
Abstract
Background:
The laparoscopic sleeve gastrectomy (LSG) procedure is the most common bariatric surgical technique worldwide, but controversy continues over staple line reinforcement (SLR) techniques. This prospective randomized study aimed to compare the effects of SLR methods on early postoperative complications and gastrointestinal symptoms in patients undergoing LSG for morbid obesity.
Materials and Methods:
Ninety patients who underwent LSG surgery for obesity between June 2019 and February 2020 in the Department of General Surgery of Bezmialem Vakıf University were included in our prospective randomized study. According to the SLR techniques, three groups were determined as Group 1: using fibrin sealant (Tisseel®), Group 2: omentopexy, Group 3: no SLR, with each group having 30 randomly assigned patients. Gastrointestinal symptoms were assessed by performing the Gastrointestinal Symptom Rating Scale (GSRS) for all patients following the first week and first month. On the second postoperative day, all patients underwent swallow-graphy to investigate twists and fistula.
Results:
The test group included 90 patients totally, of which 17 are males and 73 are females with a mean age of 35.3 ± 11.6 years and a mean body mass index of 45.3 ± 7.7 kg/m2. According to the GSRS, reflux and indigestion scores in Group 3 were significantly higher than those in the other groups in the first week (P < .001). There was no statistically significant difference in abdominal pain scores in the first week. Group 3's operation time was statistically significantly shorter than the other groups (Group 1 P = .005; Group 2 P = .001). In Group 3, 2 patients (2.2%) had bleeding. There was no mortality. There were no twists or fistulas found in swallow graphs. Symptomatic reflux was not observed in the first-year follow-up period.
Conclusions:
SLR methods reduce gastrointestinal system complaints in the early postoperative period. In our study, omentopexy and fibrin sealant used in LSG did not show a statistically significant difference in early postoperative complications.
Introduction
Obesity is one of the most significant health problems of the 21st century. The effects of diet, exercise, and medical treatments are limited compared with surgical treatments. 1 Laparoscopic sleeve gastrectomy (LSG) was accepted as the primary bariatric procedure by the American Metabolic and Bariatric Surgery Association (ASMBS) in 2012 and is currently the most frequently used technique in obesity surgery.2,3 This increases the importance of the complications it brings with it, the most serious of which are staple line leakage and bleeding. 4 In the literature, the rates of leakage and bleeding after LSG are between 0.5%–4.7% and 1.1%–8.7%, respectively.5,6 Staple line reinforcement (SLR) techniques can be used in LSG surgery, but there is no consensus on what comprises standard SLR techniques. 4 According to the ASMBS, 75% of bariatric surgeons prefer to use SLR, but there are a limited number of prospective randomized studies in the literature regarding the comparison of SLR techniques.7,8
Nausea–vomiting, abdominal pain, and oral intake intolerance are the leading problems of the gastrointestinal system after bariatric surgery. 9 Nausea and vomiting, at a rate of 8.5%, are the most common symptoms, especially after restrictive-type bariatric surgery procedures. 10 Postoperative nausea and vomiting are known to be directly related to reasons such as operation time, bougie size, SLR technique, anesthesia, and postoperative analgesia protocol.2,3,7 Postoperative nausea and vomiting complaints are the most common reasons for readmission to hospital (12.95%). 11 The second most common reason is abdominal pain (11.75%). 11
In the literature, it has been stated that postoperative bleeding may increase in cases without SLR, which may lead to twist and functional stenosis. It has been reported in many studies that gastrointestinal system symptoms and oral intake tolerance were observed for these reasons.3,10,12 It is thought that with the use of SLR techniques, the remnant stomach remains in a similar position to that in the normal anatomy, and thus, gastrointestinal symptoms are seen less in the postoperative period. 1 It is also observed that it decreases postoperative complications and incidences of rehospitalization and enable rapid recovery. 7
Our aim in this prospective randomized study was to compare the effects of SLR methods on gastrointestinal symptoms and early postoperative complications in patients undergoing LSG due to morbid obesity.
Materials and Methods
Study design
The study was designed in accordance with the Declaration of Helsinki Ethical Principles and was approved by local ethics committee (August 7, 2019; No: 15/11). Patients who underwent LSG surgery due to morbid obesity between June 2019 and February 2020 in Bezmialem Vakıf University Faculty of Medicine, Department of General Surgery, were included in the study.
