
Abstract
Background:
Minimally invasive surgery (MIS) is increasingly used for repair of congenital diaphragmatic hernia (CDH). Reported recurrence after MIS repair varies and is limited by short follow-up and low volume. Our objective was to compare recurrence after MIS versus open repair of CDH.
Materials and Methods:
Infants who underwent CDH repair between 2010 and 2020 were identified using the PearlDiver Mariner database, a national patient claims data set allowing longitudinal follow-up of patients across systems. Kaplan–Meier analysis and Cox proportional hazards regression models were used to evaluate the association of surgical approach (MIS versus open) and use of a patch with time to recurrence while adjusting for comorbidities (congenital heart disease and pulmonary hypertension) and length of stay (LOS).
Results:
In a cohort of 629 infants, 25.6% (n = 161) underwent MIS repair with a median follow-up of 4.8 years and recurrence rate of 38.6% (n = 243). Rates of recurrence after MIS repair were lower than open (5 years: 38.6% versus 44.3%; P = .03) and higher with use of patch (5 years: 60.1% versus 40.1%; P = .02). After adjustment for comorbidities and LOS as a proxy for patient complexity, there was no significant difference in recurrence based on approach (adjusted hazard ratio [aHR]: 0.79; confidence interval [95% CI]: 0.57–1.10; P = .16) or use of patch (aHR: 1.22; 95% CI: 0.83–1.79; P = .32).
Conclusions:
Recurrence rates after repair of CDH were not different based on surgical approach or use of patch after adjustment. Previous data were likely biased by patient complexity, and surgeons should consider these factors in determining approach.
Introduction
Minimally invasive surgery (MIS) for repair of congenital diaphragmatic hernias (CDHs) has become increasingly used since first described in 1995. 1 A recent survey from an international cohort of surgeons demonstrated that 52.1% would choose an MIS approach with thoracoscopic preferred to laparoscopic. 2 Despite increasing use, there remain numerous controversies regarding application of MIS approaches versus open. 3 Suggested advantages to MIS repairs include improved stability of intraoperative hemodynamics, decreased duration and amount of postoperative ventilation, faster recovery to enteral feeds, improved cosmesis, generally fewer complications, and lower death rates.4–7 Potential disadvantages are increased intraoperative hypercapnia, acidosis, and difficulty with the use of mesh for larger defects. 4
Reported recurrence rates after CDH repair have varied greatly from 4% to 48% for MIS repairs and 0% to 16% for open repairs in recent studies.8–10 The three largest metanalyses have all found an increased incidence of recurrence after MIS repair as compared with open.6,7,11 In addition, two of the largest studies to date from the CDH Study Group that each included several thousand patients also demonstrated higher rates of recurrence after MIS repairs.9,12 There is concern, however, that these data may be misleading and recurrence may be similar as center experience increases.
We, therefore, used a large national patient claims database, PearlDiver Mariner, to determine real-world outcomes after these approaches. Our objectives were to determine whether approach (MIS versus open) and technique (use of patch) impacted rate of recurrence after CDH repair in infants. Our hypothesis was that rate of recurrence after MIS repair would be no different than open repair on account of incorporating long-term follow-up and increasing utilization and familiarity with MIS techniques by surgeons. Moreover, that use of a patch would be associated with increased recurrence given likely greater size and complexity of repair.
Materials and Methods
The PearlDiver Mariner Patient Claims Database (PearlDiver Technologies, Colorado Springs, CO) is a national all-payer medical and surgical claims database that provides HIPAA-compliant patient information for research purposes. The database is constantly growing with quarterly updates—at time of data collection it included 91 million patients from 2010 to 2020. The database is derived from commercial, Medicare, and Medicaid claims from various provider networks, including academic institutions, children's hospitals, and community hospitals. Providers who supply the claims data are required to contract with independent third parties to conduct audits on the validity and reliability of the data.
