
Abstract
Aims:
To demonstrate feasibility and efficacy of simultaneous intraoperative cholangiogram (IOC) and antegrade biliary stenting (ABS) with laparoscopic cholecystectomy (LC) compared with preoperative biliary investigation and delayed LC in acute gallstone pancreatitis (AGP).
Methods:
A retrospective case–control study was performed comparing patients who had a simultaneous IOC ± ABS with LC at index admission with those who had delayed LC in the treatment of AGP. 74 patients were included in this study from January 2016 to October 2018. All patients who underwent LC for AGP were included in a prospective database with 1 year follow-up.
Results:
30 (40.5%) patients underwent simultaneous IOC ± ABS with LC, 11 of these required ABS insertion. 2 (6.7%) patients also underwent magnetic resonance cholangiopancreatography (MRCP). No patients underwent endoscopic retrograde cholangiopancreatography (ERCP). No patients were readmitted with AGP or symptomatic gallbladder. Mean length of total hospital admission was 10.1 days. 44 (59.5%) patients underwent delayed LC. Of this cohort, 7 (15.9%) patients underwent ERCP and 19 (43.2%) underwent MRCP. In total, there were 19 (43.2%) readmissions in this group with pancreatitis or symptomatic gallbladder. Mean length of total hospital admission was 13 days.
Conclusions:
In our pilot study we demonstrated that performing simultaneous IOC ± ABS with LC is a feasible option in the secondary care setting. Using this surgical technique, we have demonstrated a reduction in readmissions with AGP and symptomatic gallbladder while also reducing the number of CBD investigations required. Using simultaneous IOC ± ABS with LC reduced the mean total length of stay in hospital.
Introduction
Gallstones and alcohol use are widely reported as the most common causes of pancreatitis in the western world accounting for up to 80% of cases.1–3 Although 80% of cases of pancreatitis are mild and uncomplicated with a mortality rate of ∼1%, mortality is seen to be much higher in those with severe disease, being as high as 25% in those who develop infective necrosis.4,5 The British Society of Gastroenterology recommends that patients undergo laparoscopic cholecystectomy (LC) for acute gallstone pancreatitis (AGP) within 2 weeks, ideally during the index admission. 1
The wide variation of practice in the United Kingdom commonly involves a series of investigations in the form of magnetic resonance cholangiopancreatography (MRCP) to investigate for common bile duct stones (CBDS), followed by endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy if choledocholithiasis is demonstrated.6–9 This variation in practice is dictated by local policy and logistics.6–9 These preoperative investigations delay LC, imposing risks of recurrent pancreatitis and complications as a result of this.10,11
Our previous study has demonstrated the efficacy of simultaneous LC and intraoperative cholangiogram (IOC) ± antegrade biliary stent (ABS) through the cystic duct (CD) in the symptomatic gallbladder patients. This precludes patients for CBD exploration. 10
The aim of the study was to investigate the clinical feasibility of IOC ± ABS with LC in AGP, compared with preoperative biliary investigation and delayed LC.
Methods
Study design
A retrospective review on a prospective database that includes all the consecutive LC patients was taken. Subjects included in the study were divided into the following:
Single-stage IOC ± ABS at index admission. Preoperative biliary investigation and delayed LC at subsequent admission.
Subjects
All consecutive patients diagnosed with AGP managed with LC over a 34-month period (January 2016–October 2018) were included in the study.
Inclusion
All consecutive patients undergoing LC for AGP. AGP was diagnosed based on the British Society of gastroenterology recommendations. 1
Exclusion
For this study, patients with chronic gallstone pancreatitis and those with AGP from retained stones after LC were excluded from the analysis.
Outcomes
The primary outcome measure was the frequency of MRCP and ERCP investigations performed in each group. Secondary outcomes included length of hospital stay, morbidity, and mortality.
Follow-up
All patients were followed up for a minimum of 1 year from admission with AGP, with a median length of follow-up of 2.8 years.
Surgical technique
LC is performed using a standard four-port technique (10 mm umbilical, 10 mm epigastric, 5 mm anterior axillary, and 5 mm mid axillary line). 10 Calot's triangle is dissected ensuring the critical view of safety. Once the anatomy is delineated IOC is performed using an Olsen endoscopic cholangiography set (Cook Medical, REF G05927). A primed cholangiogram catheter (CC) (4.0F/43 cm) is inserted into the peritoneal cavity through a percutaneous cannula. The CD is clipped (Teleflex medical ref-003200) close to Hartmann's pouch and partially transected using scissors, allowing insertion of the CC under vision. If there is evidence of stone or debris in the CD, this is milked out through the incision in the CD.