Similar prospective and randomized studies in the literature were evaluated before power analysis. A 20% difference between groups was considered significant. It was determined that there would be 30 patients in each group and 90 patients in total, with 80% power in the 95% confidence interval (CI).4,5,13
Patients between the ages of 18 and 65 years with a body mass index (BMI) ≥40 kg/m2 or BMI ≥35 kg/m2 with obesity-related diseases such as hypertension, diabetes mellitus, hyperlipidemia, or sleep apnea syndrome were included in the study. Those who had had previous bariatric and metabolic surgery, who had been treated for esophagitis, hiatal hernia, and gastroesophageal reflux disease (GERD) detected in preoperative examinations, and who had shown hypersensitivity to antiemetics and analgesics and inflammatory or irritable bowel disease and additional surgery (such as cholecystectomy, hiatal hernia repair) were excluded from the study. All operations were performed laparoscopically by 2 experienced bariatric surgeons.
In this study, the three groups were determined as the group using fibrin tissue glue (Tisseel® fibrin sealant) (Group 1), omentopexy (Group 2), and the group without SLR (Group 3). All patients were randomized via the website www.random.org
The demographic findings of all patients, such as age, gender, comorbid diseases, anticoagulant drug use, and BMI, were recorded in the study. The preoperative, postoperative 6th- and 24th-hour hemoglobin levels, and the first, second, and third days of the postoperative drain flow were recorded to compare the bleeding. Upper gastrointestinal contrast studies were performed in all patients on the second postoperative day for leakage and stenosis. Bleeding: It was accepted that in the first 24 hours after the operation, hemoglobin value decreased by more than 2 units and/or more than 75 mL of hemorrhagic qualities came from the drain placed to the abdomen. Leakage: It was accepted that patients who presented clinically with complaints such as abdominal pain, weakness, nausea–vomiting, and fever had radiological findings of oral contrast extraction in abdomen computed tomography (CT) scan or fluoroscopy.
All patients were evaluated via the Gastrointestinal Symptom Rating Scale (GSRS) to evaluate gastrointestinal symptoms in 1 week and 1-month postoperative period. The GSRS is a questionnaire whose reliability and validity have been verified in Turkey. 14 According to the scale, gastrointestinal system symptoms can be evaluated according to five subgroups as diarrhea, constipation, indigestion, abdominal pain, and reflux complaints. 15
A standard diet program was given to all patients by a specialist bariatric dietitian before discharge. All patients were followed for 1 year after surgery.
Statistical methods
The asymptotic or exact Pearson's chi-squared test (two-way) was used according to the number of data in the cells to compare the three groups with categorical variables. The conformity of quantitative variables to the within-group normal distribution was tested via the Shapiro–Wilk test. One-way analysis of variance or the Kruskal–Wallis test was used in the comparison of the three groups according to their conformity to normal distributions. The Bonferroni correction was performed in post hoc tests. The Wilcoxon signed rank test was used to compare the changes in the first week and first month questionnaire scores within the group, and the repeated-measures variance test was used to investigate the differences between the groups. The results were analyzed using IBM SPSS Statistics (version.22) program suite. The significance limit was accepted as 0.05.
Surgical technique
Operations were performed in the French position, with the surgeon placed between the two legs, and five trocars were placed. The omentum resection on the greater curvature of the stomach was started from the proximal part of the crow's foot. The omentum was separated with a Harmonic scalpel (UltraCision®; Ethicon Endo-Surgery, Cincinnati, OH, USA) to the superior esophageal junction. The gastroesophageal junction was fully mobilized, and the blood flow preserved. Finally, the greater curvature was separated from the omentum between the gastroesophageal junction to 2 cm proximal to the pylorus. In addition, adhesions of the gastropancreatic area were opened with the preserved left gastric vascular bundle.
This process provided equal traction of the anterior and posterior walls of the stomach during resection. A 39F bougie was placed in the stomach by the anesthetist before resection. A linear roticulator stapler with a 60 mm cartridge (Echelon®; Ethicon Endo-Surgery) was used in gastric resection. In accordance with the thickness of the stomach wall, green, yellow, and blue cartridges, in total 5–6, were used sequentially. The bleeding in the stapler line was stopped with the endoclip. After the resection was completed, the guide tube was removed, and a nasogastric tube was emplaced. An intraoperative leakage test using methylene blue was routinely performed. SLR procedures were later applied in accordance with the groups.