All claims within the data set are adjudicated and are regularly subject to audit policies and internal review. The major benefit of this database is the ability to follow patients between separate hospitalizations or insurance changes using unique patient identifier codes, which allows for time-specific longitudinal research while also keeping patient information de-identified. This database has been most published on in the orthopedic literature, but more recently has been used fields of general and pediatric surgery.13,14 The Rush University Medical Center Institutional Review Board provided protocol exemption for this study.
Patients under the age of one who underwent CDH repair through either an MIS or open approach were identified through the Mariner database using appropriate International Classification of Diseases (ICD) procedure codes (Supplementary Table S1). Patients who had ICD-9/10 procedure codes listed for both MIS and open approaches in the same record were excluded.
The primary outcome was time to hernia recurrence requiring reoperation. Recurrence was defined as patients who underwent a second surgical repair after the first based on ICD-9/10 procedure codes. The primary exposures of interest were surgical approach (MIS versus open) and technique (use of a patch versus no patch) determined by ICD-9/10 procedure codes. Additional demographic and clinical variables collected included patient sex, region, insurance plan, comorbidities, length of stay (LOS), and length of follow-up.
Comorbidities, which included congenital heart disease (CHD) and pulmonary hypertension (PHTN), were identified using ICD-9/10 diagnosis codes (Supplementary Table S2). CHD included major cardiac defects as defined by the Congenital Diaphragmatic Hernia Study Group: atrioventricular septal and canal defects, tetralogy of Fallot, coarctation of the aorta, hypoplastic left heart, and double outlet right ventricle. 15 Length of follow-up was defined as time from the index procedure through the last submitted claim included in the database for each patient.
Bivariate analysis comparing demographic and clinical characteristics by surgical approach was performed using Wilcoxon rank-sum test for continuous variables and chi-squared test for categorical variables. Kaplan–Meier analyses and Cox proportional hazards regression models were used to determine association between time to recurrence and key exposures of interest including surgical approach (MIS versus open) and technique (patch use versus no patch use). A Cox proportional hazard model including all key exposure variables while adjusting for CHD, PHTN, and LOS was then performed.
A P value of <0.05 was used to define statistical significance and all tests performed were two-sided. Statistical analyses were done using the PearlDiver Mariner interface, which employs R software (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 629 infants were identified who underwent CDH repair between the years 2010 and 2020 (Table 1). Seven patients were excluded for having both open and MIS codes at initial repair, implying a procedural conversion, or coding failure. MIS techniques were used in 161 cases (25.6%) and open repair performed in 468 (74.4%). A patch was used in 94 cases (14.9%). There was no variation in surgical approach based on sex, region, or plan type. CHD was present in 93 (14.8%) of patients, and 228 (36.2%) of patients had PHTN. Patients with CHD and PHTN were more likely to undergo open procedures. Patches were used more commonly in open repair compared with MIS (n = 81 [17.3%] versus n = 13 [8.1%]; P < .01). LOS was longer after open versus MIS repair (26.0 days versus 11.5 days; P < .01). Median patient follow-up was 4.8 years (interquartile range [IQR]: 2.1–7.1) with no difference in length of follow-up based on surgical approach (4.4 [IQR: 2.0–7.2] versus 5.0 [IQR: 2.1–7.1] years, P = .60).
Characteristics of Patients Who Underwent Congenital Diaphragmatic Hernia Repair by Minimally Invasive Versus Open Approach
Continuous variables are presented as median (IQR), whereas categorical variables are presented as frequency (percentage). Chi-squared test was used for categorical variables, and Wilcoxon rank-sum test was used for continuous variables.
CHD, congenital heart disease; LOS, length of stay; MIS, minimally invasive surgery; PHTN, pulmonary hypertension.
Overall rate of recurrence was 38.6% (n = 243). Rate of recurrence after MIS approaches was lower than open repair at 1 year (26.1% versus 36.4%), 3 years (34.4% versus 43.4%), and 5 years (36.6% versus 44.3%; Fig. 1 and Table 2). Use of a patch was associated with a higher risk of recurrence at 1 (39.7% versus 32.8%), 3 (56.1% versus 39.0%), and 5 years (60.1% versus 40.1%; Fig. 2).