Approximately 1 cm of the CC is inserted into the CD and a clip is placed to prevent leakage of contrast, initially confirmed with saline. IOC is performed using X-ray image intensifier while flushing a radiopaque dye (Lopamidol, Nefopam 300) through the CC. If CBDS are identified, a transcystic ABS is performed by first removing the CC and inserting an open-end flexi-tip ureteral catheter (7F, 70 cm; Cook Medical, REF G14809) through the cannula into the CD. A guidewire (Guide wire L, flexi-tip 3 cm, length 180 cm, 0.98 mm diameter; Terumo Europe Corp.) is carefully inserted through the ureteral catheter and advanced down the CBD into the duodenum under X-ray guidance.
Once satisfactorily positioned, the ureteral catheter is removed leaving the guidewire in place and a double pig tail end biliary stent (Zimmon Biliary stent, REF G22161, 7F, 4 cm; COOK Medical) is inserted over the guidewire, and advanced using a pushing catheter (Cook medical, 7F, 170 cm, G21774). Once stent position is confirmed, the guidewire is removed while maintaining the position of the pigtail using the pushing catheter. Final placement is established using X-Ray. After this, the clip and CC are removed before proceeding with clipping and cutting the cystic artery and completing cholecystectomy. Patients in whom a stent is inserted are booked for an elective ERCP for stent removal within 12 weeks of LC (Fig. 1).
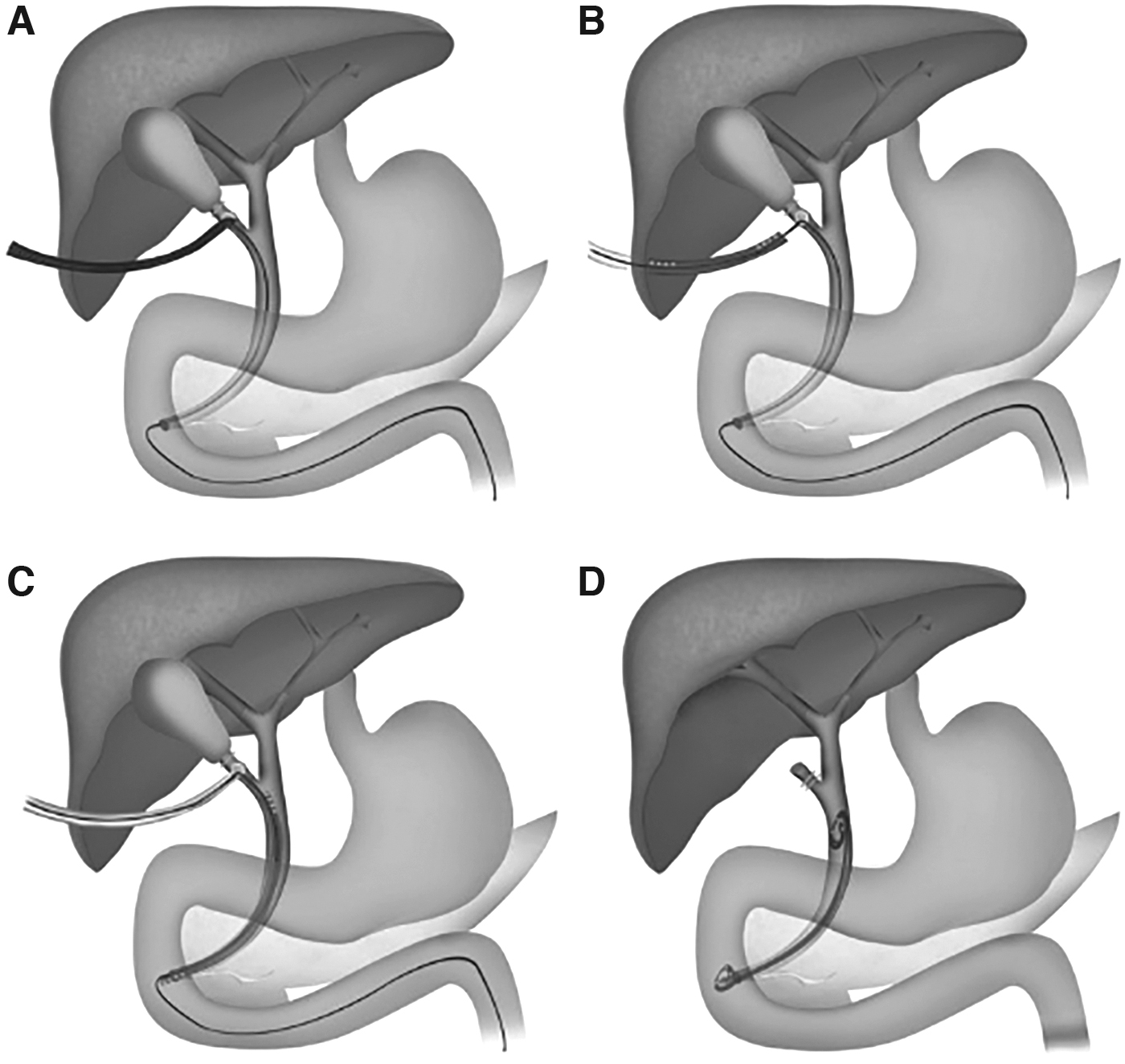
From Rehman et al.