Fibrin sealant
After gastric resection, two boxes of fibrin tissue glue (Tisseel fibrin sealant; Baxter®, Deerfield, IL, USA) were applied to the stapler line and the stomach posterior, and the omental tissue was placed on this line. Thus, stabilization of the sleeve stomach was achieved via adhesion to the pancreas at the posterior and to the omentum at the lateral (Fig. 1a).
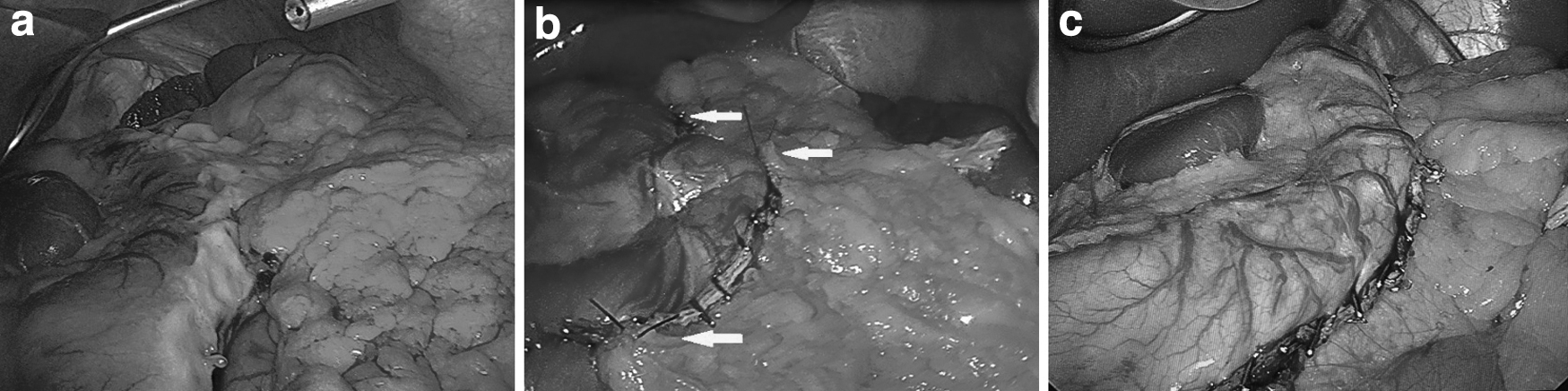
Study groups.
Omentopexy
In the omentopexy group, our aim after resection was to ensure that the sleeve stomach in the anatomical “J or inverted C” position. For this, the omentum was approached from two to four different points according to the length of the stapler line and sutured (Fig. 1b).
No SLR
It was determined as the control group, and no SLR method was used after gastric sleeve resection (Fig. 1c).
Results
Patients' data
A total of 90 patients underwent LSG between June 2019 and February 2020. Seventeen patients (18.9%) were male and 73 (81.1%) were female. The mean age was 35.3 ± 11.6 years, and their mean BMI was 45.3 ± 7.7 kg/m2. The demographic data for these patients are shown in Table 1, and it was determined that the groups were distributed homogeneously. Comparison of the postoperative findings of the patients is shown in Table 2.
Preoperative Characteristics of All Patients
BMI, body mass index; CI, confidence interval; SD, standard deviation.
Postoperative Outcomes of All Patients
CI, confidence interval; GI, gastrointestinal; SD, standard deviation.
When the operative times were evaluated for the groups, Group 3 times were found to be statistically significantly shorter than those in Group 1 (P = .005) and Group 2 (P = .001).
Leakage tests were routinely performed for all patients both intraoperatively and postoperatively, and no leakage was detected in any patient. The mean hospital stay was 3.2 ± 0.5 days. No mortality was observed. After a 1-year follow-up, the mean BMI was 28.67 ± 4.2 kg/m2 and the mean percent of excess weight loss was %73.05 ± 15.4 kg/m2. There was no significant difference between the groups in terms of weight loss (P = .478).
Complications data
For the evaluation of postoperative bleeding in each group, the mean hemoglobin values measured at preoperative (P = .411) and postoperative at 6 hours (P = .582) and 24 hours (P = .261) were compared, and no statistically significant difference was found. When the mean drain flow rates were compared between the groups (for the postoperative first day, P = .343; second day, P = .324; third day, P = .459), no statistically significant difference was found.