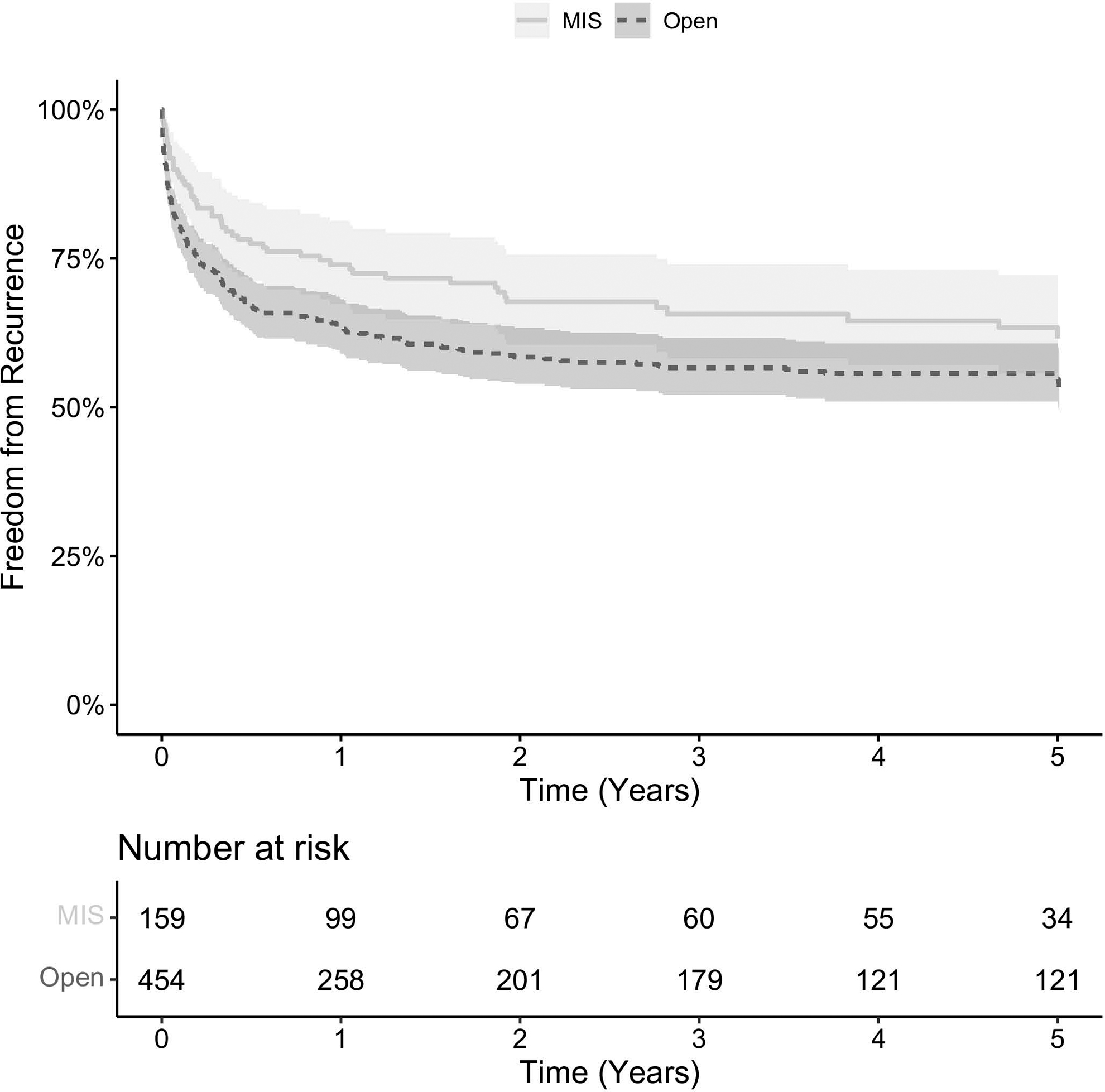
Approach and time to recurrence after repair of congenital diaphragmatic hernia. MIS, minimally invasive surgery.