10
Statistics
Simple descriptive and inferential statistics were used to generate the results. Categorical data were described using frequency and percentage. Continuous values were reported as mean ± standard deviation.
Ethics
Research Ethics Committee review was not required under the harmonized GAfREC for research, limited to the use of previously collected information nonidentifiable by researchers outside the usual care team. This exception also applies to research undertaken by staff within the care team using information previously collected in the course of care for the team's own patients, with the proviso that data are anonymized or pseudoanonymized in conducting the research. As such, this research involves no breach of the duty of confidentiality owed by care professionals (www.publichealth.hscni.net/sites/default/files/directorates/files/GAfREC_changes_Remit_REC_2011_08.pdf).
Results
We identified 301 patients diagnosed with acute pancreatitis during the 34-month study period. Gallstones were diagnosed as the etiology in 112 (37.2%) patients, alcohol in 102 (33.9%) patients, 53 (17.6%) patients were idiopathic, 9 patients (3%) developed pancreatitis post-ERCP, and the remaining 25 (8.3%) had other etiologies, including hyperlipidemia, medication, ERCP, ampullary malignancy, trauma, autoimmune, and viral (Table 1).
Causes of Pancreatitis in the Cohort of 301 Patients
ERCP, endoscopic retrograde cholangiopancreatography.
Of the patients with gallstone pancreatitis, 73 (65%) were female. The mean age was 56 years (SEM: 1.91). 104 (92.9%) patients were diagnosed based on a raised serum amylase, whereas the remaining 8 had a normal amylase but were diagnosed using CT scan. 38 (33.9%) patients were deemed unsuitable for LC based on comorbidities and functional baseline.
Of the 74 patients who underwent LC, 30 (40.5%) underwent simultaneous IOC ± ABS insertion during their index admission, whereas the remaining 44 (59.5%) patients were discharged and underwent cholecystectomy at a later date (Table 2).
Comparing Patient Data on Those Who Underwent IOC ± ABS Versus Those Who Did Not Undergo IOC and Instead Had Preoperative Investigations
IOC, intraoperative cholangiogram;
LC with IOC ± ABS
30 (40.5%) patients underwent simultaneous IOC ± ABS with LC and 11 required ABS insertion. The mean age was 49 years (SEM: 3.3) and 70% were female. The median admission bilirubin was 24.5 (IQR: 46).
The number of patients undergoing ERCP was 0 (0%) and MRCP was 2 (6.7%).
No patients were readmitted with AGP or symptomatic gallbladder.
The mean number of days between admission and time to LC + IOC ± ABS was 5.3.
Mean length of total hospital admission days including index admission and any postoperative complications was 10.1 days.
There were no patients in which IOC was not technically feasible.
Complications
2 (6.7%) patients developed a collection postoperatively and were managed with USS-guided drainage without further complication. One of these patients also developed a pulmonary embolism and hospital-acquired pneumonia requiring anticoagulation and antibiotics during their admission. 1 (3.3%) patient developed a postoperative intra-abdominal hematoma, which was managed accordingly.
Preoperative MRCP/ERCP with delayed outpatient LC
44 (59.5%) patients underwent delayed outpatient LC with preoperative biliary investigation. The mean age was 51 years (SEM: 2.5), 70.5% were female. The median admission bilirubin was 24 (IQR: 33.5). In this cohort, 7 (15.9%) patients underwent ERCP and 19 (43.2%) underwent MRCP. Mean length of total hospital admission days, including index admission, admission for LC, and postoperative admissions, was 13 days.
In this cohort 16 (36.3%) has IOC performed at the time of surgery. Of these patients, 4 (25%) showed stones on this imagining modality. There was only 1 patient in which IOC was not technically feasible.