In Group 3, bleeding was observed in 2 patients (2.2%) during the postoperative period. One of these patients was hemodynamically stable and was followed conservatively. The patient was discharged on the seventh postoperative day. The other patient had dyspnea on the seventh postoperative day. On this patient's CT scan, effusion in the left lung and hematoma in the abdomen were observed. Tube thoracostomy and intra-abdominal percutaneous drainage were performed. In the follow-up period, the size of the hematoma regressed, and the drains were removed on the 20th postoperative day and the patient was discharged.
Two months later, the patient reported abdominal pain and fever. In the subsequent examinations, gastric fistula was detected due to intra-abdominal infected hematoma. The endoscopic double pigtail procedure was performed to deal with the fistula, and a percutaneous drainage catheter was inserted into the loculation in the abdomen. This was followed up with wide-spectrum antibiotics, and the percutaneous catheter was removed on the 20th day after the procedure. The pigtail catheter was removed with control endoscopy in the third month postoperation.
Survey data
According to the GSRS, reflux symptoms in Group 3 after the first week were statistically significantly higher than Groups 1 and 2 (P < .001). In the first month questionnaires, reflux symptoms were reported to have decreased significantly in Group 3 compared with the others (P = .001 for Group 1 and 0.007 for Group 2). However, there was a statistically insignificant increase in symptoms in Groups 1 and 2 (P = .603 and P = .807; Fig. 2c).

Gastrointestinal Symptom Rating Scale results. Changes in the first week and first month complaints between the groups:
Indigestion in the GSRS questionnaire was found to be statistically significantly higher in Group 3 than in Groups 1 and 2 (P < .001) at the first week, and in the first month, indigestion decreased in all the groups, but only that in Group 3 was found to be statistically significant (P < .001). This decrease was found to be similar in Groups 1 and 2 and was not statistically significant (P = .966; Table 3 and Fig. 2a).
Results and Changes of Patients' Gastrointestinal Symptom Rating Scale Scores at the First Week and First Month and Between the Groups
GSRS, Gastrointestinal Symptom Rating Scale.
For both the first week and first month survey results, there was no statistically significant difference between the groups in terms of abdominal pain scores (for the first week, P = .702; for the first month, P = .682; Fig. 2b).
There was no statistically significant difference between the groups with regard to diarrhea and constipation scores for the first week and first month survey results (Table 3 and Fig. 2d). In all groups, the diarrhea scores were reduced, and the constipation scores increased (Table 3 and Fig. 2e).
Discussion
Today, the most popular form of bariatric surgery is LSG. According to the ASMBS, LSG constituted 61.4% of bariatric procedures in the United States in 2018. 16 LSG surgery has become the preferred procedure within suitable patient groups due to its ease of application compared with other bariatric surgeries and its acceptable minimal mortality (0.3%) and morbidity (5.2%) rates. 3
Bleeding and leakage are the most serious complications post-LSG. 4 Leaks and bleeding usually develop from the staple line of the stomach, which is shaped into a sleeve. The bleeding rate after LSG is between 0% and 8%, and the leakage rate is between 1.1% and 8.7%.5,6,17 According to the report of the Fourth International Sleeve Gastrectomy Consensus Summit, 75% of bariatric surgeons apply SLR, whereas 57% use SLR materials and 43% prefer to support the staple line with oversewing. 18 Among these techniques, a limited number of randomized controlled studies and meta-analyses have been conducted in the literature. 5 According to the results of these studies, the effects of SLR procedures on bleeding and leakage have been discussed, but no definite conclusions have been reached on the subject.