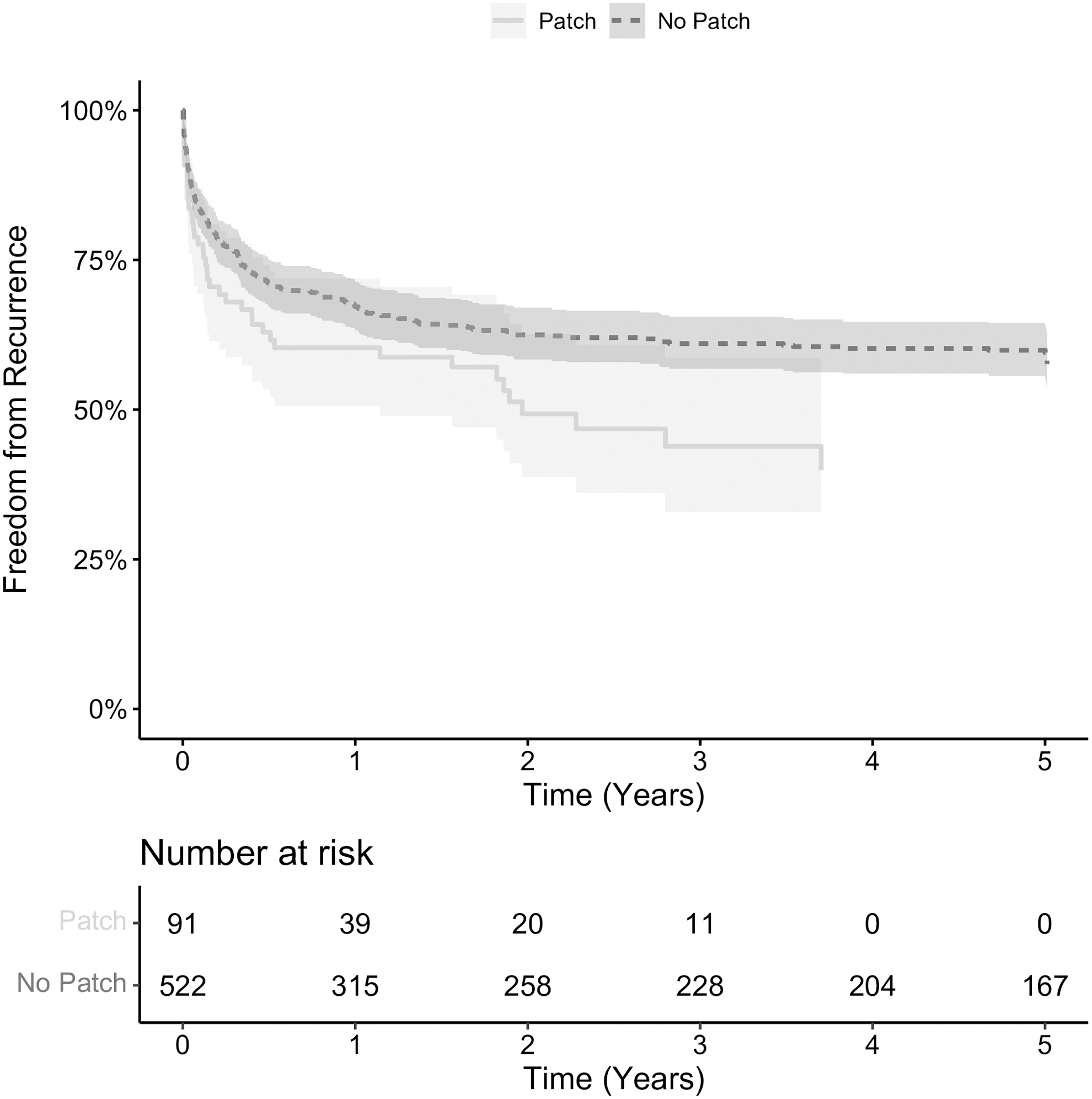
Patch use and time to recurrence after repair of congenital diaphragmatic hernia.