9 (20.5%) patients were readmitted with pancreatitis. Five of these patients had two readmissions with pancreatitis. 5 (11.4%) patients were readmitted with a symptomatic gallbladder. In total, there were 19 readmissions in this group.
Complications
In this cohort 1 patient (2.3%) developed a bile leak requiring ERCP and stent insertion with antibiotics and subsequent ERCP to remove the stent. 1 patient (2.3%) developed a superficial surgical site infection, which required opening and packing of the wound. 1 (2.3%) patient developed urinary retention postoperatively requiring catheterization and commencement of alpha-blockade before discharge. 1 patient (2.3%) developed a postoperative hemorrhage and required laparotomy.
Discussion
Our pilot study has demonstrated the feasibility of performing simultaneous IOC ± ABS with LC in acute pancreatitis. We demonstrated that patients who underwent preoperative investigations with delayed LC were at risk of developing recurrent AGP and symptomatic gallstone disease.
The data demonstrate that simultaneous IOC ± ABS with LC reduces the number of MRCP/ERCP investigations required in the management of AGP. There was an overall 15.9% reduction in use of ERCP and a 36.5% reduction in use of MRCP by performing simultaneous IOC ± ABS with LC.
It is important to note that two patients in the simultaneous IOC ± ABS with LC cohort also underwent MRCP, this was due to local variation of practice. The two MRCP investigations performed reported presence of cholelithiasis but no CBD stones. At time of IOC, this surgical technique demonstrated the presence of CBD stones in these patients and ABS was subsequently inserted.
By reducing the number of preoperative MRCP/ERCP required in AGP, the patient's risk of recurrent pancreatitis is reduced and LC can be expedited. It has been demonstrated in studies that preoperative ERCP can leave patients with residual stones, resulting in a further postoperative ERCP being performed. 12 This cumulatively adds to the risk of perforation, pancreatitis, and bleeding. 11
Thacoor et al demonstrated that the need for MRCP is negated by taking the patient directly to theater for IOC thereby reducing cost of treatment and improving the patient flow. 13 There is benefit that must be noted of IOC being superior to MRCP in the detection of CBD stones and helping to delineate anatomy, providing a role in the avoidance of bile duct injury.14–16
Simultaneous IOC ± ABS with LC has been documented as a single-stage technique for investigation and management of CBD stones with concurrent definitive management of cholelithiasis. 10 Rehman et al demonstrated this technique to be a safe and cost-effective treatment option for routine use during LC to ensure no CBD stones persist; this reduces the number of ERCPs required, while defining anatomy and playing a role in reducing bile duct injury.10,13 The data in this study further support the use of this technique in the treatment of AGP.
The surgical technique for IOC ± ABS used in this study has the benefit of being a feasible option for district general hospitals as specialist expertise and equipment are not required. 10 When performed as part of a surgeon's routine practice, IOC ± ABS increases operative time by an average of 5 minutes and saves £1,195.05 when the additional instrument and radiographic cost is compared with performing ERCP. 10 The cost of direct access magnetic resonance imaging in the NHS is £178. 17 The cost of imaging must also be combined with the additional cost incurred by extending length of stay in hospital while awaiting investigation. For patients needing LC as definitive treatment the average cost is £279 per day. 18
As we have demonstrated in our study, there is a reduction in mean length of stay of 2.9 days in the IOC ± ABS cohort. This translates to an average cost of £809.10 per patient independent of additional imaging costs.
The patients in this data set were consecutive patients admitted over several years reducing the risk of selection bias in this cohort study. The demographics and admission biochemistry of the two cohorts in this study were comparable, further demonstrating strength in this study. Furthermore, we have provided data looking at the use of this technique specifically in AGP, providing a clear comparison of the two treatment strategies within this patient group.
Conclusion
In our pilot study we have demonstrated that performing simultaneous IOC ± ABS with LC is a feasible and beneficial management option when treating AGP in the setting of a secondary care center. We have demonstrated that by delaying LC the patient is at risk of developing recurrent AGP and GS disease. There is a reduction in the number of preoperative investigations required thereby reducing cost along with associated risks and complications. Simultaneous IOC ± ABS with LC, therefore, has a positive impact on both the patient and the hospital.
Authors' Contribution
I confirm that all authors listed contributed to the production of this article. The order of the authors accurately represents the contribution to the article.
Footnotes
Disclosure Statement
All authors declare they have no conflict of interest.
Funding Information
There was no funding for this research.