach, pheochromocytoma, and malignant tumor were independent risk factors for transition and opening.
In this study, the univariate stratified analysis showed that overweight instead became an inhibiting factor of transition opening compared with patients with normal BMI (BMI ≥24 kg/m2, β = −0.708, P = .036), so we believe that LA is also safe and feasible for overweight patients. The results of the study by Rodriguez-Hermosa et al. 5 showed that there was no significant difference in the conversion rate between patients with BMI <30 kg/m2 and BMI ≥30 kg/m2 (P = .467), which is similar to our results. It is considered that functional adrenal tumors can not only lead to body weight loss due to long-term high hormone-metabolic levels, but also cause intraoperative hormone release leading to hemodynamic instability (HI) and transition to opening. That is, patients with lower BMI may be functional tumors and transition to opening easily, while those with relatively higher BMI were more likely to be free of functional tumors and at lower risk of transition. Thus, the strength of tumor function may be correlated with BMI.
However, some researchers 6 believe that BMI >30 kg/m2 is a risk factor for LA conversion. They believe that the reason why LA does not apply to obese patients may be related to difficulty in anesthesia intubation, small operating space, excessive fat affecting anatomy, and difficulty in instrument operation due to excessive abdominal wall thickness. At present, there is no agreement on the relationship between BMI and transit, and prospective studies with a large sample size are expected.
Univariate analysis showed that retroperitoneal ectopic tumors (β = 2.654, P < .001)were closely related to conversion, and accounted for 18.4% of all patients with transit, including 2 cases of malignant tumor and 5 cases of paraganglioma. The causes of conversion were related to the dense distribution of retroperitoneal great vessels and organs prone to injury, adhesion around metastatic tumors, and special endocrine function of pheochromocytoma. However, the results of multivariate analysis showed that ectopic tumor was not an independent risk factor for transition and opening, which was consistent with the results of some foreign studies.7–9
Several studies have shown that tumor size is an independent risk factor for conversion.9,10 Feo et al. 11 reported that the conversion rate of tumor diameter greater or equal to 5 cm was 6.0%. Vidal et al. 7 reported that the conversion rate of tumors >5 cm was 18.2%, and in this study, the conversion rate of tumors >7 cm was 18.3% (11/60). Large adrenal mass conversion may be due to inadequate preoperative preparation, tumor growth leading to changes in the normal anatomical relationship of neighboring tissues, lack the operation space, the risk of increased malignancy (>6 cm tumor, malignant risk as high as 25%), 12 and rich collateral circulation of tumor and surrounding tissue abnormalities, vascularization, central vein ligation increased difficulty, etc. Different from preferentially precise dissection and ligation of the central adrenal vein for functional tumors, it is difficult to separate the veins for large tumors due to insufficient operation space, and most of them adopt the method of first exposing the tumor and then ligation of tumor veins, which increases the possibility of damaging the tumor vessels.
At present, the maximum tumor diameter of LA that can be applied is inconclusive. It is reported in the literature that the maximum is 22.5 cm. 13 The size of tumors is not an absolute contraindication for LA, and the integrity of the tumor capsule, the degree of infiltration or adhesion between the tumor and surrounding tissues, and the technical proficiency of the surgeon should be considered comprehensively.
Prudhomme et al. 14 and the results of this study showed that the transabdominal approach was an independent risk factor for the conversion to open surgery. Economopoulos et al. 15 and Marrero et al. 16 also proved that the transabdominal approach had a higher conversion rate, which may be related to the increased difficulty of surgery caused by abdominal organ injury or interference and the inability to control tumor vessels at an early stage. There are many reports on the comparison of the advantages and disadvantages of the transabdominal approach and the retroperitoneal space approach. The retroperitoneal space approach can eliminate the influence of surrounding tissues and expose the tumor with better effect, which is conducive to the precise dissection and ligation of the tumor vein as early as possible. However, the transabdominal approach has a large surgical space and the surgeon is relatively familiar with the abdominal anatomy, which may be more conducive to surgical resection of larger tumors.
LA is still challenging for special histopathological types of tumors, especially pheochromocytoma and malignancy. Vidal et al. 7 and Nel et al. 17 found that pheochromocytoma had a higher conversion rate than other tumors, and was 14.6% (19/130) and 19.5% (8/41), respectively, and this study was 10.8% (18/168), which was related to the proliferation and numerous branches of tumor nourishing vessels, the close relationship between tumor and large surrounding vessels, pneumoperitoneum pressure, and operative procedure that induced a large number of catecholamine secretion. So preoperative blood volume supplementation and drug preparation are crucial in reducing the incidence of HI and conversion rate. Delozier et al. 18 found that the conversion rate of adrenal cortical cancer was as high as 19.4% (38/196), and Thompson et al. 9 demonstrated that malignant tumors were significantly correlated with LA conversion (P = .002). Therefore, LA is generally not recommended when malignant tumors are suspected.
Preoperative needle biopsy for the adrenal tumor is not recommended because of the risks of hemorrhage, cyst rupture, local tumor infiltration, and hypertensive crisis. When the malignant tumor is suspected during the intraoperative exploration, it may be converted to open to meet the negative margin standard. Unlike primary adrenal malignancies, adrenal metastases tend to be smaller and do not invade the adrenal capsule and are therefore more suitable for LA.
The results showed that the endoscopic group was superior to the conversion group in terms of operative time, intraoperative blood loss, intraoperative blood transfusion rate, and postoperative hospital stay, which was consistent with the study results of Al-Jalabneh et al. 19 Clinicians should correctly view conversion to open surgery, which is not surgical complications or surgical failure, but a wise choice to prevent the occurrence of serious complications. Although conversion can prolong the operation time and hospital stay, the decision on whether to open transfer should be based on the safety of patients' lives rather than simply pursuing minimally invasive surgery. In addition, the Da Vinci Surgical System has been widely used in adrenal surgery, reducing hand tremors and providing three-dimensional imaging, clearer visualization and flexible arm. It can be preferred for patients with complex adrenal tumors such as large volume tumors, complex vascular adjacents, pheochromocytoma and paraganglioma, and overweight or obese patients.
A large number of patients were included in the present cohort, although this study still has some limitations. First, since this is a single-center retrospective study, there may be inherent selection and bias due to failure to better minimize the interaction between variables. Second, the exclusion of some patients from this study due to a lack of clinical data may affect the results of the study.
In summary, large tumor size, transabdominal approach, pheochromocytoma and malignant tumors were predictors for open conversion of LA. Conversion is influenced by multiple factors and cannot be explained by a single factor. Surgeons should make a comprehensive assessment and effective intervention on the risk factors, so as to avoid conversion to open surgery and postoperative complications and improve the quality of medical treatment.
Footnotes
Authors' Contributions
Conceptualization and design: P.F.S. and Q.H.; data curation: Q.H., B.Z., and Y.L.; formal analysis and methodology: Q.H., B.Z., P.Y.W., and S.J.Y.; writing—original draft: Q.H.; writing—review and editing: P.F.S. and Q.H.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.