Rate of Recurrence After Repair of Congenital Diaphragmatic Hernia by Approach, Technique, and Comorbidities
P value determined based on overall log-rank tests rather than individual time points.
CHD, congenital heart disease; IQR, interquartile range; MIS, minimally invasive surgery; PHTN, pulmonary hypertension.
After adjustment for comorbidities and LOS, there was no difference in risk of recurrence after MIS versus open repair (adjusted hazard ratio [aHR]: 0.79; confidence interval [95% CI]: 0.57–1.10; P = .16) or use of patch (aHR: 1.22; 95% CI: 0.83–1.79; P = .32) (Table 3). Risk of recurrence was higher in patients who had CHD (aHR: 2.16; 95% CI: 1.57–2.98; P < .01) and PHTN (aHR: 1.35; 95% CI: 1.01–1.80; P = .05).
Clinical and Technical Factors Associated with Risk of Recurrence After Congenital Diaphragmatic Hernia Repair
CHD, congenital heart disease; CI, confidence interval; HR, hazard ratio; IQR, interquartile range; LOS, length of stay; MIS, minimally invasive surgery; PHTN, pulmonary hypertension; Ref, reference.
Discussion
Many have criticized the use of MIS approaches for repair of CDH due to historically high rates of recurrence; however, there is concern that these studies evaluated outcomes early in the adoption of MIS approaches and may not demonstrate real-world use of this technology in experienced hands. Furthermore, there is likely selection bias as surgeons are much more likely to operate on smaller hernias through a minimally invasive approach, which would be associated with lower recurrence rates. We queried a large national claims database with the ability to evaluate patients across multiple admissions at different institutions with the goal of better characterizing recurrence after MIS repair. 13
We found that recurrence rates were actually lower after MIS repair before adjustment for use of patch and comorbidities. Once we adjusted for these factors, there was no difference in recurrence based on approach or use of patch, contrary to findings from many smaller single center studies. This adds to the current literature as it gives a more complete understanding of what is happening by incorporating data from a variety of centers and following children for a longer period of time.
A large range of recurrence rates after MIS repairs of CDH have been reported and are generally higher than open. Rates as high as 48% have recently been described, and metanalyses also support higher recurrence after MIS repair.6–8,11 The exception are a few small retrospective studies.16,17 The two largest studies to date that focused on MIS versus open repair were through the CDH Study Group and suggest that rates of recurrence are higher after MIS repair.9,12 Although their database is built from patient data at a wide range of hospitals, it is limited by only including follow-up through the initial hospitalization.
Our data contradict the literature and demonstrate a possible trend toward decreased recurrence after MIS repair as experience grows. One of the strengths of the Mariner database is the ability to follow patients for a long period of time and across institutions. Having long-term follow-up in this population is key as one center demonstrated that whereas 70% of recurrence occurred before 2 years, 17% continued to occur after 4 years. 18 This cohort uniquely encompasses a wide range of hospitals with median follow-up of 4.8 years, which may explain the discrepancy with current literature.
Increased adoption of MIS techniques offers another potential explanation for the lower rates of recurrence in this study as compared with previous literature. Based on recent surveys, MIS techniques are now preferred by up to 52.1% of pediatric surgeons for initial repair of CDH. 2 This is reflected in the increased proportion of patients who underwent MIS repair in this study (25.6%) as compared with previous large national cohorts that had rates of 3%, 5%, and 16%.8,12,19 The CDH Study Group demonstrated that within their clinical registry from 2007 to 2015, although recurrence was initially higher after thoracoscopic repair, recurrence became approximately the same as open for the final 4 years of the study period. 9
The potential for improvement over time were also illustrated through a single institution quality improvement initiative that incorporated improvements in technique successfully halved rates of recurrence after thoracoscopic repair. 20 Beyond improvements in surgeon technique leading to progression beyond the learning curve, other factors such as improved patient selection and collaborative care must also be considered as contributing to these decreased recurrence rates. 9,19 This collective experience gained from a center performing more cases through MIS approaches is one potential contributor to the demonstrated reduced rates recurrence.