In randomized controlled studies on SLR procedures, comparisons were mostly made between oversewing and other methods. In the meta-analysis by Wang et al, the effects of the oversewing technique and SLR products (Gore® SeamGuard® [W. L. Gore & Associates, Elkton, MD, USA], Peri-Strips Dry® [BPS; Synovis Life Technologies, Inc., St. Paul, MN, USA], and Tisseel fibrin sealant [Baxter]) on the risk of bleeding in LSG were examined; this risk was found to be statistically significantly lower in the groups using SLR products than in the no-SLR groups (risk ratio [RR] = 0.609, 95% CI = 0.439–0.846, P = .003). In the same study, the risk of leakage between the groups was not found to be statistically significant (RR = 0.654, 95% CI = 0.275–1.555, P = .337). 5
Dapri et al's prospective randomized study was performed with three different groups, including continuous suture, SeamGuard, and no-SLR groups. In this study, a statistically significantly reduction in bleeding was detected in the groups in which SLR was applied compared with those for whom it was not, but it was reported that no significant difference was found in terms of leakage. 19 It has been reported that SLR procedures reduce bleeding with their mechanical or hemostatic effect on the staple line, but on the other hand, they increase the risk of leakage due to disruption of staple line tissue with perfusion and/or ischemia, especially in cases with oversewing. 8 According to the ASMBS report, SLR is not necessary, but its application is understandable in terms of security. 8
In our study, bleeding was observed in 2 patients (6.6%) in the third group, although this was not statistically significant. In one of these patients, a leakage developed secondary to an infected intra-abdominal hematoma 2 months after the operation. Complications that may develop after surgery in obese cases can cause serious morbidity or mortality. Obese patients may present with late symptoms depending on the degree of obesity and body composition. Hematoma or abscess in the abdomen may be deeply located. Therefore, physical symptoms such as abdominal distention, tenderness, tachycardia, and fever may not develop in the early period.
For such reasons, the management of complications is more difficult than in normal patient groups. 12 In addition to the surgeon's experience, the selection of preferred techniques for primary surgery is more important to minimize the complications that may develop after bariatric surgery for these reasons. Although the results related to the effects of SLR techniques on postoperative complications in the literature are generally not statistically significant, complications are seen less frequently in patient groups in which SLR products have been applied,6,19–21 which is consistent with our study.
Studies on SLR procedures generally focus on leakage and bleeding, with a few investigating the effects on stenosis and GERD after LSG due to SLR.5–7,22 The rate of gastric stenosis after LSG is between 0.7% and 4%. 23 Fixation of the stapler line in LSG surgery is thought to prevent twisting, kinking, and organo-axial rotations of the stomach. 7 There is no standard regarding the use of the omentopexy technique with continuous or intermittent sutures, especially in cases undergoing omentopexy. While this detail is not included in some publications, it has been stated in others that omentopexy can be performed with intermittent sutures, especially to restore the anatomical position of the stomach.24–26
In the analysis performed by Aurora et al, the incidence of stenosis was reported as 0.5% in patients in whom the staple line was supported by oversewing. 27 In the study by Batman and Altun, stenosis was reported as the most common complication, with a rate of incidence of 1.3%. 25 Omentopexy can be applied to prevent organo-axial rotation after LSG. To prevent stenosis that may develop due to omentopexy, the intermittent suture technique is preferred to continuous suture. 26 In our study, omentopexy with an intermittent suture technique was applied to prevent stomach rotation and to reduce the risk of twist, and no complications were observed at the 1-year follow-up.
There are limited studies in the literature on the effects of SLR techniques on gastrointestinal symptoms. Afaneh et al investigated the effects of omentopexy on early postoperative nausea, vomiting, and GERD, but found that there was no significant difference between the control group. In the study, it was stated that the use of antiemetic drugs increased in the omentopexy group. 13 In the study by Sharma and Chau, no difference was found between the groups with and without omentopexy in terms of GERD in the postoperative period. However, it was stated that gastric symptoms (abdominal pain, nausea, bloating) were more common in the group without omentopexy. 26 In our study, the indigestion scores of the patients in Group 3 were found to be statistically significantly higher than those in Groups 1 and 2 according to the results of the first week questionnaire (P < .001). However, no significant difference was found in the first month GSRS survey results (P = .945; Fig. 2a).