Prior studies have suggested that patch repair may be an independent predictor of recurrence. 21 Although early studies showed that recurrence may be highest when patches are used in combination with an MIS approach,7,12 more recent study suggests that patch use may not be associated with recurrence after adjustment for other factors. 22 One challenge when studying different approaches and techniques in infants who have undergone CDH repair is that clinical status, hernia size, and comorbidities likely contribute to and bias selection of technique. Centers often have specific criteria for patients to qualify for MIS repair. 4 These may vary widely, but for example one center's primary criteria for MIS repair is stable CDH with a low fraction of inspired oxygen (FiO2), no PHTN, and no liver in the hernia defect suggesting possibility for primary repair. 4
As most centers have some level of selection criteria, this implies that those who undergo MIS repair may generally be better surgical candidates with smaller defects that would not require patch repair and less pulmonary hypoplasia. In this study, we found that patient comorbidities rather than use of a patch had greater association with recurrence. Although historically patch use and approach may have been associated with recurrence, this suggests that improved patient selection regarding both approach and technique may also contribute to reduced rates of recurrence.
This study does have limitations. Generally, large databases lack granularity that affects the scope of the study. We were unable to determine hernia type (Bochdalek versus Morgagni) or complexity of repair (such as size and presence of liver within the hernia) through use of billing codes. This may affect recurrence as factors such as defect size have been shown to increase risk of recurrence. Most of the existing multi-institutional studies have excluded Morgagni hernias, and rate of recurrence after repair of Morgagni hernias in infants remains largely uncharacterized. If recurrence or use of laparoscopic versus thoracoscopic approach varies widely between Bochdalek and Morgagni defects, this may have impacted our results.
Although we were unable to determine defect size directly, prior studies have similarly included use of patch as a proxy for defect size when this information is unavailable.9,18 The type of material used in patch repair may affect rate of recurrence, which was also unable to be determined for this study. 21 Large patch repairs are often considered higher risk for recurrence, and these are most commonly done open, which may bias the results. 17 Finally, PearlDiver Mariner is an all-payer database that captures claims from a wide variety of networks including academic and community hospitals. There may be significant variation among centers in staff experience and available resources that we are unable to delineate using the available data, which may contribute to recurrence after repair.
Conclusion
Evaluating recurrence after use of MIS versus open techniques for CDH repair has historically demonstrated higher rates of recurrence after MIS repair. This study utilized a large national database with a median follow-up of 4.8 years and found that rates of recurrence were not significantly different between MIS and open repair or with use of patch after adjustment for patient comorbidities. Further work should focus on determining optimal patient selection for MIS approaches. In the interim, patient complexity and characteristics of the hernia defect should continually be considered when selecting surgical approach.
Footnotes
Authors' Contributions
Conceptualization, methodology, software, formal analysis, and writing—original draft by G.A.S. Methodology and writing—review and editing by N.J.S. Data curation and writing—original draft by J.K. Formal analysis, data curation, and writing—review and editing by G.O. Conceptualization, writing—review and edit, and supervisions by S.P., M.B.M., A.N.S., and B.C.G.
Acknowledgments
We would like to thank Jeff France of Pearl diver and Adan Becerra of Rush University Medical Center for continued assistance using the Mariner data base.
Disclosure Statement
B.C.G. serves on the advisory board of Pacira Biosciences; this relationship had no impact on this research. No other authors have disclosures.
Funding Information
This project was funded internally by the Rush University Medical Center Department of Surgery. Also, no external funding was received.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.