LSG and reflux disease are still among the most controversial issues today. Obesity is a risk factor for the development of GERD. 28 Before LSG, the presence of GERD in the patient was previously considered a contraindication. However, in the last consensus meetings, it was evaluated as a relative contraindication, and it was stated that LSG could be applied in appropriate cases. 29 While the development of de novo GERD in the long term after LSG was reported to be 7.4% after 5 years in some studies, it was also reported to be 26.7% after 1 year in others. 29 There are different results in the few studies on the effects of SLR methods on reflux. In the literature, it is stated that the increase in the radius of curvature of the stomach, which is brought to the anatomical position with fibrin tissue glue or omentopexy, reduces the intraluminal pressure. Thus, there are publications stating that reflux symptoms can be seen less frequently.26,30
In the prospective study by Filho et al, it was found that postoperative reflux symptoms were significantly reduced in the omentopexy group in the results of the GERD evaluation questionnaire performed on the preoperative and 90th postoperative day. 31 In the studies by Afaneh et al. and Sharma and Chau, the application of omentopexy did not make a significant difference in the results of the reflux questionnaires for GERD.13,26 However, there are also studies in the literature stating that it is not appropriate to evaluate GERD based on reflux symptoms alone. In the study by Genco et al, the degree of reflux was evaluated with postoperative endoscopic findings, where it was reported that long-term reflux symptoms are inconsistent with the results of endoscopy, and endoscopic follow-ups are important in order not to miss possible GERD and/or Barrett's esophagus even if there are no reflux symptoms after LSG. 32
However, it is known that regression is seen in GERD after LSG. However, the effect of SLR procedures on reflux is not clear, and there are few studies on this subject.20,29 In our study, according to the GSRS survey results, reflux symptoms in the first week were found to be statistically significantly higher in Group 3 than in Groups 1 and 2 (P < .001), but at the end of the first month, reflux symptoms decreased in all the groups, and there was no significant difference between the groups (Fig. 2c). Furthermore, no reflux complications were observed at the 1-year follow-up.
After bariatric surgery, the most common reasons for readmission to hospital in the early period were reported as nausea–vomiting (12.95%), abdominal pain (11.75%), and dehydration (10.54%). 11 The effect of surgical technique on complications in the first 30 days is considerable. Functional stenosis or stricture may develop due to reasons such as development of hemorrhage and edema in the tissue after oversewing to the stapler line, resection too close to the bougie in the incisura angularis area, use of a bougie smaller than 36F, unequal traction of the anterior and posterior walls during the gastric resection, and staple line not being in the same line.7,11,25
We did not have any patient who was hospitalized again due to abdominal pain, nausea–vomiting, or dehydration. According to the GSRS, there was no difference in abdominal pain between the groups in the first week results (P = .702). In the study by Sharma and Chau, the groups with oversewing to the staple line and omentopexy with intermittent sutures were compared. The fact that complaints of abdominal pain were fewer in the group with intermittent sutures shows that our results are compatible with the literature. 26
In our literature, studies on SLR mostly examined conditions such as leakage, bleeding, and stenosis.6,9,19 The significant difference of our study is the investigation of the gastrointestinal system effects of SLR techniques in LSG. This is the first prospective randomized study to compare the effects of SLR techniques on gastro-intestinal system (GIS) symptoms after LSG. Similar to our study, Afaneh et al examined the effects of omentopexy only on GIS symptoms and evaluated early postoperative nausea–vomiting and reflux symptoms using the Rhodes Index Scale and the GERD impact score survey.
According to the results of this study, no statistically significant difference was found between the groups in complaints related to nausea, retching, vomiting, or reflux in the postoperative period. 13 In the study by Elbalshy et al, groups with and without omentopexy were compared in LSG. In the group without omentopexy, increased nausea–vomiting complaints and a shorter gastric transit time were found to be statistically significant. 3 In addition, the fact that there were three separate groups and the patient characteristics in the groups were homogeneous is a prominent difference of our study.
Conclusions
Discussions continue on the routine use of SLR techniques in LSG surgery. In our study, it was shown that the use of SLR methods in the early postoperative period reduces gastrointestinal system complaints. In addition, it is important to preserve the anatomical position (C or J shape) of the stomach, which is in the form of a tube sleeve in LSG, with omentopexy or fibrin glue. Thus, it was revealed that early period GIS symptoms may be reduced. For better and more robust results, there is a need for new comparative studies involving larger patient groups in which medium- and long-term outcomes are evaluated.
Limitations
The limitations to this study can be marked as the small number of patients, the inability to compare with other SLR methods, and the lack of quantitative and objective data on the effects on the gastrointestinal tract.
Footnotes
Authors' Contributions
Y.Y.: Validation, investigation, and writing—original draft. S.Y.: Formal analysis, investigation, and visualization. C.G.: Investigation, data curation, and software. H.C.: Conceptualization, methodology, and supervision. E.Y.: Conceptualization, project administration, and writing—review and editing.
Acknowledgments
The authors thank all colleagues in the Department of General Surgery at Bezmialem Vakıf University Medical Faculty for their support.
Disclaimer
The authors confirm that this work is original and has not been published before and is not currently being considered for publication elsewhere.
Disclosure Statement
No competing financial interests exist.
Funding Information
All authors declare that they haven't any financial ties to disclose and financial support for this study.